


Abstract
Bilateral synchronous breast cancer is extremely rare. A 75-year-old man presented with a right breast mass, which ulcerated and a lump in the left breast. Right breast examination revealed a breast ulcer 7×10cm with everted edges and complete nipple destruction. The left breast showed a hard lump measuring 4×5cm in the nipple-areolar area, unattached to skin, or underlying structure. There was no palpable axillary lymph node bilaterally. A wedge biopsy of right breast ulcer and excision of the left breast lump confirmed bilateral invasive ductal carcinoma - Grade 2 tumor in both breasts. He had bilateral simple mastectomy and chemotherapy; defaulted for 18 months during treatment, and re-presented with bilateral tumor recurrence. The importance of this case report is to create more awareness that breast cancer can occur in males just as in females, though the incidence is rare in males. Early presentation and compliance with treatment modality provide a better outcome.
Male breast cancer is rare in men and accounts for 1% of all breast cancers.1 A bilateral synchronous presentation is extremely rare with an incidence of 1-2.5% of the total number of patients with breast cancer.2 Bilateral breast cancer is defined as the presence of an independent primary malignant tumor in each mammary gland. The term “synchronous” refers to the presence of primary tumors in both breasts, which are diagnosed simultaneously.3 The incidence of metachronous breast cancer is higher than that of synchronous male breast cancer.4 Most cases of male breast cancer are detected between the ages of 60 and 70 with a mean age of 67 years which is older than the mean age of females.5 The risk factors for male breast cancer include familial and genetic factors (BRCA2), radiation exposure, Klinefelter’s syndrome, hormonal imbalance, obesity, and testicular disease (undescended testis, orchitis, orchectomy).1 Although breast cancer in males presents in a similar way to that of females, there is limited data regarding treatment of male breast cancer, and most treatment recommendations are extrapolated from data in women.6 Male breast cancer tends to be diagnosed at an older age, and at a more advanced stage than female breast cancer; hence, the overall survival rate is lower in males.7 However, outcomes are comparable when age at diagnosis and stage are adjusted.5 This study examines a 75-year-old man who was diagnosed with bilateral synchronous male breast cancer; he had bilateral simple mastectomy and chemotherapy; then defaulted for 18 months during treatment and re-presented with bilateral tumor recurrence. Our objective in presenting this case is to highlight that breast cancer can occur in males just as in females, though the incidence is rare in males. Early presentation and compliance with treatment modality provide a better outcome.
Case Report
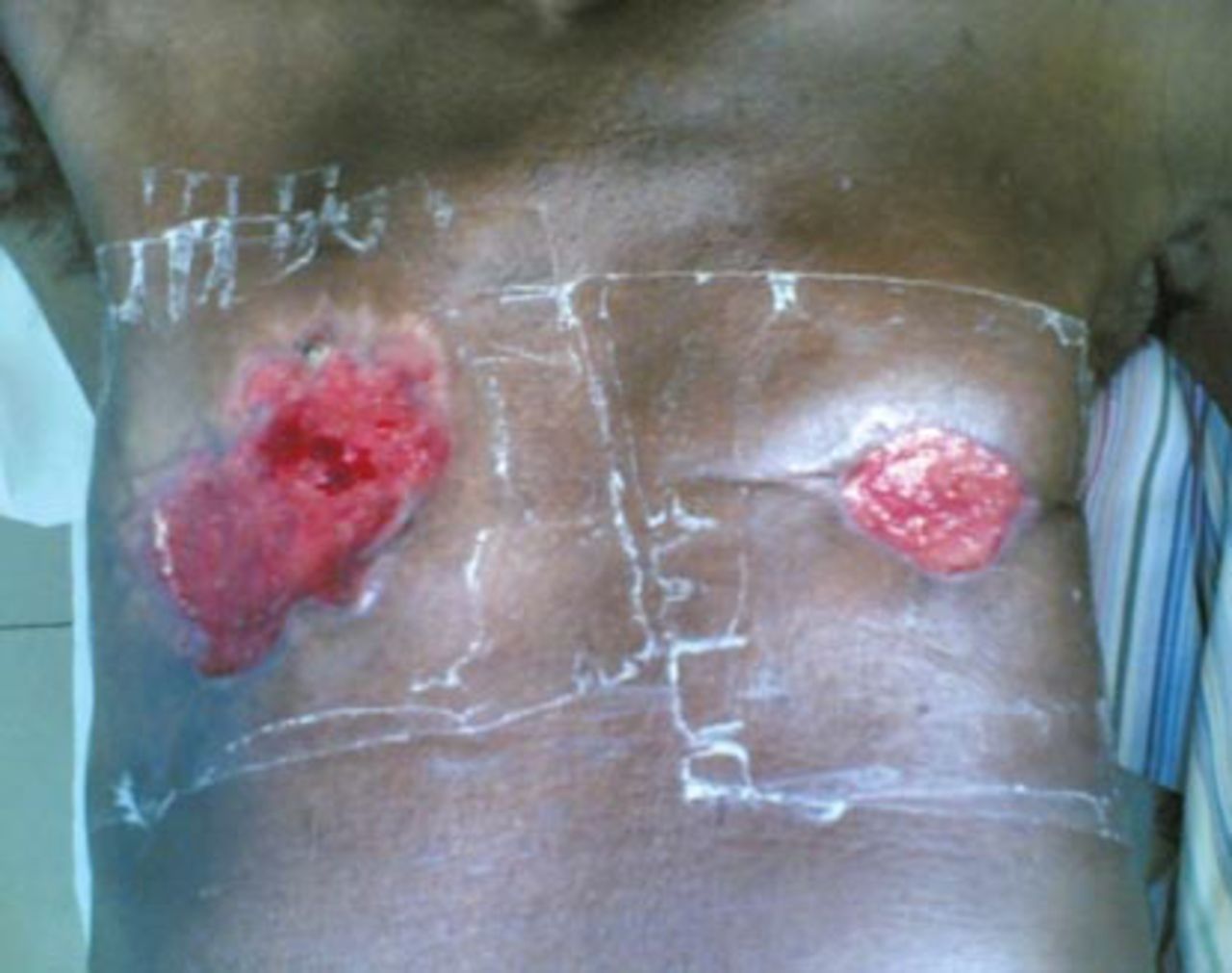
Our patient is a 75-year-old man who noticed a lump in the right breast 2 years prior to presentation. The lump was initially small in size, painless, but progressively increased in size. Following massage and application of herbal medication, the lump ulcerated with complete nipple destruction (Figure 1). Around the same time he noticed a lump in the right breast, he felt a small lump in the left breast, which was the size of a bean seed, painless, and progressively increased in size. There was no history of nipple discharge, ulcer, or itching of the left breast. There was no antecedent history of trauma to both breasts and no family history of breast disease/malignancy. He had no history of cough, chest pain, night sweats, weight loss, or difficulty in breathing. There was no history of abdominal pain/swelling, yellowness of the eyes, bone pain, or low backache. He drank 2 bottles of alcohol daily for approximately 30 years, and smoked a pack of cigarette daily for 9 years. General examination revealed an elderly man, chronically ill-looking, not pale, afebrile, anicteric, not dehydrated, with neither pedal edema, nor peripheral lymph node enlargement. The right breast examination revealed an ulcerated breast with complete nipple destruction. The ulcer measured 7 × 10 cm with everted edges, non-tender with sloughs on the floor, and hypo/hyper pigmented surrounding skin. The left breast showed a hard lump measuring 4 × 5cm in the nipple-areolar area with no differential warmth, non-tender, and unattached to skin or underlying structure. There was no palpable axillary lymph node bilaterally. The examinations of other systems were essentially normal.

Picture at presentation showing ulcerated right breast with complete nipple destruction and a left breast lump.
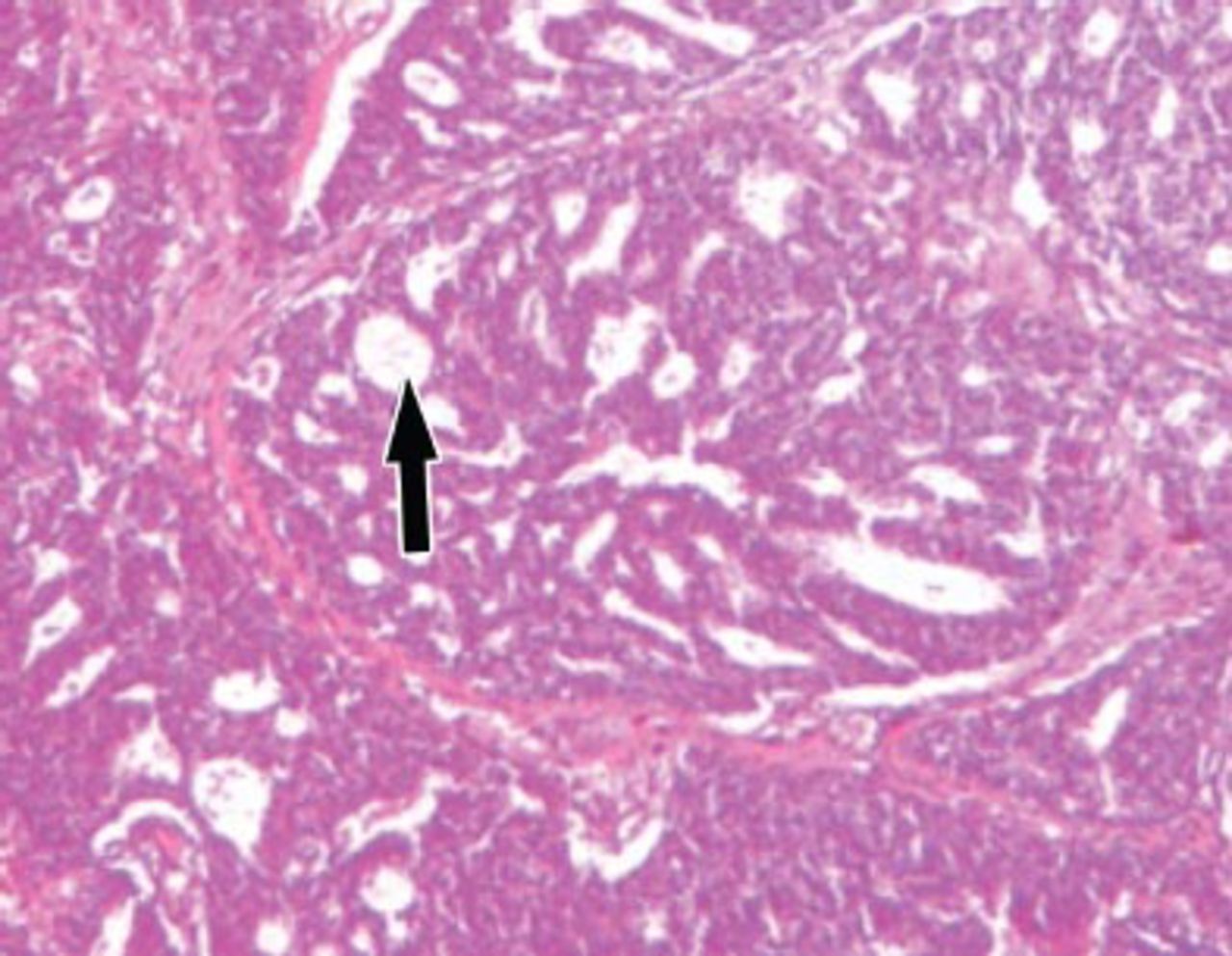
Full blood count, random blood sugar, electrolytes, urea and creatinine carried out were normal. An abdominal ultra-sonography and chest radiograph did not reveal features of metastasis. The tumor-lymph node-metastasis (TNM) staging was T4bN0Mx in the right breast, and T3aN0Mx in the left breast. A wedge biopsy of the right breast ulcer and excision biopsy of the left breast lump confirmed a bilateral invasive ductal carcinoma (Figures 2 & 3). Sections of both breasts show a malignant neoplastic lesion composed of malignant ducts, sheets, and nests of atypical polygonal epithelial cells with invasion of the stroma and surrounding tissues by these cells. These cells have large ovoid to round hyperchromatic nuclei with numerous abnormal mitosis. Both breast tumors were grade 2 (Nottingham modification of Bloom-Richardson breast cancer grading system). The estrogen, progesterone, and Her-2-neu status were not carried out due to lack of facilities; hence, he was neither treated with tamoxifen nor Trastuzumab (Herceptin).

Left breast: invasive ductal carcinoma. Arrow shows focal area of mucin between sheets of malignant cells.

Right breast: invasive ductal carcinoma. Arrow shows sheets of malignant cells surrounded by desmoplastic stroma.
He had bilateral simple mastectomy without axillary dissection because there was no palpable axillary lymph node (Figure 4). In addition, axillary lymph node dissection in advanced breast cancer is not advocated, as it does not improve the overall survival. He had 2 cycles of Cyclophosphamide, Adriamycin, and 5-flourouracil chemotherapy regime. He defaulted after the second cycle of chemotherapy for 18 months and represented with bilateral tumor recurrence (Figure 5), marked weight loss, and ascites. He is presently being worked up for chemotherapy.

Picture after bilateral simple mastectomy.

Tumor recurrence after patient defaulted from treatment for 18 months.
Discussion
Bilateral breast cancer is defined as the presence of an independent primary malignant tumor in each mammary gland while the term “synchronous” refers to the presence of primary tumors in both breasts, which are diagnosed simultaneously.3 Our patient had tumors in both breasts on hospital admission. A total of 24 cases of synchronous bilateral male breast cancer have been reported as of August 2011 using a PubMed search.4 This corroborates the fact that the incidence of metachronous breast cancer is higher than that of synchronous.4 Although breast cancer can affect men of all ages, the median age at diagnosis is 60-70 years,2 which is in keeping with the age of 75 in our patient. Presentation is usually late with more than 46% of patients having stage III or IV of the disease at the time of diagnosis,8 which is similar to our case. This can be attributed to low awareness, absence of screening protocols in men, and limited amount of mammary tissue in male, thus allowing rapid local invasion.8 The most frequent histological type in men is invasive ductal carcinoma (85-90%),9 which is similar to the findings of our patient. Other rare invasive tumors are invasive papillary (4.5%) and mucinous (2.8%) papillary carcinoma. Although breast cancer in males presents in a similar way to that in females, there is limited data regarding treatment of male breast cancer, and most treatment recommendations are extrapolated from data in women.6 The mainstay of treatment is based on local and regional control of the disease with surgery.10 Other adjuvant therapies are chemotherapy, radiotherapy, and hormone therapy.10 This was similar to the treatment of our patient, which comprised simple mastectomy and chemotherapy, though he did not fully comply initially with the chemotherapy regime.
The prognosis of male breast cancer remains uncertain because of the late diagnosis, unpredictable course, and high potential for metastasis.11 The prognosis does not seem to be poor compared with females when age and stage are matched.11
The importance of this case report is to create more awareness that breast cancer can occur in males just like females, although it is rare in males. A painless lump, bloody nipple discharge, or retraction in a male, especially an elderly male, requires thorough evaluation and on confirmation of cancer, compliance with treatment modalities is necessary to ensure good outcome.
In conclusion, breast cancer is rare in males, and extremely rare is bilateral synchronous breast cancer. Early presentation and compliance with treatment schedule will help reduce the incidence of tumor recurrence and provide better prognosis for the patient.
References
* References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
* Unpublished data and personal communications should be cited only in the text, not as a formal reference.
* The author is responsible for the accuracy and completeness of references and for their correct textual citation.
* When a citation is referred to in the text by name, the accompanying reference must be from the original source.
* Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
* Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from:
Acknowledgment
Dr. Ezekiel E. Ugiagbe reviewed the slides for clarity and correctness.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 28, 2014.
- Accepted November 26, 2014.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.