


Abstract
Pulmonary agenesis is a very rare congenital abnormality that can be missed in a routine radiographic examination, which delays diagnosis until adulthood. It can be associated with other congenital malformations, such as valvular heart disease and gastrointestinal organ abnormalities. Computed tomography (CT) is a useful modality for its better delineation of pulmonary and vascular structures. The reported case here is for an adult male who presented with dextroposition of the heart and was found to have a unilobed right lung associated with polysplenia. This has not been previously reported in the literature.
Introduction
Congenital pulmonary anomalies are rare malformations that can range from hypoplasia to complete agenesis involving the entire lung or just a part of it. For instance, such anomalies can include absence of the pulmonary artery, bronchus or lung parenchyma. Pulmonary agenesis is an extremely rare congenital abnormality resulting from a failure to develop the primitive lung bud.1,2 The diagnosis of pulmonary agenesis can either be isolated or be found in association with other congenital anomalies involving other organs, such as the trachea, esophagus, heart, vertebra, anus and limb. Multiple anomalies have been reported more frequently than single anomalies.3,4 Patients with right-sided agenesis are likelier to die before those with left-sided agenesis.5 Additionally, they do have a more frequent association with other congenital anomalies of different organs and tissues, with no identified reasons.6 Patients with pulmonary agenesis are usually diagnosed in the pediatric age group. However, some patients may present in adulthood, especially those with less severe disease or those with no associated anomalies. Our case is an example of such a patient who was referred to our centre in early adulthood after incidental findings on a chest x-ray of dextrocardia for further evaluation. To our knowledge, this is the first reported case of the association of polysplenia and the single right lower lobe of the lung with agenesis of the upper and middle lobes. We believe that such an association is quite rare and that it may be missed in routine chest radiographs.
Case Report
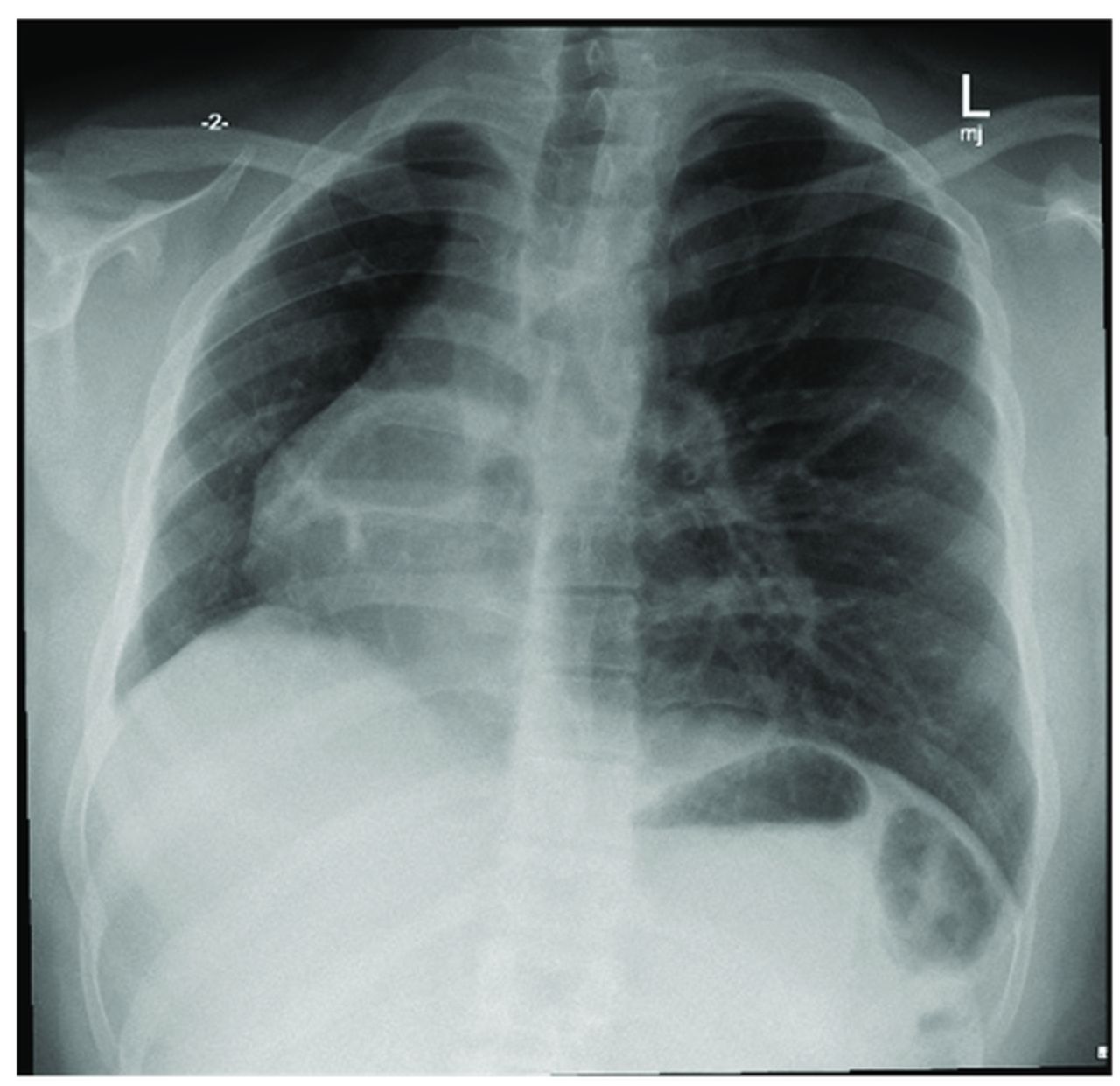
A 19-year-old, non-smoker male patient was referred to our clinic after incidental findings on his chest radiograph (Figure 1). The patient is a resident of a remote village in the eastern province of the Kingdom of Saudi Arabia.

- Chest radiograph showing dextroposition of the heart in the right hemithorax.
Clinical findings
He presented with a cough, sore throat and fever. No chest pain, anorexia or weight loss was noted. Additionally, no significant past medical history was documented. A physical examination revealed a right tracheal deviation. Asymmetrically decreased movement of the right side of the chest was noted. Additionally, the heart sounds were placed on the right.
Diagnostic assessment
A chest x-ray (CXR) was carried out to rule out pneumonia, and it showed no infiltrate but dextrocardia with mediastinal deviation to the right. Furthermore, a computed tomography (CT) scan of the chest showed a hypogenic right lung, which was composed only of the right lower lobe (Figure 2). The right pulmonary artery was tortuous and small in calibre. An abnormal orientation of the right bronchus to the right pulmonary artery with the right bronchus appeared hyparterial. A single right pulmonary vein was noted draining normally into the left atrium. Dextroposition of the heart and mediastinum were shifted to the right. An abdominal scan showed multiple spleens, suggestive of polysplenia. An echocardiogram was performed and confirmed normal heart function and structures with cardiac activity in the right infra-axillary area.

- Computed tomography (CT) angiogram. A) Axial cut showing a small tortuous right pulmonary artery (arrow) arising normally from the pulmonary trunk. B) Solitary pulmonary vein (the arrow) draining normally into the left atrium. C) Coronal cut showing right hyparterial unilobed bronchus is seen with a solitary lower lobe (the arrow) and agenesis of the upper and middle lobes. D) CT abdomen showing polysplenia (the stars).
Therapeutic intervention
The patient received conservative treatment and was instructed to return for regular follow-up.
Follow-up and outcomes
The patient is progressing well without any complications or additional health conditions.
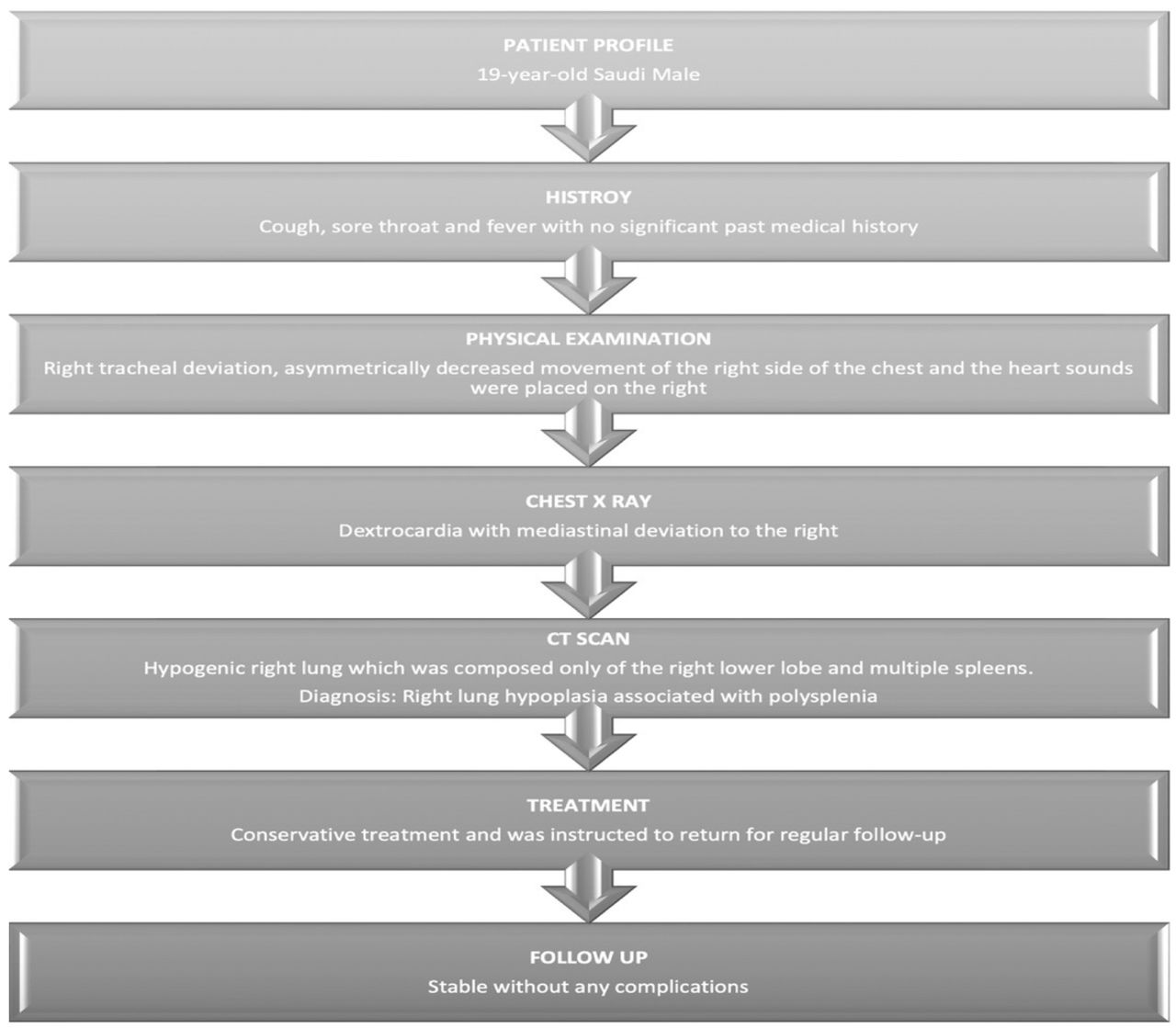
Timeline from the patient’s initial clinical presentation to follow-up appointments is shown in Figure 3.

- The timeline summarizes the patient’s initial presentation, chest x-ray, computed tomography scan, diagnosis, treatment and follow up.
Discussion
Lung hypoplasia is an extremely rare congenital defect in which part of the lung fails to develop. The condition has been estimated to occur in 30 thousand live births.7 Pulmonary agenesis can be solo or associated with other anomalies. It was initially classified by Schneider and then described in more details by Boyden.8 It has been categorized into 3 main types based on the degree of lung and bronchial involvement in the anomaly. The first is the complete absence of the lung and its structures from the bronchi and vessels on the same side. The second is a rudimentary airway with no lung tissue. The third is hypoplasia, where there is a presence of a variety of parts of the bronchus, pulmonary tissue and vascular supply.9 Lung agenesis occurs approximately before the fifth week of gestation when the lung buds are protruded from the foregut as a diverticulum.
Patients with pulmonary agenesis may have a healthy life or present with atypical symptoms, such as repeated pneumonia. Many patients, like ours, can be incidentally diagnosed with abnormal chest radiographs. Our case had no symptoms throughout his childhood until he presented with a simple upper respiratory tract infection when CXR was done and revealed dextrocardia. Following the CXR findings of dextrocardia, a chest CT was performed to identify an abnormality that showed that the right lung was not fully developed. Heterotaxy syndrome should be considered in patients with lung agenesis. The majority of cases are associated with bilobed lungs, liver transposition, congenital heart disease, azygous continuation of the inferior vena cava and polysplenia.10 Therefore, an abdominal CT scan was performed and revealed only polysplenia with other normal abdominal organs. Additionally, the echocardiogram showed normal heart structures. In pulmonary agenesis, prevention of recurrent infections is crucial because they can be life threatening. Fortunately, our patient did does not require long-term medical treatment. However, others may need bronchodilators and chest physiotherapy, for instance, depending on their symptoms and the presence of bronchiectasis.
In conclusion, pulmonary agenesis is a rare condition and can be mistaken for other pathological conditions. In this case report, the presentation of our case with an abnormal chest radiograph of dextrocardia, which was revealed by a CT scan, revealed lung hypoplasia. It is challenging to diagnose lung agenesis; however, physicians should consider it in the differential diagnosis of the dextroposition of the heart. Therefore, looking for other associated congenital anomalies is of paramount importance.
Acknowledgment
The authors gratefully acknowledg Scribendi Inc. for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 31, 2024.
- Accepted June 14, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.