


Abstract
Objectives: To understand the perceptions, attitude, and prescribing practices of clinicians regarding antimicrobial resistance (AMR).
Methods: A multidisciplinary cross-sectional study comprising 447 clinicians of university, public, and private hospitals of Jeddah, Saudi Arabia was carried out from August to October 2014 using a self-administered questionnaire.
Results: Interestingly, 33% of the general physicians yielded to patient/parent’s demand for the choice of antimicrobials (AMs) as compared with only 13.2% of the residents, and 4.3% of the specialists. In addition, expensive AMs are more often prescribed by the general physician (70.4%) in comparison with 26.4% residents and 30.4% of the specialists. However, no significant differences were observed between the knowledge and perceptions regarding the current scope of AM agents, as well as their use and misuse. Furthermore, dependability of specialist and residents seems to be significantly higher than general physicians on pocketbooks and smartphone for AM education sources.
Conclusion: This study revealed that despite a clear concept of AMR, general physicians lacks consistency in prescribing aptitude and use of effective educational resources, while all respondents lacks dedication to follow the guidelines of AM use. This highlights the requirement of AM stewardship with decisive objective of reduction in AMR.
Antimicrobials (AMs) have the uniqueness to provide radical curative treatment of infections, and by virtue of this fact, these medications have the capability of not only renovation of quality of life, but have also proven to be life saving in several severe infective conditions.1 Conversely, their confusing and inappropriate use has now lead to an intimidating outcome of antimicrobial resistance (AMR), which in turn, leads to failure in managing infectious disorders, escalation of morbidity and mortality, and impedes the advancement in health outcomes with staggering costs on healthcare providers as well as the society.2-5 Certain classes of drugs like antipsychotics and chemotherapeutic agents are exclusively prescribed by concerned specialists, while in contrast, AMs are enthusiastically prescribed by all clinicians, as well as the allied healthcare personnel irrespective of their knowledge or training concerning AMs.6 Not withstanding the worldwide spread of AMR with their devastating outcomes, and with equally valuable propagation of information to the healthcare team regarding the adversity of AMR, their misuse is still rampant.7 The World Health Organization recommended the necessity of educating the healthcare team to revamp and curb the irrational antimicrobial prescribing with an overall objective of averting potential AMR.8,9 An inapt prescription pattern of AMs was detected in the range of 24-80% of the patients attending a community hospital in Saudi Arabia.10 A recent local study11 highlighted AMR as a major health problem, and noncompliance is one of the major contributory factors. Similarly, another recent study12 demonstrated that in comparison with students of other health sciences, pharmacy students had a clear concept of theoretical knowledge of AMR and cautious use of AMs. Correspondingly, a recent survey13 conducted among the young university graduates in Saudi Arabia demonstrated a pessimistic perspective regarding the levels of their perception of antimicrobial use. An alarming condition of pan-resistant Acinetobacter baumannii is emerging in Saudi Arabia,10,14 and also significant high resistance rates of non-fermenters is prevalent in Saudi Arabia.15 Any educational intervention of clinicians, either concerning antimicrobial utilization or AMR is apparently an utter failure without taking into consideration their comprehension and attitude towards AM.1 Consequently, to explore the motivation behind the cause of disproportionate antimicrobial prescription, it is essential to evaluate the knowledge, attitude, and prescribing practice.1,16 To tackle the development of AMR, and to facilitate the clinician’s attempt to efficiently take care of their patients, global antimicrobial stewardship programs are extensively developed. Yet, such efforts in Saudi Arabia were carried out only in dentistry.1 It is an important observation that studies related to AMR in Saudi Arabia until now did not cover knowledge and perception of clinicians,10-15 and this persuaded us to execute or carry out this study.
Methods
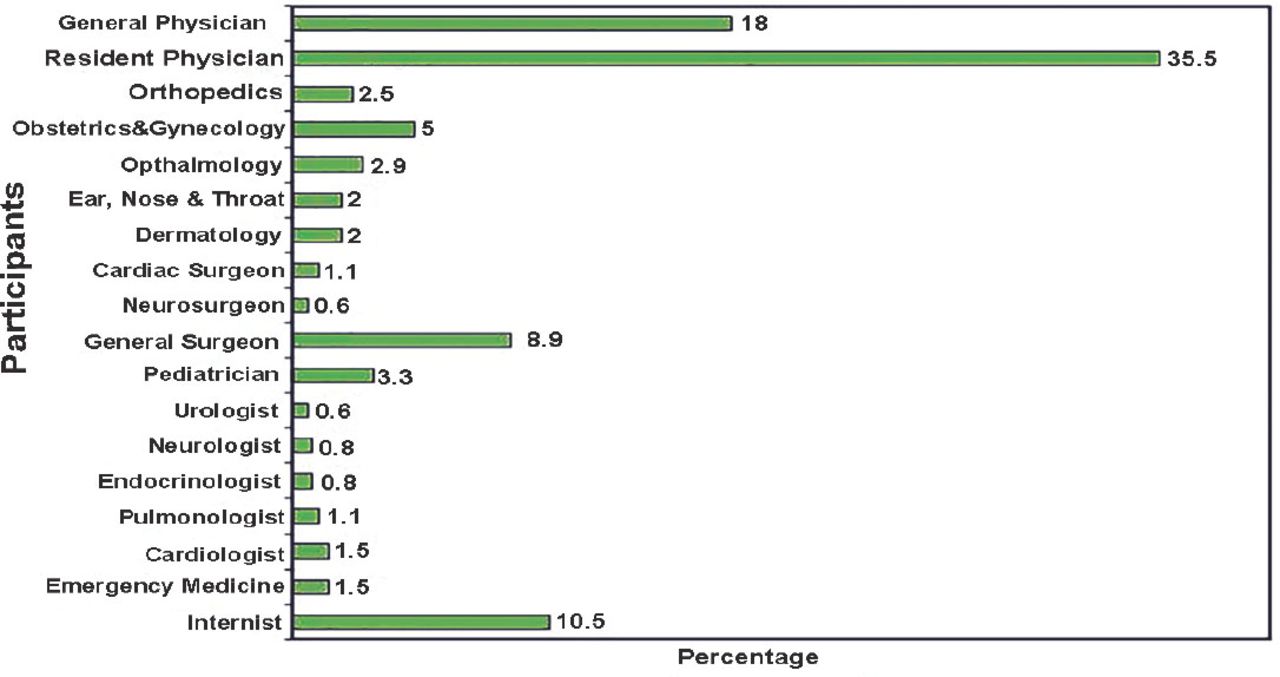
We performed a multidisciplinary, cross-sectional survey of clinicians from university, public, and private hospitals in Jeddah, Saudi Arabia, from August to October 2014. By taking into consideration the population size of the clinicians of 3 hospitals and application of 95% confidence level, the sample size was calculated as 565, out of which 447 respondents completed the questionnaire. The participants comprised 55% male, and 45% females. There were 252 participants <30 years old, 150 were between 30-50 years old, and 45 were >50 years old. The medical staff was categorized as 81 general physicians, 159 resident physicians, and 207 specialists. Among specialists, 37.8% were from different surgical specialties, and 62.2% were from internal medicine, pediatrics, emergency medicine, dermatology, obstetric and gynecology, ophthalmology, and orthopedics (Figure 1). Participants from university hospitals comprised 231, with 114 from private hospitals, 102 from public hospitals. The respondents were divided inot general physicians, resident physicians, and specialists to assess the resemblance and the divergence of their comprehension, outlook, and prescribing practices of AM. To prepare an appropriate questionnaire for the study a systematic search was carried out to identify suitable articles/studies using PubMed, Medline, Scopus, and Google scholar search engines. The following keywords and MeSH terms were utilized, “antibiotics”, “AMs” and clinicians, medical staff combined with any alternative like: “indication of AMs/antibiotics”, “types of antimicrobial prescribed”, “duration of AMs prescription”, “AM resistance”, “knowledge,” “attitude” and AM practices of clinician and/or medical staff. A multidisciplinary group of experts involving 3 experts of infectious disease, 3 clinical pharmacologists, and a psychological expert designed the questionnaire including demographic information, participant’s professional profile, their knowledge in relation to the current scope of antimicrobial use and resistance, and the main sources of information considered by themselves highly resourceful for continuing education of AMs. An appropriate questionnaire comprising 58 items was prepared following evaluation of literature and questionnaires pertaining to former similar studies.16-20 The validation of the questionnaire was subsequently carried out by executing a pilot study in 20 specialists, before commencing this study. After approval of the study protocol by the institutional ethical committee, a self-administered questionnaire was distributed randomly to the participants by the hospital directors during the working hours at their work place, and participants were requested to respond promptly. The response rate was 79.1%. No incentive was offered; information obtained from the respondents was secured during the study.
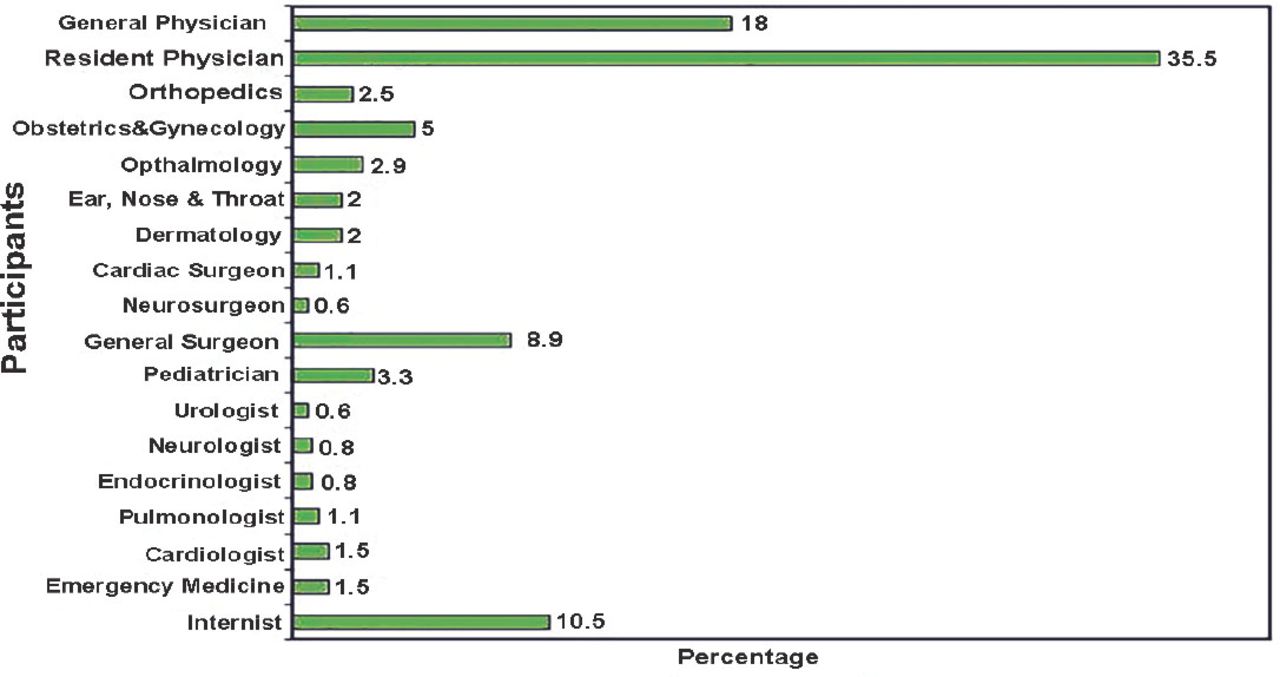
Categorization of the participants included in the study according to specialty.
Statistical analysis
Analysis of all the information obtained was carried out using the IBM SPSS Statistics for Windows, version 19.0 (IBM Corp, Armonk, NY, USA), and the expression of the results was carried out by absolute numbers and percentages. In case of normally distributed data, the differences between the groups of respondents were analyzed using Fischer’s exact test with the intention to test for significant association between the groups (p<0.05), while non- normally distributed data was evaluated by the 5-point scale of the Kruskal-Wallis test, this was consequently embraced by the response inclination of clinicians into agreeing, neutral, and disagree categories.
Results
Antimicrobial utilization by the participants
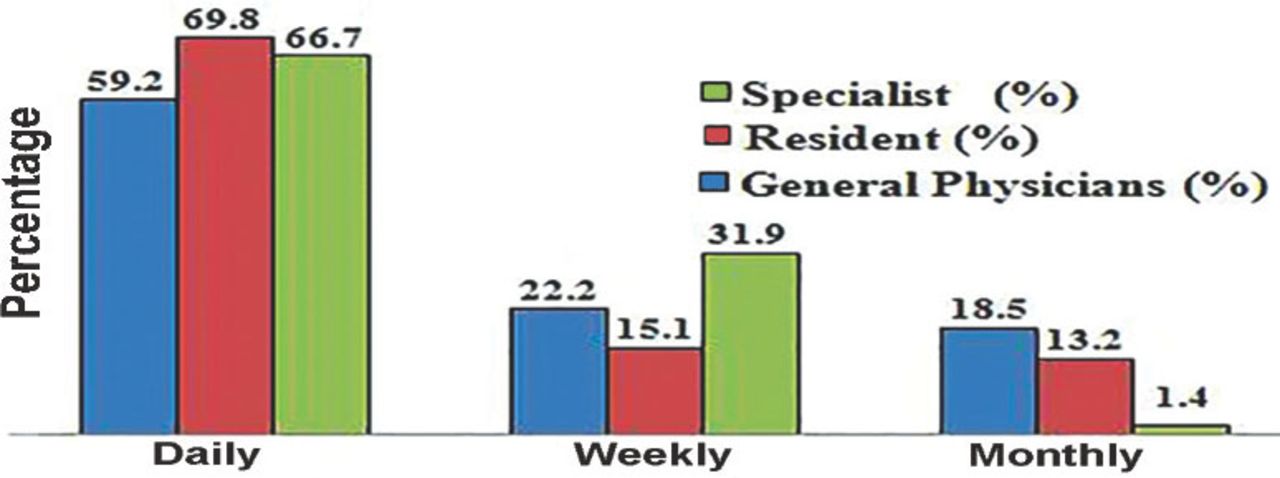
Antimicrobial prescriptions among the different groups for daily use was illustrated to be more or less same with no significant difference; it was 66.7% for residents, followed by 69.8% for specialists and 59.2% for general physicians (Figure 2).
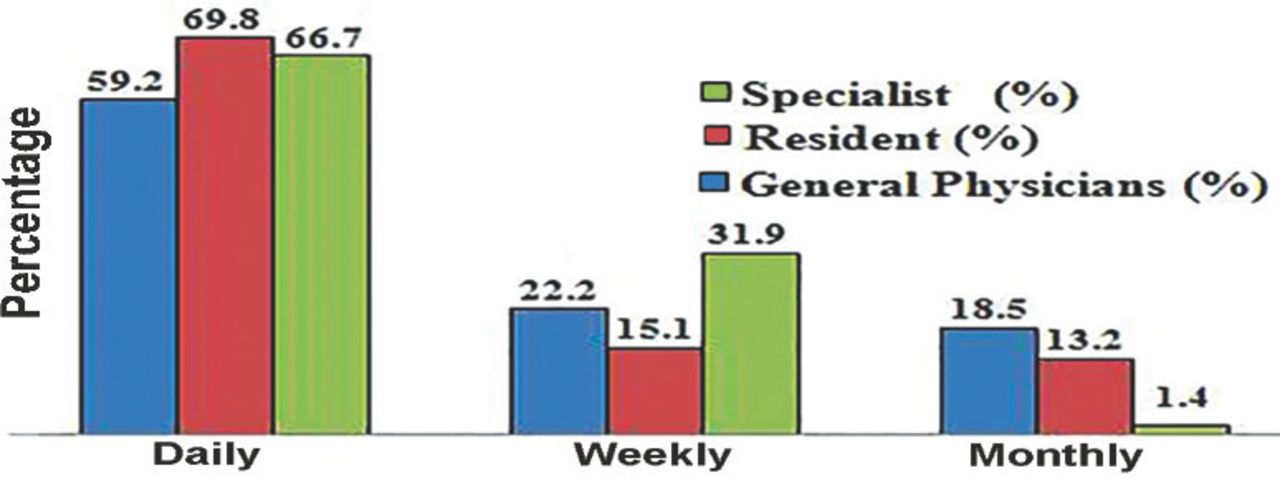
Utilization rate of antimicrobials by the participants included in this study.
Factors influencing the choice of AM by the respondents
Categorical similarities were observed in all groups pertaining to the comprehension of scientific materials, attending courses and lectures, effectiveness and past experience with the drugs, recommendations by other colleagues, and knowledge acquired during their medical education (Table 1). However, 3 important parameters of prescribing behavior; namely, prescription based on patient/parent’s demand, the cost of AM, and tranquility of mind portrayed a statistically significant difference in general physicians in contrast to resident physicians and specialists.
Factors influencing the choice of antimicrobials among the participants included in the study.
Knowledge and perception of the present scope of AM agents
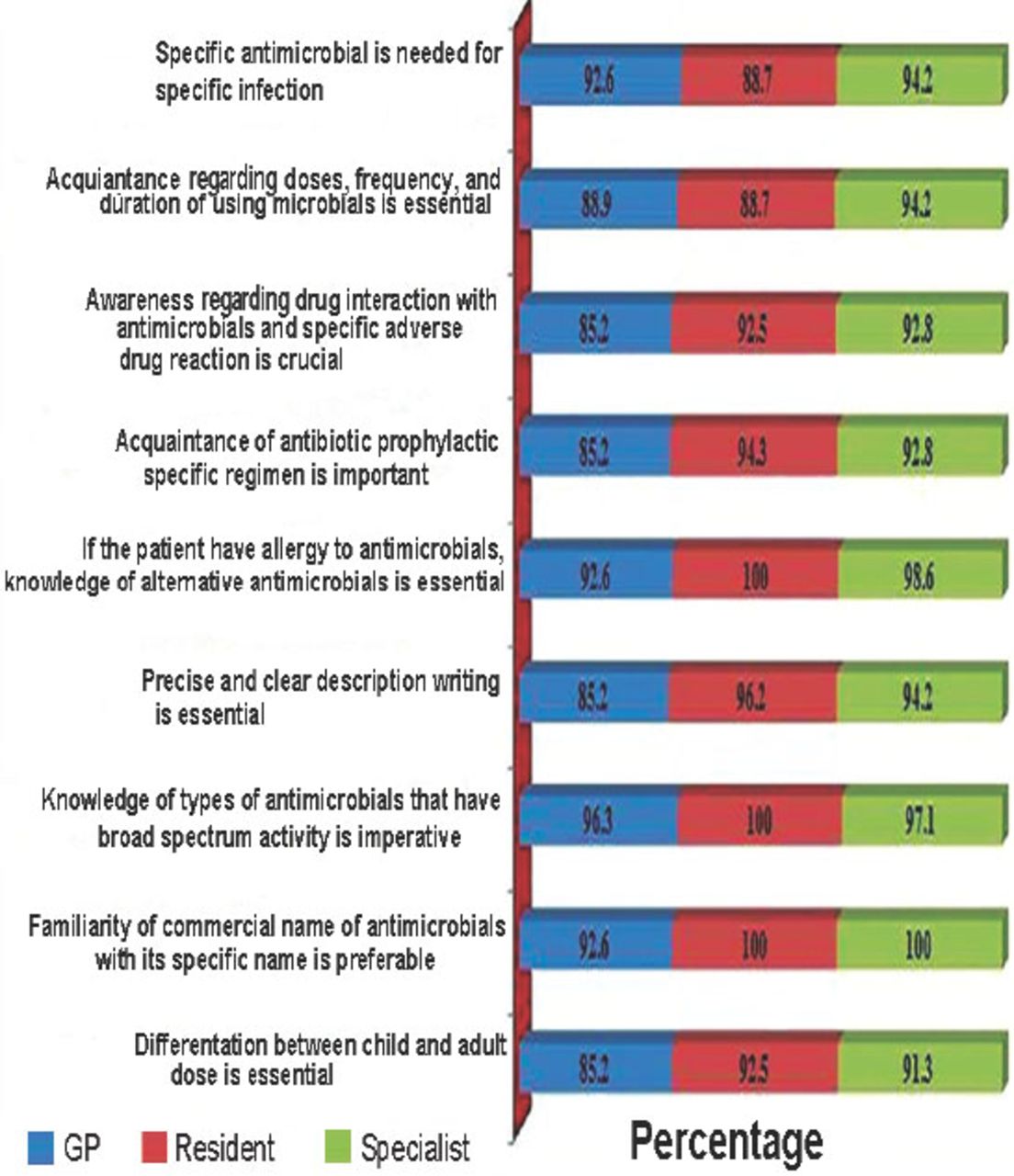
All the respondent groups had comparable perspectives, and no distinct differences were observed statistically in their knowledge of range of utility of AMs based on microorganism (Figure 3). The demarcation between child and adult dose is imperative, which in the results, bears similar likeness in all the respondents, general physicians (92.6%), resident physicians (88.7%), and specialists (94.2%).
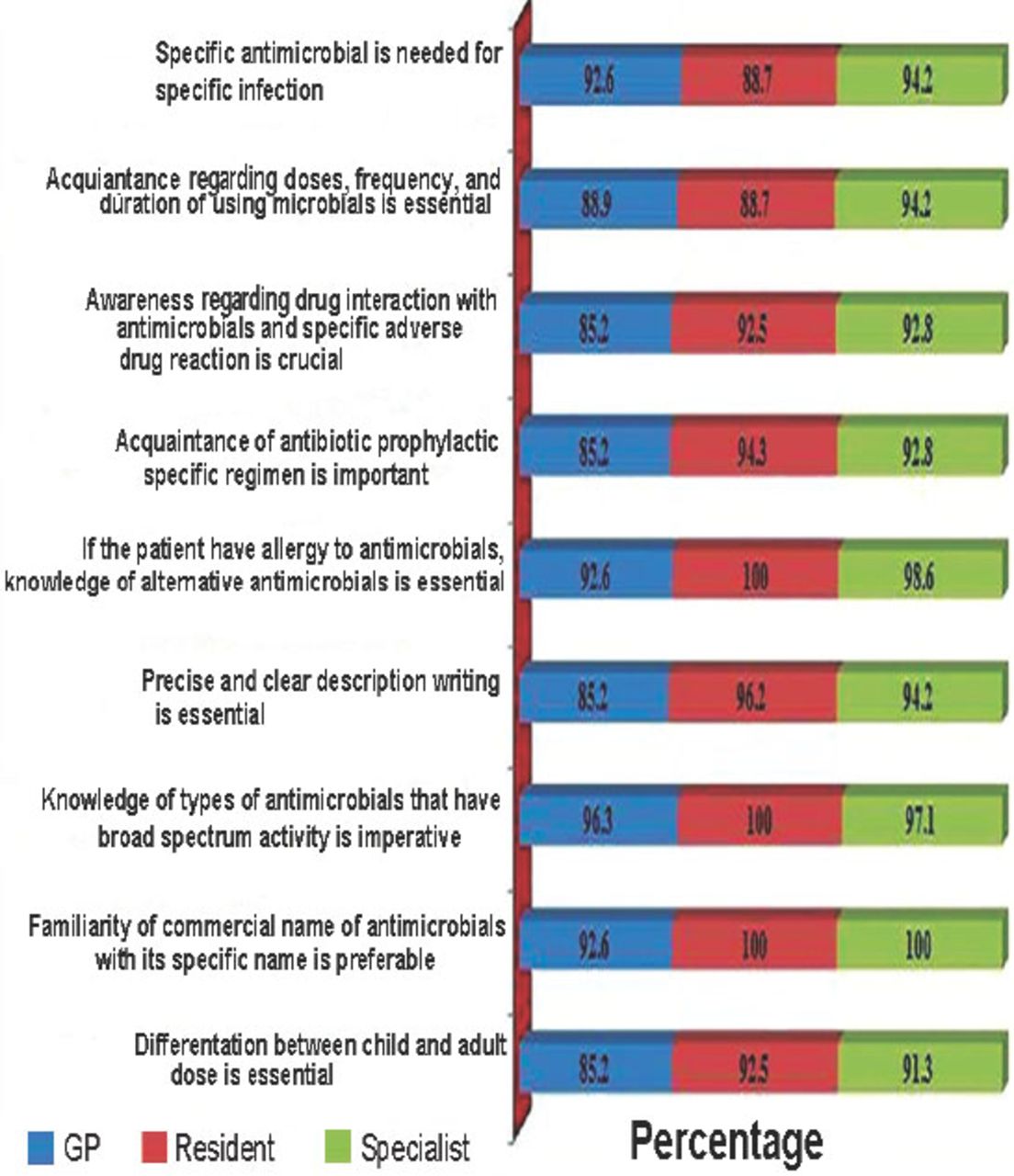
Knowledge and awareness regarding the current scope of antimicrobial agents used by the participants.
Knowledge concerning AM use
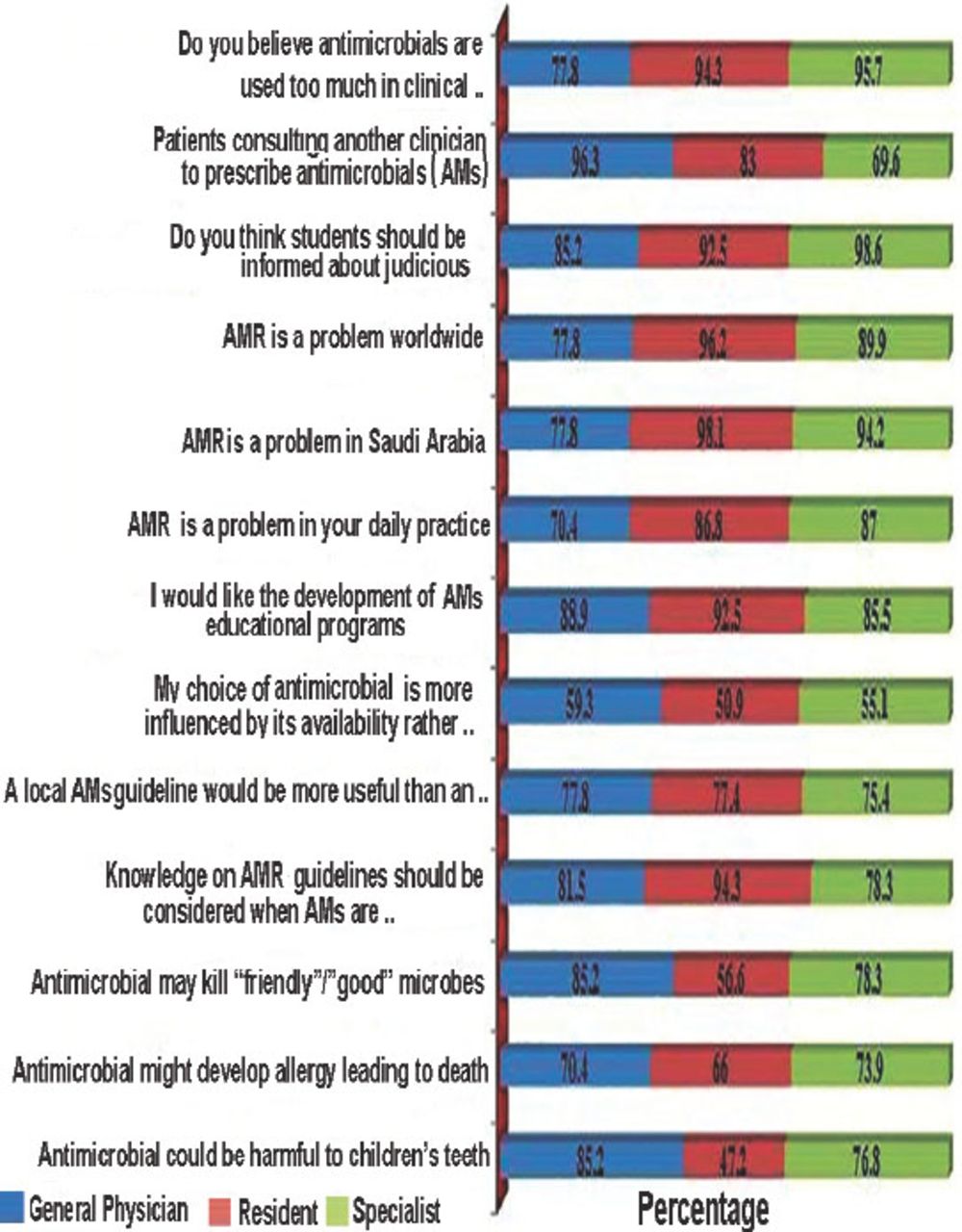
Disparity was observed between general physicians and 2 other groups of respondents in the disproportionate use of AM in their routine practice, only 40.7% of the general physicians agreed, while the acceptance rate of the resident physicians was 94.3%, and in specialists was 95.7% (Figure 4). All the 3 groups of respondents revealed similar responses regarding AMR as not only a worldwide and countrywide dilemma, but also a setback in their daily practice as well. Enthusiasm to have antimicrobial educational courses was similar between general physicians - 88.9%, resident physicians - 92.5%, and specialists - 85.5%. They all agreed with the concept that knowledge of AM should be considered when AMs are prescribed to a patient, general physicians - 81.5%, resident physicians - 94.3%, and specialists - 78.3% (Figure 4). In addition, a coherent analogous agreement was observed in all 3 groups of respondents regarding the ability of microbes to disrupt the commensal microorganisms, their ability to produce allergic response, and harmful effect on the teeth of children.
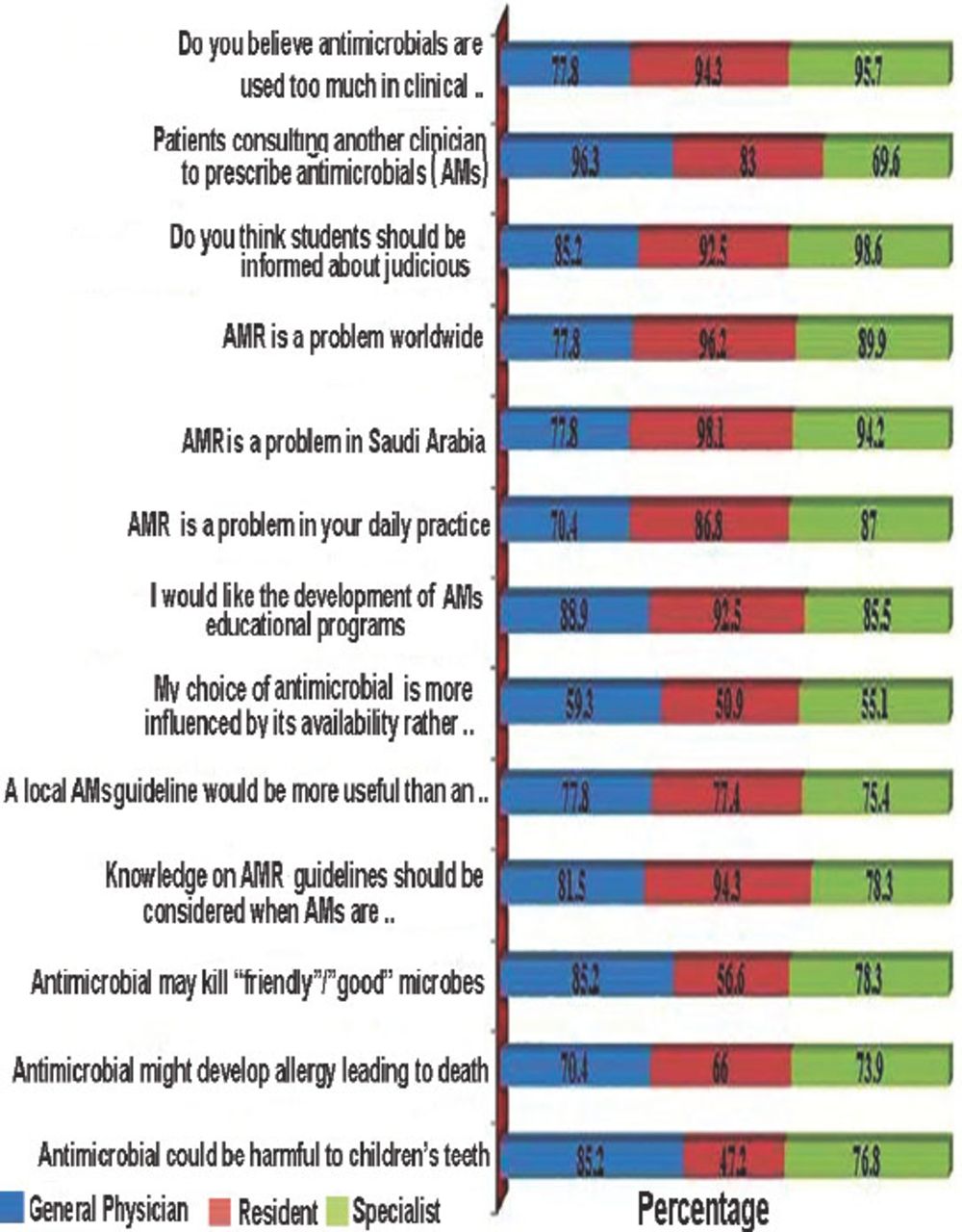
Knowledge of antimicrobial use according to participants in this study. AMR - antimicrobial resistance
Knowledge of the participants regarding the cause of AMR
Uniformity was displayed in all 3 categories of the participants, in view of inappropriate use, noncompliance, self-medication, and utilization of different trademarks of the same AMs as a core reason for the development of AMR (Table 2).
Knowledge of the respondents regarding the causes of antimicrobial (AM) resistance.
Knowledge of the effectiveness of AM continuing education sources on AM prescriptions
Various antimicrobial continuing education sources play an important role in influencing antimicrobial prescription; however, this study revealed that 92.6% of general physicians, 86.8% of resident physicians, and 30.4% of specialists opted for expert opinion. Conversely, 91.3% of the specialists, and 92.5% of the resident physician heavily rely on the pocketbook of infectious disease therapy in comparison with only 40.7% of the general physicians. Similar statistically significant findings were also observed with iPhone or Smartphone applications (Table 3).
Knowledge regarding the effectiveness of antimicrobial (AM) continuing education sources on AM prescription among respondents in this study.
Practice of using AMs
The practical knowledge of the 3 groups of participants for lack of need for AMs in the treatment of the most common infective conditions in the outpatient setting, such as acute diarrhea and acute pharyngitis were excellent and encouraging (Table 4). In contrast, when asked about the necessity of dose adjustments for Clindamycin and Gentamicin in patients with impaired kidney function, 98% specialists, 91% of residents agreed, while only 33% of general physicians agreed. Similarly, for recognition of AMs as a causative agent for Clostridium difficile infection, 97% of specialists and 76% of residents revealed the correct choice, whereas only 29.6% of the general physicians chose the accurate option. In the selection of a suitable antimicrobial for β-lactamase positive E. coli bacteremia, the proficiency of specialists was 94%, in resident physicians was 74%, and only 29.6% of the general physicians were able to provide a proper selection. Correspondingly, to recognize the conditions with possibility for the needless use of AMs and the drug of choice of AMs for a complicated case of urinary tract infection, most specialists and residents had a correct choice, whereas the scoring of general physicians were observed to be quite disappointing in this regard.
Review of comprehension of antimicrobials with the resulting division of correct reply of medical staff.
Discussion
Reduction of disproportionate antimicrobial utilization is the major key factor in the repression of AMR,1-5 and this could be accomplished to a great extent by modification of prescribing manners of the clinicians.1,8,9,16 Hence, this study was carried out to scrutinize and seek out the potential educational intervention relating to antimicrobial prescribing practices.
This study revealed that all the respondents acknowledged the magnitude of knowledge gained during their education, reading scientific materials, attending courses and lectures as well as knowledge gained during undergraduate or postgraduate training. However, a statistically significant disparity was observed between general practitioners and resident physician with specialists on parent / patient’s demand, the cost of the AMs, and peace of mind (Table 1). These 3 parameters are obviously influenced by an inability to diagnose and attending a huge number of patients in quick succession.1 This inconsistency necessitates a forceful educational move to overcome this significant inclination of prescribing behavior for AMs.16-20 Comprehension regarding effectiveness of antimicrobial continuing education sources on antimicrobial prescription (Table 3) showed a statistically striking dissimilarity between general practitioners and resident physician on seeking expert opinion and following the pocket book of infectious disease therapy. However, concerning iPhone or smartphone application, Saudi drug formulary, and institutional antimicrobial guidelines all the participants revealed passive responses. These perceptions, poor appreciation, and unfamiliarity with national guidelines are noticeably unusual from other recent studies,16,21,22 seemingly this requires persuasive educational interventions. It is imperative to have a clear concept of theoretical knowledge for clinical practice with the aim of reducing AMR.1,16-20 Unequivocally, this study has revealed all the participants have the excellent awareness of indication, contraindication, drug interaction, and unwanted effects of AMs (Tables 2 and Figure 3).
In addition, all the respondents, quite reasonably identified AMR as a national and global setback and concern. The prospect of alteration of commensal intestinal flora by the AMs (Figure 3), potential harmful effect on a child’s tooth, and severe allergic drug reaction also received explicit affirmative responses from all the groups of participants. The perception and outlook pertaining to AM utilization and AMR of all the groups of participants are summarized in Table 2, Figures 3 & 4. Enhanced perception of the fundamental reasons for AMR and rational use of AMs is the basic essence to overcome AMR;1,7,16,17,20,23 interestingly, in our survey, these parameters were evidently illustrated and accepted by all the groups.
Reviews of comprehension of AMs with the resulting division of correct response of participants were observed in Table 4. Although, taken as a whole acquaintance with indication, contraindication, drug interaction, and unwanted effects of AMs of all the participants varied from very good to excellent, in addition they all agree on the lack of need for prescribing AMs for acute diarrhea an acute pharyngitis. However, the group of respondents comprising of general practitioners in comparison to resident physicians and specialists substantially proved to be lacking in their knowledge regarding requirement of dose adjustment of Clindamycin and Gentamicin in renal impairment, as well as recognition of appropriate microorganism responsible for producing Clostridium difficile infection. This lack of knowledge was further exposed by the lack of suitable selection of AM for β-lactamase positive E. coli bacteremia, and identifying the settings for needless use of AMs and selection of the optimal regimen of AMs for a complicated case of urinary tract infection. This disparity was statistically significant, and warrants suitable targeted educational interventions; however, similar gaps in knowledge were also reported in few recent studies.16-20,24-26 Although this appraisal illustrates good knowledge and outlook of most of the respondents, general practitioners seem to have an unclear perception on issues regarding choice of AMs. The enormous values of antimicrobial continuing education sources on antimicrobial prescription were not adequately appreciated by all groups of the respondents. In addition, a gap of proficiency evaluation and incongruity was observed in general practitioners in contrast to resident physicians and specialists. This indicates the need for appropriate targeted educational interventions.
Study limitations
The inherent limitation of such evaluation is that the respondents tend to generally provide answers sought after, as an alternative to the realistic viewpoint. However, to defeat this pragmatic situation, we incorporated 2 validity, and reliability questions in the questionnaire, these questions bear both affirmative and negative aspects that guide to identify the legitimate responders.
Recommendations
Excellent educational interventions to incorporate the necessity of rational and standardized antimicrobial use, especially among the general practitioners seems to be vital, although all respondents should be capable of rigorously following the local and national guidelines to avert the excessive use of AMs and consequently repress the AMR.
In conclusion, this study revealed that the respondents have a clear concept of theoretical knowledge of AMR and cautious use of AMs. However, discrepancies were recognized in general practitioners regarding the seeking of effective educational resources, proficiency, and factors influencing antimicrobial use. All respondents were not strictly following the national and local guidelines of AM use. This highlights the requirement for AM stewardship with precise information and decisive ambition of reduction in AMR.
Related Articles
Baadani AM, Baig K, Alfahad WA, Aldalbahi S, Omrani AS. Physicians’ knowledge, perceptions, and attitudes toward antimicrobial prescribing in Riyadh, Saudi Arabia. Saudi Med J 2015; 36: 613-619.
Al-Harthi SE, Khan LM, Abed HH, Alkreathy HM, Ali AS. Appraisal of antimicrobial prescribing practices of governmental and non-governmental dentists for hospitals in the western region of Saudi Arabia. Saudi Med J 2013; 34: 1262-1269.
Khan LM, Al-Harthi SE, Saadah OI, Al-Amoudi AB, Sulaiman MI, Ibrahim IM. Impact of pharmacovigilance on adverse drug reactions reporting in hospitalized internal medicine patients at Saudi Arabian teaching hospital. Saudi Med J 2012; 33: 863-868.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 24, 2015.
- Accepted May 18, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}