


Abstract
Objectives: To measure the efficacy of new insulin analogues compared with the conventional types of insulin, and to compare their effects on patient satisfaction regarding their weight changes and the frequency of hypoglycemic episodes.
Methods: In this retrospective cohort observational study, data was collected from the medical records of 122 eligible diabetics on insulin therapy attending government primary care centers in Jeddah, Kingdom of Saudi Arabia from June 2013 to July 2014. The data collected considered the efficacy, safety, and patient satisfaction of the types of insulin therapy used for their treatment.
Results: After 12 weeks, there was a reduction in mean glycosylated hemoglobin (HbA1c) of -0.88% for the analogue type versus -0.19% for the conventional type, and at 24 weeks, the mean drop in HbA1c was -2.02% for the analogue type versus -1.12% for the conventional type, but the differences were not statistically significant. More patients (87% versus 38%) on analogue compared with conventional insulin treatment were satisfied with therapy.
Conclusion: In the primary health care setting, insulin analogues showed greater efficacy improvements than conventional insulin therapy within 6 months. However, conventional insulin therapy can still be used at primary care centers with limited resources, and when patients refuse to be converted.
Diabetes mellitus is a major cause of morbidity and mortality, and its global prevalence is rising rapidly.1 The estimated direct annual medical cost of diabetes care in Saudi Arabia is enormous; it constitutes an economic burden on the country.2 Since diabetes mellitus is a chronic illness that requires continuing medical care to reduce the risk of long-term complications,3 currently many diabetic patients attend the governmental primary care centers to receive this care. Studies from the United Kingdom confirmed the benefits of improved glycemic control in patients with types 1 and 2 diabetes mellitus,4,5 and they recommended tight glycemic control to maintain the glycosylated hemoglobin (HBA1c) concentrations of 7% or less. Insulin therapy is indicated to control all patients with type 1 diabetes, uncontrolled type 2 diabetics, and gestational diabetes to achieve the recommended target. There are 2 main types of insulin, the old conventional insulin that include the regular human insulin, and intermediate-acting neutral protamine Hagedorn insulin (NPH); however, these agents could not mimic the physiological pattern of endogenous insulin secretion, so insulin analogues were developed to overcome this limitation.6 Despite this theoretical superiority, the short acting insulin analogues were found to have a minor benefit to HBA1c values compared with the regular insulin in adult patients with type 1 diabetes mellitus, and no benefit in the population with type 2 or gestational diabetes.7 The 2 basal insulin analogues, insulin Glargine and Detemir, which have different chemical structures and modes of actions, were also developed to overcome the limitations of NPH insulin. Hypoglycemia and weight gain were always the main fear for patients on insulin, but studies on the analogues were conflicting, some did not observe a major clinical advantage in terms of hypoglycemia for either the rapid-acting or the long-acting insulin analogues over conventional insulins, others found that both rapid and long-acting analogues had little benefit in terms of glycemic control or reduced hypoglycemia. But insulin analogues were superior over the conventional insulins in terms of quality of life.8,9 The insulin analogues although expensive, adding to the enormous budget of the Ministry of Health in the treatment of diabetes mellitus, were introduced for free dispensing in some governmental primary health care centers in January 2014. The available analogues are the long-acting, Glargine (Sanofi, Bridgewater, NJ, USA), and the short acting Lispro (Eli Lilly & Co, Indianapolis, IN, USA) and Aspart (Novo Nordisk Inc., Plainsboro, NJ, USA), and their biphasic analogues, namely, Humalog in both concentrations 25/75 and 50/50 (Eli Lilly & Co, Indianapolis, IN, USA), and also NovoMix 30/70 (Novo Nordisk Inc., Plainsboro, NJ, USA). Though some patients are satisfied and refused to convert, efforts are in place to replace the current conventional insulin with the new insulin analogues for their proposed superiority of efficacy, safety, and quality of life. This study was carried out to help the general practitioners in choosing among the different insulin types, and in counseling their diabetic patients attending the government primary care health centers regarding their choice of insulin therapy.
Methods
Study design and setting
This retrospective cohort study was conducted at 2 government-funded primary care centers, in Jeddah, Kingdom of Saudi Arabia. They have approximately 1500 registered diabetics who receive regular follow-up and treatment. This medical record based study was approved by the Health Directorate, Research center, Jeddah, and conducted from June 2013 to June 2014. The American Diabetic Association Guidelines recommendations3 were followed for insulin initiation, titration, and monitoring. The regimens were individualized according to the patient centered approach. We included all diabetic patients on insulin therapy; they were divided into 2 groups. The first group was for those who were started on conventional insulin either alone or combined with oral hypoglycemics and had regular monthly follow-up visits for 6 months. The second group was for those who were started on the insulin analogues from the start and those who were converted from the conventional to the analogues type, either alone or combined with oral hypoglycemics and had a regular monthly follow-up visits for 6 months. Gestational diabetics were excluded as they require a special treatment protocol. For eligible diabetics, the baseline HBA1c, weight in kilograms and duration of diabetes were recorded prior to the introduction of the insulin therapy for each group, the insulin types and regimens were also defined. The HBA1c and weight were again recorded from the medical records after 12 and 24 weeks. The number of reported hypoglycemic episodes (which were defined as any reported hypoglycemic symptoms such as tremors, dizziness, headache, fainting, and documented low blood sugar by glucose home monitoring of being less than 70 mg/dl) was counted. Patient satisfaction with the therapy (less than 2 episodes per month and no weight gain) was recorded.
Statistical analyses
Descriptive analyses of the qualitative variables were displayed as proportions and percentages. Continuous variables were described as mean and SD values. The change from baseline in HbA1c, and body weight was analyzed using a paired t-test. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY, USA). Significance was set as a p-value <0.05.
Results
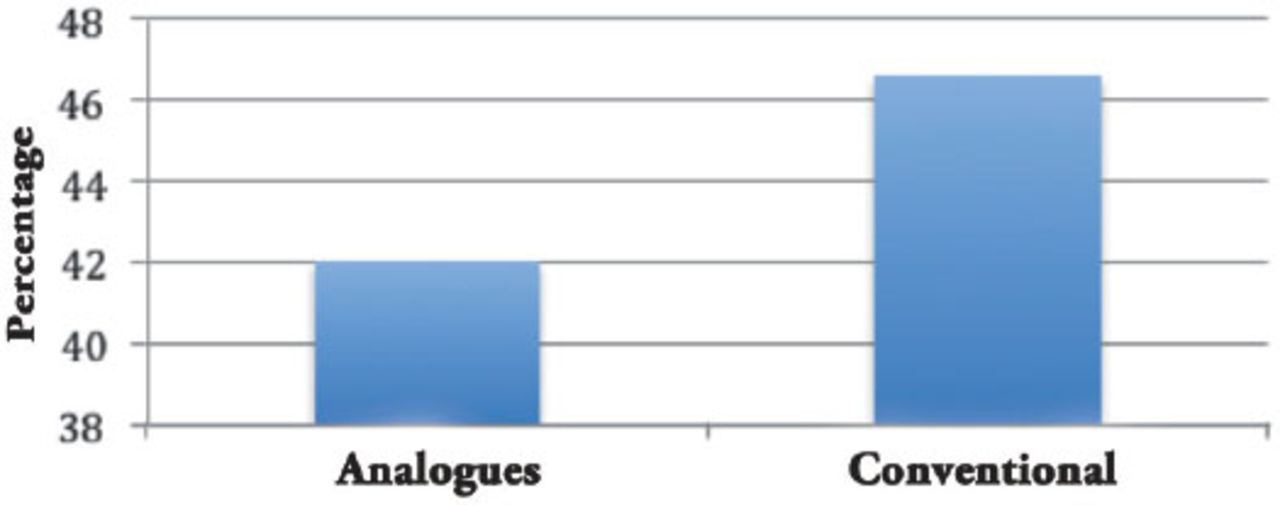
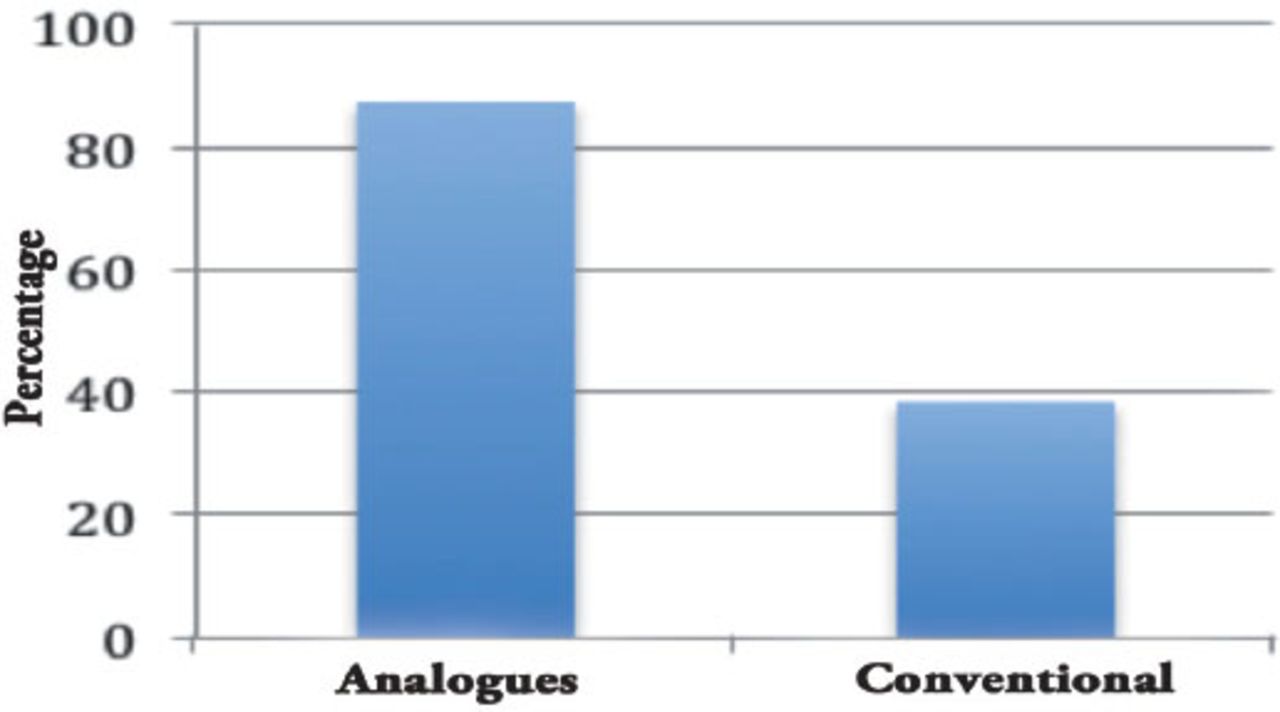
A total of 122 diabetic patients were enrolled in this study, 60 (49.2%) were on conventional insulin therapy, 62 (50.8%) were on insulin analogues, 20 of them (32.3%) were started on it for the first time, and 42 (67.7%) were converted from the conventional to the analogues types. The mean age of the insulin analogues group (54.4 years) was slightly lower compared with the conventional insulin group (57.1 years) (p=0.026). There was a significant difference in gender regarding the use of insulin types, 38 (61.3%) males used the insulin analogues, 20 males (33.3%) used the conventional, while 24 female (38.7%) used the analogues, and 40 females (64.5%) used the conventional insulin (p=0.001). Table 1 shows that there was no significant difference between the groups, in the baseline weight, HBA1c, and the duration of diabetes mellitus. Table 2 summarizes the levels of HBA1c and weight after 12 weeks, the mean HBA1c for analogues dropped by -0.88 (p=0.173), while it dropped by -0.19 for the conventional insulin group (p=0.166). Table 3 summarizes the levels of HBA1c and weight after 24 weeks, the mean HBA1c dropped by -2.02 for the analogues group (p=0.122) while it dropped by -1.12 for the conventional group (p=0.652). There was weight gain in both groups after 12 and 24 weeks, but the differences were not statistically significant. More than 2 hypoglycemic episodes occurred in only 26 patients (41.9%) on the insulin analogues, while it occurred in 28 patients (46.6%) on conventional insulin (Figure 1). There was a significant difference in patient satisfaction, out of the 62 diabetics who were on insulin analogues, 54 (87.1%) were satisfied, but only 23 (37.1%) were satisfied in the conventional insulin group (p=0.0005) relative risk 2.724, 95% confidence interval: 1.727-4.296 (Figure 2).
Baseline comparison between the insulin analogues group and the conventional insulin group in diabetic patients attending primary care centers.
The glycosylated hemoglobin (HBA1c) and weight after 12 weeks in diabetic patients attending primary care centers.
Glycosylated hemoglobin (HBA1c) and weight after 24 weeks among diabetic patients attending primary care centers.
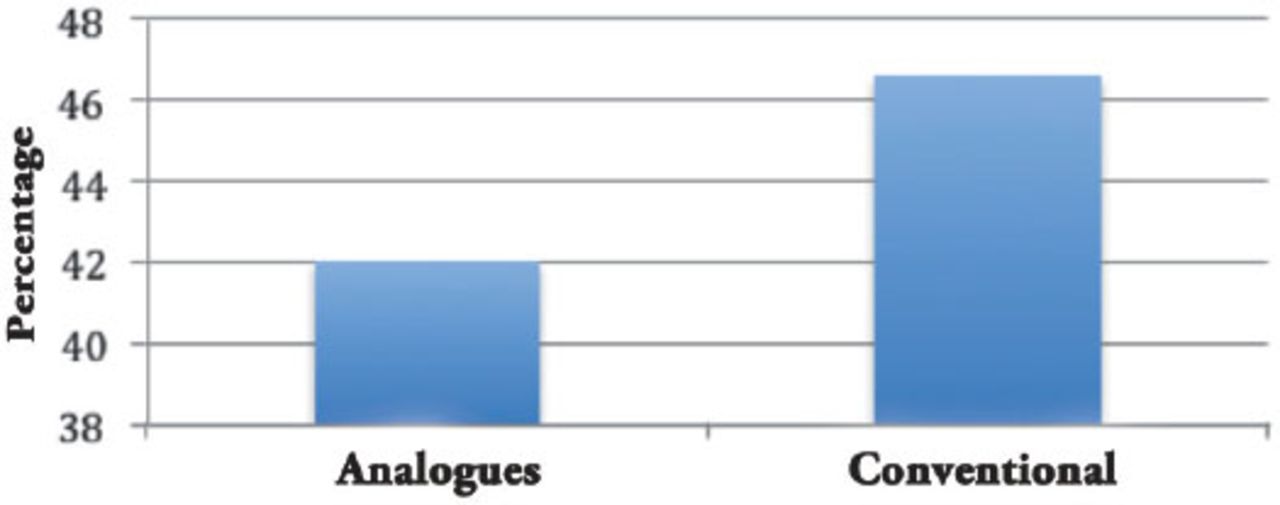
Percentage of diabetic patients who had more than 2 hypoglycemic episodes per month.

Percentage of diabetic patients who were satisfied with their insulin therapy.
Discussion
For most diabetic patients, the ideal target for HbA1c should be below 7% since achieving this level of control reduces the risk of end-organ damage. Every 1% drop in HbA1c reduces the risk of microvascular complications by 40%, and death by 21%.1,9 Conventional insulin therapy is effective in reducing the HBA1C for up to 1.5%. The insulin analogues were developed to mimic the physiological endogenous secretion and cause less hypoglycemia and weight gain. Although some studies failed to prove this theoretical difference, a meta-analysis carried out to compare the outcomes of both insulin analogues with the conventional insulins found little benefit regarding their glycemic control and hypoglycemic episodes.6 But the A1Chieve,9 a metacentric non-interventional study on 60000 diabetics in 28 countries, across 4 continents, over 24-weeks, evaluated the safety and effectiveness of insulin Detemir, biphasic insulin Aspart, and insulin Aspart (Novo Nordisk Inc., Plainsboro, NJ, USA), in people with type 2 diabetes mellitus, concluded that starting or switching to insulin analogues was associated with improvement in glycemic control with low frequency of hypoglycemia.9,10 While an Italian study10 carried out to compare basal NPH with Detemir and Glargine found that the long-acting analogues provided superior glucose control for up to 32 hours in type 1 diabetics. Regarding weight gain, which was one of the most important fears of diabetics on insulin therapy, a study found that the factors that predict weight gain over 12 months were diabetes related distress, insulin initiation and titration dosages, and age.11 In our study of a total of 122 diabetic patients, 60 were receiving conventional insulin, 62 were on insulin analogues, 20 were newly started, and 42 were converted from the conventional to the analogues. The slight difference in the mean age between the 2 groups was because we had included some younger individuals of diabetes type 1 in the analogue group and most of them were on the analogue basal-bolus regimen. The 2 groups were similar for other variables like mean basal weight, duration of diabetes, and HBA1c before the start. Although there was a significant difference in gender regarding the uses of insulin, mostly because males tended to use more analogues than females, which may be because females were more fearful and reluctant to convert.
We found a minor difference although not statistically significant in favor of the analogues in their ability to reduce HBA1c over 24 weeks (2.02 versus 1.12), which was almost similar to the results in the A1Chieve study,9 which showed an improvement of in HBA1c (insulin naïve: -2.5%, insulin users: -2.2%). Although hypoglycemic attacks were the main draw backs of insulin therapy according to many studies,12 we reported the occurrence of hypoglycemic episodes more than twice a month in 42% of diabetics on the insulin analogues compared with 48% in those who were on the conventional group, the difference was not statistically significant. Regarding weight gain during insulin therapy, consistent with different studies on insulin that showed a strong association with weight gain, either due to hypoglycemia, psychological distress, aging, and water retention,11 in our study the weight gain before and after treatment was highly significant and similar in magnitude for both groups. The significant differences observed in patient satisfaction in this study, in terms of the frequency of hypoglycemic attacks, and weight gain (87% of those on the insulin analogues, were satisfied compared with only 38% of those on conventional insulin) were consistent with different studies on satisfaction and quality of life.13,14
The main study limitations are that this study was a retrospective observational study, and the sample was small and only from 2 centers. The statistical analysis would have been more accurate if the study design was of a prospective cohort, and the sample was large enough, and there was an adjustment for age and gender.
In conclusion, the introduction of new insulin analogues in the primary care setting to be used by the general practitioner was a good addition for managing diabetics. However, there is a need for further efforts from the physician to master the new guidelines of insulin analogue therapy, initiation, conversion, titration, patient education, home glucose monitoring, and follow-up to get the maximum benefits and avoid complications like frequent hypoglycemia and weight gain. For all those who will be started on insulin therapy, insulin analogues are the preferred choice, and those on conventional insulin should be counseled for conversion, but their preference should be respected.
Related Articles
Al-Hayek AA, Robert AA, Braham RB, Turki AS, Al-Sabaan FS. Frequency and associated risk factors of recurrent diabetic ketoacidosis among Saudi adolescents with type 1 diabetes mellitus. Saudi Med J 2015; 36: 216-220.
Habib SS. Serum resistin levels in patients with type 2 diabetes mellitus and its relationship with body composition. Saudi Med J 2012; 33: 495-499.
Ansar H, Mazloom Z, Kazemi F, Hejazi N. Effect of alpha-lipoic acid on blood glucose, insulin resistance and glutathione peroxidase of type 2 diabetic patients. Saudi Med J 2011; 32: 584-588.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 29, 2015.
- Accepted April 27, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.