


Abstract
Objectives: To screen for low bone mineral density among young adult Saudi women using quantitative ultrasound (QUS) and exploring the high risk groups.
Methods: A cross-sectional study was performed on 279, 20-36 years old female students and employees of Taibah University, Al Madinah Al Munawwarah, Kingdom of Saudi Arabia between January and May 2014. The study included bone status assessed using QUS, a structured self-reported questionnaire, anthropometric measurements, and evaluation of bone markers of bone metabolism.
Results: The prevalence of low bone mineral density was 9%. Serum osteocalcin was found significantly higher in candidates with low bone mineral density, 20.67 ng/ml versus 10.7 ng/ml, and it was negatively correlated with T-scores. At any given point in time the exposed subjects to low calcium intake and inadequate sun exposure in the population were 11 times and 3 times more likely to have low bone mineral density, (adjusted odds ratio [OR], 11.0; 95%confidence interval [CI]=3.16, 38.34; p=0.001) and (adjusted OR, 3.32, 95%CI=1.27, 8.66, p<0.01).
Conclusion: Early detection screening programs for low bone mineral density are needed in Saudi Arabia as it affects young Saudi women specially the high-risk group that includes young women with insufficient calcium intake and insufficient sun exposure. Serum osteocalcin as a biomarker for screening for low bone mineral density could be introduced.
Osteoporosis is a major public health problem, characterized by a diminution in bone mass and a destruction of bone architecture. Osteoporosis affects approximately 200 million people worldwide, and is the primary cause of 1.5 million fractures per year in the United States.1 The prevalence of osteopenia and osteoporosis of either the spine or the femur in Saudi women ≥50 years old is estimated to be as high as 43.4% for osteopenia and 41.4% for osteoporosis.2,3 According to the Saudi Osteoporosis Society, the annual cost of osteoporosis-related femoral fractures in Saudi Arabia was approximately 1.14 billion USD in 2007.4 Therefore, screening for bone mass quality among young women at the peak of their bone mass, between the ages of 20 and 36 years, is considered as a prophylactic process for early identification and prevention of osteoporosis to lower the risk for fracture-related morbidity and mortality.5 Although, the gold standard test for bone mineral density (BMD) is dual-energy x-ray absorptiometry (DEXA), quantitative ultrasound (QUS) technology has emerged as a convenient and portable tool for screening of BMD. In addition to measuring BMD, QUS also provides information on the micro-architecture of the bone.6 To improve the predictive value of QUS screening for BMD-related fracture risk, results should be interpreted within the context of other risk factors, which have independently been associated with BMD.7 Although many studies have evaluated bone status in Saudi women, most of these studies used DEXA at tertiary care facilities and focused on bone status among post-menopausal women over the age of 50 years. There is a lack of information on the bone status of women under the age of 50 years. Therefore, the aim of our study was to screen for BMD, at a university level (as a community institution that included the range of our target age group), using QUS to determine the prevalence of low BMD (osteopenia and osteoporosis) among young adult Saudi women, and to evaluate risk factors associated with low BMD.
Methods
This cross-sectional study included 304 healthy young Saudi women within the peak bone mass period between 20 to 36 years of age,7 and it was completed between January and May 2014. The study was conducted at Taibah University in the Al Madinah Al Munawwarah region. The University includes a diverse group of members of the community and from a large age range.8 Al Madinah Al Munawwarah is located in the NorthWestern part of Saudi Arabia, with a population of 1,100,093, according to the 2010 census.9 Our study focused on the female section of the University, which includes 15 colleges in 3 clusters, main campus, medical campus, and Alssalam campus. Eligible participants were healthy Saudi women, at a peak bone mass (PBM) ages of 20 to 36 years. Prospective participants were screened to exclude those with a diagnosis of osteoporosis or osteopenia, and those receiving treatment for these conditions.
Sampling procedure
A stratified cluster sampling procedure was used. Five colleges were selected from the 3 university clusters. Within each college, the primary sampling unit was the stratum of occupation (students, teaching staff, clerks, and workers). Then the samples of the target population were randomly selected (using random number tables) from the list of the selected college based on probability proportional to size of population. All visitors to the medical clinics during the study periods were included in the study. The selected participants were asked to come to the medical clinic of the University for medical examination and interview. Informed written consent was provided by all participants and the study received ethical approval from the University’s ethical committee
Data collection
A self-report questionnaire was used to collect data on socioeconomic, lifestyle, and clinical status. The following socioeconomic factors were recorded: age, area of residence, occupation, marital status, education, and household income. For analysis, the level of education was categorized as follows: higher level consisted of university education at the post-graduate, graduate, and bachelor levels; middle level consisted of secondary and intermediate school education; and low level consisted of education received at primary school, or no formal education. Monthly household income status was categorized as follows: low income level, <5000 Saudi Riyal (SRs); moderate income level, between 5000 and 10000 SRs; and higher level income >10000 SRs. Lifestyle habits included smoking, physical activity, sun exposure and type of clothing worn outdoors (namely, cover of face and/or whole body with clothes), and calcium intake. Calcium intake was evaluated based on the consumption of calcium-rich dairy products. Calcium intake (mg) was estimated from dairy products sources, as well as from non-dairy sources, as follow: milk (8 oz.), 300 mg; yogurt (6 oz.), 300 mg; cheese (1 oz.), 200 mg; and 250 mg were added for non-dairy sources. The total intake of calcium was estimated for each participant and copmared with the 2011 recommendations for dietary intake of vitamin D and calcium set out by the Institute of Medicine, which considers <1000 mg/day to be a low calcium intake for women <50 years.11 Based on this criterion, participants were classified into a normal or a low calcium intake group for analysis. The following clinical characteristics were evaluated: body mass index (BMI) <20 kg/m2; diabetes mellitus (DM); hypertension; previous history of a traumatic fracture; thyroid diseases, use of steroids; use of oral contraceptives; age at menarche; menstrual cycle; hysterectomy; removal of ovaries; and early menopause. Prior to the study, a pilot study was performed among 30 individuals to pre-test the questionnaire and the measurement methods to ensure reliability of the data. After analysis of the pilot study, a few questions of the questionnaire were modified.
Measurements
Bone mass quality was measured from the left calcaneus using the Lunar Achilles Ultrasonometer (In Sight, GE Healthcare, Chicago, USA), with a temperature-controlled water-based system used as a coupling medium for wave propagation. Ultrasound attenuation (dB/MHz) and speed of wave propagation (m/s) were measured and used to calculate the stiffness index. The measured stiffness was compared with normative reference values, and the T-score of BMD calculated. The reference criteria for diagnosis of low BMD established by the World Health Organization are based on DEXA values and, therefore; were not applicable to our study.12 Instead, we used the cutoff criteria provided in a previously published study,7 using QUS and conducted in Saudi Arabia. The following QUS T-score cutoff values were used: a score ≥1 is indicative of a normal BMD; a score between 1 and -1 is indicative of low BMD; a score between -1 and -1.8 is indicative of osteopenia; and a score ≤-1.8 is indicative of osteoporosis.
Anthropometric measures
Body weight was measured while wearing typical outdoor clothing, without shoes, using a standard weight scale, with weight reported to the nearest kg. Height was measured to the nearest cm using a stadiometer. All measurements were verified by 2 observers. The BMI was calculated from the recorded height and weight, and participants were categorized into 4 groups for BMI analysis: underweight (<18.5 kg/m2), lean (18.5-24.9 kg/m2), overweight (25-30kg/m2), and obese (>30 kg/m2).
Blood samples
Venous blood samples were obtained from 23 participants who provided consent for blood analysis. The following blood biochemical levels were evaluated: serum calcium, serum phosphorus, 25-hydroxy vitamin D (25-OHD), serum bone-specific alkaline phosphatase (B-ALP) isoenzyme, serum osteocalcin (OC) bone turnover marker, and bone anti-resorption marker osteoprotegerin (OPG).
Sample collection, storage, and assay test principals
Samples of 8 ml of venous blood were withdrawn and received in the laboratory in 2 test tubes. The first tube was left to rest for 10 minutes (min) to allow clot formation and then centrifuged at 3000 for 10 min. The serum was separated and stored at -80°C until biochemical analysis for calcium, phosphorus, and serum OC levels. The second tube was heparinized and the blood content centrifuged at 3000 g for 10 min. The plasma was separated and stored at -80°C until biochemical analysis for 25-OHD, human plasma OPG and B-ALP levels.
Levels of 25-OHD were analyzed using an enzyme-amplified sensitivity immunoassay (ELISA) Kit (Immunodiagnostic System Inc. IDS Inc., Woburn, USA), with the normal range defined as 9-37.6 ng/ml. Based on 25-OHD levels, participants were sub-classified as follows: vitamin D deficiency, 25-OHD concentrations <20 ng/ml; insufficient vitamin D, 25-OHD concentrations between 20-32 ng/ml; and sufficient vitamin D levels, 25-OHD concentrations >32 ng/ml.13
Assessment of bone marker levels
Levels of human OPG were evaluated using a standard sandwich enzyme-linked immunosorbent assay ELISA Kit (Novatein Bioscience manufacturer USA, catalogue number: BG-HUM11612, 96 wells). Human B-ALP concentration was quantified using the Eliza Kit (Novatein Bioscience manufacturer USA, catalogue number: NB-E10824, 96 wells). OC was measured using the Naovateinbio hOST-EASI Kit (catalogue number: NB-E10875, 96 wells). The Naovateinbio hOST-EASI Kit is a solid phase EASIA, performed on a microtiter plate.
Statistical analysis
All statistical analyses for the study were performed using Data Analysis and Statistical Software; STATA (version 13) StataCorp, LP, Texas, USA. Data were evaluated for normality of distribution. Descriptive statistics were then calculated for all variables, using the mean and standard deviation (SD) for normally distributed data and the median and range for data with a skewed distribution. Correlation between T-scores and bone markers was performed. One-way analysis of variance (ANOVA) test was used to assess a difference in mean T-scores normally distributed variables, whereas non parametric (Mann-Whitney test) was used with other skewed distributed continues variables. Chi-squared test and Fisher’s exact test were used, when appropriate for the data set, to assess association of BMD and categorical variables. For all analyzes, a p<0.05 was considered to be significant. crude and adjusted odds ratio (OR) with 95% confidence interval (CI) of risk factors associated with a low BMD were estimated using multivariate logistic regression.
Results
The study included 304 Saudi women, 20 to 36 years old. All participants enrolled in the study completed the questionnaire and QUS assessment components of the study. Of these, 25 questionnaires were not completed in their entirety and the data from these participants were excluded from the analysis. The median age of the 279 participants included in the final analysis was 27 years (25th percentile was 22 and 75th percentile was 32). The overall prevalence of low BMD among our study group was 9% (25/279), out of which 3% (8/279) were identified as having osteopenia and 6% (17/279) as having osteoporosis.
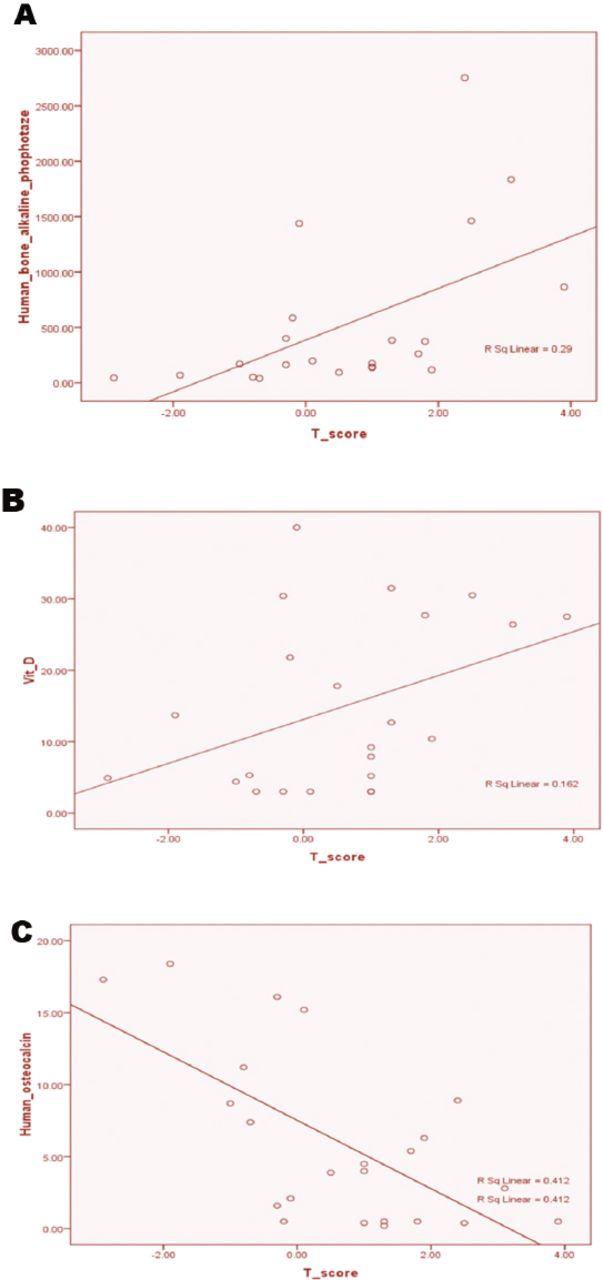
The distribution of socio-demographic characteristics for our study group is reported in Table 1, with key features summarized as follows: approximately 2-thirds of our participants were <30 years old and had higher education; 94% (254/260) lived in the city; approximately 60% of participants were clerks or students; 47% were single; 49% had a moderate economic status; and 48% a high economic status. The distribution of Z-scores and biochemical measures is reported in Table 2. Both vitamin D and plasma OC levels were consistently lower in our study group, copmared with the norm-referenced standard. The median vitamin D level was 10.4 ng/ml, with the 75th percentile still below the norm-referenced standard at 27.5 ng/ml. The median plasma OC level was 1.47 ng/ml and, again, the 75th percentile value of 4.5 ng/ml was still below the norm-referenced standard. All other blood biochemistry measures were within normal standard range. Non-parametric evaluation of differences between the normal and low BMD groups is also reported in Table 2. Significant between-group differences were identified for Z scores (p=0.001) and OC levels (p=0.01). No significant between-group differences were identified for levels of vitamin D, serum calcium, and OPG, as well as human B-ALP concentration. Levels of serum phosphorus were also comparable between groups (F-test=0.86, degree of freedom (DF)=2, 20; p=0.44). The correlations between the T-scores of BMD and the biochemical parameters are shown in Figure 1. The T-scores were positively correlated with human B-ALP concentration (r =0.58; p=0.01) and vitamin D levels (r =0.40; P <0.05). OC levels were inversely correlated with T-scores (r =-0.65; p=0.001) Figure 1A. The overall prevalence of low BMD was 9% (25/279). Middle and lower level of education were merged together in Table 3, because the number of low education group was only 4 individuals. Low BMD was found more among: early and late period of peak bone mass age, 10.6% copmared with 5.6. It was 14% among women with low-to-no sun exposure and 8% among women with a low dietary intake of calcium. Also a higher prevalence of low BMD was identified among women with DM (37.5%),(Table 3).
Socio-demographic characteristics of the participants. (n=304)
Biochemical and bone markers characteristic of the participants by bone mineral density (BMD).
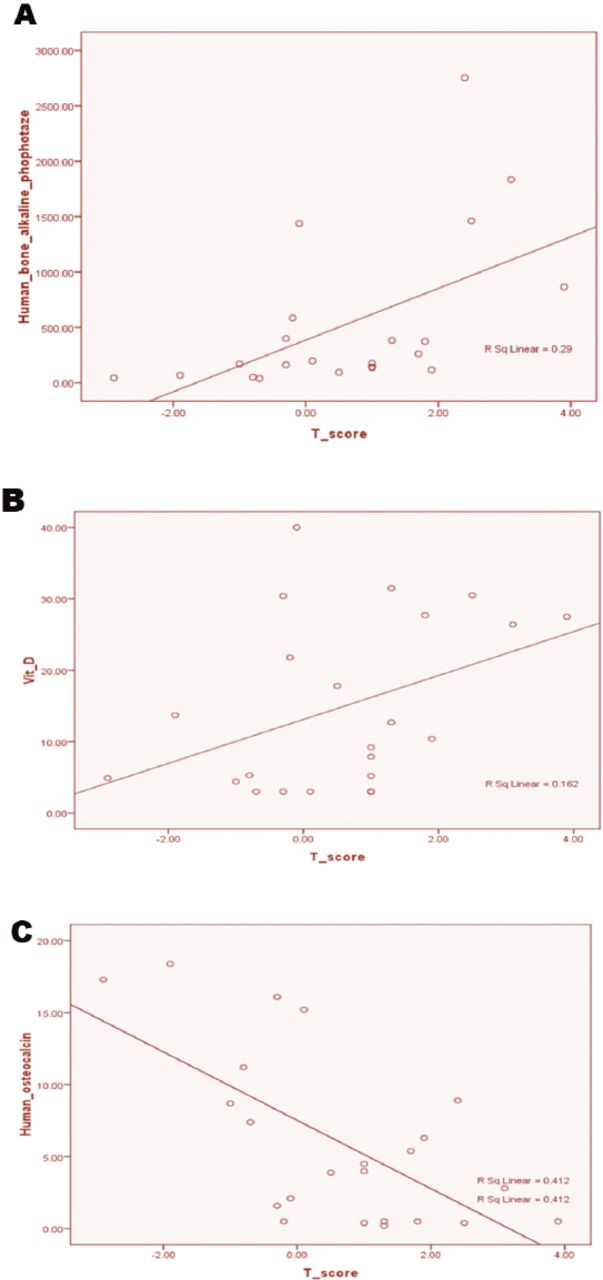
The correlations between the T-scores of bone mineral density and the biochemical parameters: A) correaltion of T-score with Human bone alkaline phosphtase, B) correaltion of T-score with vitamine D, and C) correlation of T-score with human osteocalcin.
Univariate regression analysis between low bone mineral density (BMD) and socio demographic and life style.
Risk factors quantification and effect was summarized in (Table 3 & 4). The crude odds ratio (crude OR), evaluated by univariate analysis in (Table 3 & 4), revealed that 8% of low BMD was found among women with low dietary intake of calcium <1000 mg/day, however at any point in time low BMD was 5 times more likely among lower intake calcium group copmared with normal (crude OR 5.05 (1.74, 14.65); p=0.005). Low BMD was 14% among those who did not expose to sun compared with 5% among those who did expose to sun. It was 3 times more among those who did not expose to sun (3.32, 95% CI=1.27, 8.66).
Univariate regression analysis of low bone mineral density (BMD) with clinical risk factors.
There was no evidence of an association between socio-demographic factors (age, area of residence, occupation, marital status, educational level, and household income), lifestyle factors (physical activity and outdoor covering of the body and face) and other clinical risk factors (smoking, BMI, hypertension, history of fractures, thyroid diseases, use of steroids, use of oral contraceptives, age at menarche, regularity of menstrual cycle, and development of low BMD. The adjusted ORs for low BMD as a function of the evaluated factors, after adjustments for confounding factors, are reported in Table 5. At any given point in time the exposed subject to low calcium in the population are 11 times more likely to have low BMD, (adjusted OR, 11.0; 95% CI: 3.16, 38.34; p=0.001). For those with low sun exposure were more than 3 times more likely to have low BMD (adjusted OR, 3.32, 95% CI: 1.27, 8.66, p<0.01). Although those with DM were 6 times more likely to have low BMD compared with non-diabetic, but when adjusted for other confounding variables, there was no evidence to reject the null hypothesis of no difference in BMD between them (adjusted OR and 95% CI: 5.12(0.88, 29.770 and p=0.07).
Multivariate logistic regression, reporting the adjusted odd ratios between low bone mineral density (BMD) and calcium intake, exposure to sun and diabetes mellitus.
Discussion
The overall prevalence of low BMD was 9% (25/279), with 6% for osteopenia and 3% for osteoporosis. A similar cross-section study, conducted in Al-Khobar et al7 reported a prevalence rate of 11.9% for osteoporosis and 24% for osteopenia among a comparable group of young women in their peak bone mass age. Using QUS to compare bone quality in pre- and post-menopausal women working at King Saud University in Riyadh, Kingdom of Saudi Arabia, Mahboub et al14 reported a prevalence rate of osteopenia of 30.1% and a low prevalence rate of osteoporosis of 6.5%. Alghannam et al15 used DEXA to screen bone quality in 321 healthy Saudi women, reporting a prevalence rate of osteoporosis of 0-7% among women ≤31 years of age, with a higher prevalence rate of osteopenia of 18-41%. These studies in general confirm our findings of a higher prevalence rate of osteopenia than osteoporosis among women in a younger age group. The prevalence of osteopenia was much less in our study as one third of our study group was between the ages of 25 and 30 years (PBM age) and with lower prevalence of low BMD than reported by Alghannam et al.15 However, the identification of osteopenia in this young age group (namely, ≤36 years of age) remains an important health issue, being a predisposing factor for osteoporosis and increasing the risk fractures at a later age. Our findings of low serum levels of 25-OHD vitamin D (Table 2 & Figure 1) corroborates findings from 2 previous studies16,17 that have reported vitamin D insufficiency to be a common risk factor for osteoporosis. We also identified a negative correlation between T-scores and OC levels (Table 2 & Figure 1), with the OC level in the group with a low BMD being significantly higher than in the group with normal BMD (p=0.01). Our results, which are indicative of a higher level of bone demineralization, are comparable with a recently reported negative correlation between serum OC levels and BMD in a study conducted in Northern India,18 it concluded that higher OC levels could be used for screening purpose in post-menopausal women, with further assessment using DEXA if indicated. It is worth stating that in interpretation of bone markers results, other bone disease like metastases need to be excluded.
Although we had anticipated an association between a low BMD and socio-demographic factors, namely age, education, marital status, and household income, we found no evidence of such an association (Tables 3 & 4). A systematic review19 concluded that there is limited evidence of a positive association between educational level and BMD in women, with no evidence of an association between household income or occupation and BMD, regardless of gender. Subjects who experienced inadequate exposure to the sun were at higher risk of getting low BMD (Table 5). This result could reflect a vitamin D deficiency due to low sun exposure, with vitamin D insufficiency being a significant risk for low BMD, regardless of calcium intake. A previously published study20 presented evidence of widespread vitamin D deficiency among different groups of the Saudi population, with explanations varying from a low dairy intake, inadequate vitamin supplementation, and low sun exposure due to the very hot climate. A comparable study conducted in Lebanon21 provided evidence that wearing a veil was predictive of low vitamin D level. Although crude analysis explored a role of diabetes in low BMD, adjusted result showed no evidence of role. However, a recent study22 reported low BMD among post-menopausal Saudi women with type-2 DM. Another recent study,23 also conducted in Saudi Arabia, evaluated plasma levels of bone metabolism markers in children with type-1 DM, reporting a lower BMD among this clinical population copmared with age-referenced normative values.
The finding of this study, if linked to the results of previous studies may reflect the growing biological role of DM in the development of low BMD. An important result of our study is exploring the role of low dietary intake of calcium and low sun exposure in the development of low BMD that needs further analytical studies to asses their effect as a modifiable risk factors.
The limitations of our study need to be acknowledged in the interpretation and application of our results. Foremost, we used a cross-sectional design and, therefore, causation and temporal sequences of events cannot be determined since the outcome and determinants are measured simultaneously. We conducted our study with a specific population at Taibah University, therefore, our results cannot be generalized to other populations with confidence. One shortcoming is that blood samples of all subjects should have been analyzed, which if performed would have increased the authenticity of this work, but due to logistic reasons, the investigators could not find bone markers in the local market, and it took a long time to import from abroad, and when they arrived only 23 participants remained to be studied. We conducted our study with a specific population at a university level as a community institute that included the targeted age group ranging from 20-36 years old, but they may not represent the community at large as the results showed very high level of education of the participants, and also high household income and low percentage of housewife that may not reflect and represent the situation in the community, therefore, our results can not be generalized to other populations with confidence. In spite of the previously mentioned limitations, our findings are supported by other studies, as discussed previously.
In conclusion, young adult Saudi women are not exempted from low BMD, which necessitates an urgent introduction of screening program for young Saudi women at university and community levels. This study identified low levels of vitamin D and OC indicative of bone demineralization, among a specific group of young Saudi young, ≤36 years old, which were largely explained by low dietary calcium intake and low sun exposure. Osteocalcin could be used as a biomarker in screening of low BMD in young adult women, however, further large size analytical studies should be considered. We also identified an important role of DM in the development of low BMD in young women. Our findings were consistent with previously reported studies, emphasizing the importance of incorporating mitigating strategies for these risk factors in future prevention programs for low BMD in young women. Prospective longitudinal studies are needed to confirm our findings and to evaluate the effectiveness of risk mitigating strategies for prevention of low BMD among young adult Saudi women.
Withdrawal policy
By submission, the author grants the journal right of first publication. Therefore, the journal discourages unethical withdrawal of manuscript from the publication process after peer review. The corresponding author should send a formal request signed by all co-authors stating the reason for withdrawing the manuscript. Withdrawal of manuscript is only considered valid when the editor accepts, or approves the reason to withdraw the manuscript from publication. Subsequently, the author must receive a confirmation from the editorial office. Only at that stage, authors are free to submit the manuscript elsewhere.
No response from the authors to all journal communication after review and acceptance is also considered unethical withdrawal. Withdrawn manuscripts noted to have already been submitted or published in another journal will be subjected to sanctions in accordance with the journal policy. The journal will take disciplinary measures for unacceptable withdrawal of manuscripts. An embargo of 5 years will be enforced for the author and their co-authors, and their institute will be notified of this action.
Acknowledgment
The authors gratefully thank the Deanship of Research at Taibah University, for providing financial support for our study. The authors would also like to thank all participants in this study.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company, This study was funded by the Deanship of Research at Taibah University, Al Madinah Al Munawwarah, Kingdom of Saudi Arabia (Grant no. 1539/434).
- Received July 21, 2016.
- Accepted August 17, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.