


Abstract
Well-recognized for their role in vascular homoeostasis, platelets may play a major role in inflammation and immunomodulation. Substantial data are emerging on the pathogenic involvement of platelets in inflammatory arthritis and autoimmune diseases, indicating the existence of crosstalk between the coagulation and inflammation system. Upon activation, platelets release pro-inflammatory platelets microparticles, which interact with leucocytes leading to joint and systemic inflammation in rheumatoid arthritis. Platelets activation by immune complexes activate dendritic cells promoting the secretion of interferon alpha, which has a key role in the development of systemic lupus erythematous. In this review, we discuss the current data on the role of platelets in the pathophysiology of inflammatory arthritis and various autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematosus, and systemic sclerosis.
In addition to the well-established pivotal role of platelets in hemostasis and thrombosis, a growing body of evidence implicates platelets in inflammation responses.1-3 In particular, recent studies have uncovered a novel platelet contribution to disease pathophysiology in inflammatory arthritis and autoimmune diseases.4,5 If the role of platelets in inflammatory arthritis is confirmed, this would have major prognostic and therapeutic implications. This review aims to analyze current evidence of platelets’ role in inflammatory rheumatic diseases and overview the potential role of platelets as a target of antirheumatic drugs.
1) Pathogenic role of platelets in inflammation. a) Platelets and systemic inflammation
Inflammation and coagulation are closely linked with inflammation tilting the homeostatic balance towards thrombosis and promoting the development of cardiovascular morbidity.6,7 Indeed, inflammation, by creating an imbalance of the normal physiologic anticoagulant mechanisms, induces activation of the coagulation system with interleukin (IL)-6, and tumor necrosis factor-alpha (TNF-α) as major players. Severe inflammatory responses, specifically in sepsis are associated with increased platelet activation in the bloodstream. Stimulated platelets actively synthesize proinflammatory cytokines, including IL-1. The IL-1 contributes to coagulation and fibrinolytic system activation and the release of more proinflammatory mediators in the early response to severe infection.5,6 Activated platelets bind other platelets and leukocytes in the bloodstream setting off a cascade of events that contribute to the development, evolution, and resolution of the systemic inflammatory response. The activation of the coagulation cascade and the excessive consumption of platelets in the microcirculation during severe sepsis might induce disseminated intravascular coagulation (DIC) and thrombocytopenia.7 However, it is now well accepted that platelets function in non-traditional ways. Indeed, upon activation, platelets release not only the proinflammatory mediators stored in their granules, but also other proteins newly synthetized in response to extracellular activation. Interactions between platelets and leucocytes are important for their mobility, but they also serve as channels for molecular signaling.8,9 In fact, activated neutrophils externalize structures combining chromatin with bacterial proteins named neutrophil extracellular traps (NETs). The NETs contribute to ensure bacterial clearance.10 Both in vitro and in vivo studies have shown that activated platelets adhering to neutrophils can initiate NET formation.11,12
b) Platelets and joint inflammation
Rheumatoid arthritis (RA) is irrevocably the condition where joint inflammation mechanisms were the most studied. So far, evidence has implicated immune cells as the major actors in RA pathophysiology. Until recently, platelets have not been expected to have a role in this field. Preliminary evidence on the involvement of platelets in rheumatoid inflammation was provided by flow cytometric analyses that have detected a substantial number of marked small platelets particles in RA synovial fluid.4 These platelet microparticles (MPs) are small membrane-coated vesicles that are released from the plasma membrane upon platelet activation. They contain cytoskeletal proteins, membrane receptors, and signaling molecules.6
Pro-inflammatory platelets MPs generation by interaction with exposed extracellular matrix
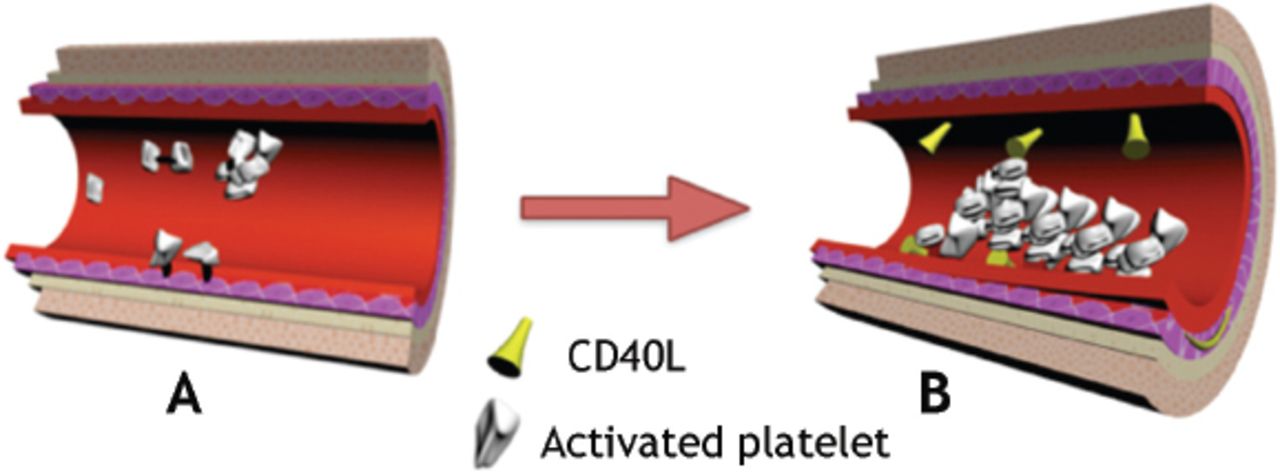
The first step in platelet activation is interaction with the exposed extracellular matrix (ECM) at sites of injury (Figure 1). Among the macromolecular constituents of the ECM, collagen is considered to play a major role in this process, as it not only supports platelet adhesion, but it also directly activates the cells initiating aggregation and coagulant activity. Platelet adhesion and aggregation on collagen involves several platelet agonists that act through a variety of surface receptors, including integrins, immunoglobulin (Ig)-like receptors, and G-protein-coupled receptors.13 Glycoprotein VI (GPVI) is one of the major signaling receptor for collagen on platelets.14 Boilard et al,4 identified the collagen receptor GPVI as a key trigger for platelet microparticle generation in arthritis pathophysiology, and demonstrates collagen receptor GPVI-dependent stimulation of IL-1 containing MPs as a relevant disease pathway in synovitis. The signaling process by which engagement of collagen receptor GPVI expressed on platelets, triggers MPs generation is not clearly understood, but has been recently suggested to involve a spleen tyrosine kinase: Bruton’s tyrosine kinase (BTK), best known as an essential element in B-cell receptor signaling.15

An image showing: A) interaction with the exposed extracellular matrix, production and release of microparticles from the platelet membrane, adhesion of platelets to each other, and to endothelial cells; and B) platelets complexes with other cells, aggregation, and binding with CD40 ligands (CD40L).
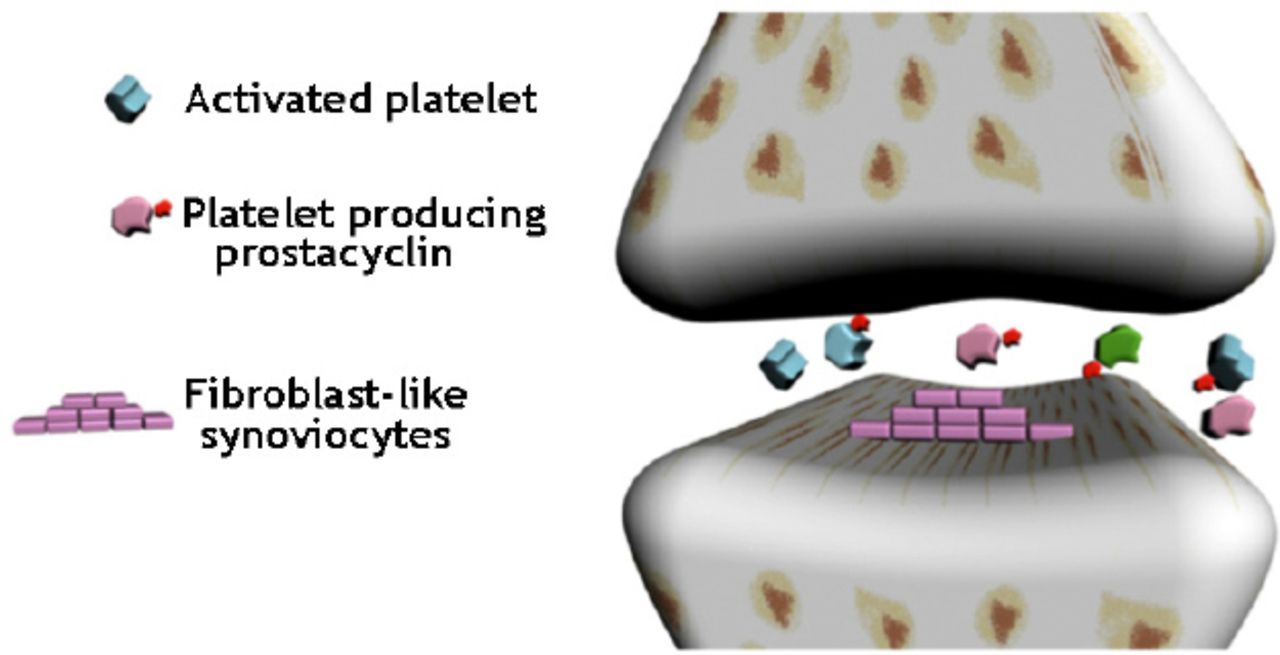
Mechanistically, platelet activation via the collagen receptor GPVI stimulates production and release of MPs from the platelet membrane. These platelet-derived MPs are detectable at high levels in the synovial fluid,16 and seem to have a major role in local elaboration of cytokines, such as IL-1, and thus, amplify joint inflammatory response. In addition, MPs can interact with and activate fibroblast-like synoviocytes (FLS), which are important effector cells that mediate both immune activation and joint destruction (Figure 2). Platelets exhibit membrane-associated IL-1 activity. Both forms of this cytokine are present in MPs, although IL-1α is predominant. Both forms of IL-1 participated in human FLS stimulation because neutralization of platelet MP IL-1 activity required blocking antibodies against both IL-lα and IL-lβ.4

An image showing synovial platelets, platelets/leucocytes interaction, and exit from the vasculature, interaction with fibroblast-like synoviocytes and production of proinflammatory prostacyclin.
Pro-inflammatory platelet MPs production and migration in the joint
Platelet activation seems to be essentially an intra-articular process, wherein the MPs role is to diffuse platelet-derived cytokines into the inflamed joint. Knowing that neither platelets nor their MPs’ have migratory properties, their accumulation in arthritic synovial fluid raises the question of how do they invade the synovium? One of the most plausible hypothesis is their transportation by leukocytes.17 Indeed, platelets/leucocytes interaction in RA has been reported in several studies; platelet adhesion to leukocytes in blood circulation enhance leukocyte rolling on the endothelial wall, and leucocytes can facilitate the transport of platelets to the joint space.18,19 Another hypothesis is the presence of gaps in the arthritic joint vasculature, which allows platelets MPs with their submicron diameter to exit the vasculature.20 Unexpectedly, platelets, which are usually seen as the guardians of vascular integrity, release locally serotonin that helps drive the persistent vascular permeability that characterizes the microvasculature of the inflamed synovium.19,20
Pro-inflammatory platelet MPs independent mechanism in arthritis
Boilard et al4 demonstrated that platelets are directly involved in synovial inflammation via production of pro-inflammatory prostacyclin. Using a Cox-1-dependent mouse model of inflammatory arthritis, they showed that platelet Cox-1 expression is sufficient to generate an active synovitis. Interestingly, this pathway operates without generation of MPs and seems to be another mechanism, totally-independent, by which platelets can contribute in arthritis pathophysiology. Prostacyclin generation by platelets can be activated by transcellular communication between platelets and FLS.21 Furthermore, Habets et al22 suggested that platelets activation can be mediated by anti-citrullinated protein antibodies (ACPA) in the very early stages of RA. They showed that incubation of platelets from healthy subjects with plasma derived from RA patients induces platelets activation, and that this activation correlated with disease’ activity and the percentage of ACPA among the total IgG.22 Platelets from RA patients express higher P-selectin levels and produce higher amounts of soluble CD40 ligand (sCD40L). The P-selectin expression and secretion of sCD40L are both markers of platelet activation. Interestingly, levels of P-selectin expression and sCD40L release correlated with high ACPA titers.22 In fact, these results point to a new paradigm, whereby platelets represent a key player in joint inflammation pathophysiology.
2. Pathogenic role of platelets in immunomodulation. a) Pathogenic role of platelets in systemic lupus erythematosus (SLE)
Strong evidence pointing to platelet activation during SLE has been reported. Platelet activation seems to be mediated by the interaction of circulating immune complexes with platelets Fc receptors.19 Increased complement deposition on platelets has also been described in SLE. Especially in patients with a history of venous thrombosis, elevated levels of C1q, C3d, and C4d are present on platelets.23 The level of platelet bound C4d correlates with disease activity and associates with the presence of antiphospholipids.24 Upon activation by immune complexes, platelets promptly associated with myeloid and plasmacytoid dendritic cells, promoting the secretion of interferon (IFN), which has a key role in the development of SLE by activating dendritic cell differentiation.19
The autoimmune reactions and abundant production of antibodies directed against blood cells, including platelets are thought to contribute to platelet activation, release of vasoactive and thrombogenic agents, and accelerated atherogenesis in SLE. Antibodies targeting platelet surface proteins were identified and linked to thrombocytopenia in SLE.25 Serum sCD40L is a marker for vascular inflammation and its role in atherothrombosis is now widely accepted.26 The CD40L and its soluble form (sCD40L) belongs to the TNF superfamily. They are molecules with a dual prothrombotic and proinflammatory role. The CD40L is a transmembrane protein originally identified on activated T cells as the ligand for CD40, a molecule that triggers B-cell and dendritic-cell activation. Its soluble form, sCD40L, is more abundant in patients with SLE and promotes disease activity. Platelets are a major source of sCD40L. Enhanced platelet activity and increased serum sCD40L have been observed in SLE patients, suggesting an important role of platelets in SLE.27 Duffau et al28 have demonstrated that platelets CD40 ligand (also called CD 154) enhance IFNa secretion by immune complex-stimulated plasmacytoid dendritic cells in SLE. Furthermore, depletion of platelets improved all measurements of disease activity and overall survival in lupus prone mice. The beneficial effects of statin treatment, which next to its lipid-lowering effect has a series of anti-inflammatory effects, including a reduction of platelet reactivity and sCD40L, has been confirmed in 2 randomized double-blind placebo-controlled clinical trials.29,30 Together, these data suggest that platelet activation and complement deposition on platelets might be useful biomarkers for venous thrombosis in SLE patients.
b) Pathogenic role of platelets in systemic sclerosis
In systemic sclerosis (SSc, scleroderma), a disease in which microvascular involvement is an important pathogenic leitmotif to some of the main clinical features, platelets contribution seems to be substantial. The link between platelet activation and vascular injury in SSc is not fully understood. Basically, the vascular damage with exposure of subendothelial connective tissue results in ongoing activation of platelets.31 Loss of the anticoagulant properties of the endothelial cell layer results in platelet activation and the release of bioactive molecules, such as platelet factor 4, platelet-derived growth factors, and b-thrombomodulin.32 Moreover, recent studies indicate that platelets release high-mobility group box 1 (HMGB1), a hallmark of necrosis in the vasculature of SSc patients, contributing to persistent microvascular injury and endothelial cell activation.33 On the other hand, plasma samples from patients with SSc contain a supranormal subset of von Willebrand factor, which can induce platelet aggregation and adhesion to the subendothelium.34 Interestingly, SSc platelets were recently found to over-express a specific receptor for type I collagen.35 Platelets have surface receptors for collagen I and collagen III. Over-expression of a type I collagen receptor would be expected to increase platelet aggregation to collagen I, and may make SSc platelets susceptible to increased aggregation and microthrombi formation, characteristics of SSc.32
Platelet activation plays also an important role during skin and lung fibrosis. Dees et al31 showed that serotonin (5-hydroxytryptamine [5-HT]) stored in platelets strongly induces extracellular matrix synthesis in interstitial fibroblasts in a transforming growth factor (TGF) β dependent manner. Thus, platelet-derived serotonin links vascular disease and tissue fibrosis in SSc. Microvascular vasoconstriction observed in SSc is mainly mediated by defective synthesis of endothelial prostacyclin (PGI2).36 Given that PGI2 is a strong inhibitor of platelet activation, the reduced PGI2 production combined with the sustained collagen stimulation followed by the production of thromboxane A2 (TXA2) have a positive feedback for platelet activation.37 In conclusion, the microangiopathy characteristic of SSc leads to a strong platelet activation, which is involved in both tissue fibrosis and inflammation via various platelet-derived mediators.
3. Platelet parameters in inflammatory arthritis and autoimmune systemic diseases. Clinical data
Some platelet markers, including mean platelet volume (MPV), a simple indicator of platelet size and activity, has been investigated to be correlated with inflammation. However, platelet markers significance is not well established and their study is not performed routinely.
a) Rheumatoid arthritis and Spondyloarthropathies
The MPV is significantly lower in both RA and ankylosing spondylitis (AS) patients with active disease as compared with controls.38 Other studies have shown that MPV is correlated with clinical disease activity indices in both RA and AS patients.38,39 Moreover, platelet indices were substantially decreased after therapy. Both anti-TNFa and conventional therapy decreases markers of inflammation and platelet indices in RA and AS patients.39,40 In another study, MPV levels were found increased in patients with psoriasis and psoriatic arthritis when they were compared with healthy subjects. The MPV was suggested to be a marker for the severity of psoriasis.41
b) Primary Sjogren syndrome
In primary Sjogren syndrome, patients showed increased plasma level of total MPs, and platelet MPs level was inversely correlated with antiserum beta 2 microglobulin level.42 Additionally, platelet serotonin level was found to be significantly lower in comparison with healthy controls.43
c) Behçet disease
The MPV changes have also been investigated in Behçet’s disease. It has been shown that an increase of MPV may indicate a thrombotic tendency in Behçet patients,39 but MPV does not seem to be an appropriate marker of activity in this condition.44,45
d) Familial Mediterranean Fever (FMF)
Similar observations were also made on patients with FMF.46 Interestingly, in FMF patients, the MPV was lower in comparison with healthy controls, either during the attack periods or during attack-free periods. Classically, there is an inverse relationship between the number of circulating platelets and their MPV, therefore, the lower MPV level is an expected result of secondary thrombocytosis in FMF patients.47 Overall, it seems that high-grade inflammation is associated with a decrease of MPV in inflammatory disorders, probably due to the high consumption of platelets at the sites of inflammation, whereas this observation is reversed when the same diseases are controlled with anti-inflammatory drugs.48
e) Osteoarthritis
Interestingly, in non-inflammatory disease, such as knee osteoarthritis, a significant difference has been found between MPV levels in patients with knee osteoarthritis with associated synovitis when compared with those with knee osteoarthritis without synovitis.49 This could be an additional argument to support the “local” fashion of platelet activation in the joints.
4) Platelets, inflammation, and cardiovascular morbidity
For a long time, it was thought that the role of platelets is limited to the final step of atherosclerosis, namely the rupture of the plaque followed by thrombotic narrowing, or occlusion of a vessel. In fact, during the long course of atherosclerotic disease, platelets play a pivotal role at all stages as they contribute to the initiation of the atherosclerotic lesion, to its progression and acute disease exacerbation.50 Thus, platelet adhesion to the endothelium under inflammatory conditions is critical for the initiation of atherosclerotic plaque formation. It induces recruitment of proatherosclerotic cells and release of proinflammatory mediators from all involved cell types. Platelet factor 4 (PF4), which is a highly abundant chemokine in platelets granules, has been linked to atherosclerotic lesions severity.50,51 The PF4 attracts monocytes and induces their differentiation into macrophages.52 Furthermore, PF4 directly promotes atherosclerosis by the inhibition of LDL catabolism and enhancement of oxidized low density lipoprotein uptake by macrophages. In advanced atherosclerosis, platelets have a role in plaque rupture and microembolic events.50 In fact, platelet participation in inflammatory diseases has been studied most extensively in the context of atherosclerosis, in which activated platelets promote endothelial cell activation, as well as leukocyte adhesion and transmigration via release of different mediators that includes IL-1, sCD40L, matrix metalloproteinases 2 and 9, amine serotonin, platelet-derived growth factor, and the prostanoid TxA2.53
Accelerated atherosclerosis is the main contributor to premature mortality in RA patients. Recently, platelet-derived MPs and other markers of platelet activation were recognized as not only triggers of arthritis, but also an essential link between RA and accelerated atherosclerosis.54 Platelet activation indeed could be a link in the pathophysiology of diseases prone to thrombosis and inflammation. In a clinical point of view, numerous platelet markers, including MPV have been investigated in connection with both thrombosis and inflammation. A meta-analysis performed in order to determine whether an association exists between MPV and cardiovascular events has shown that elevated MPV is associated with acute myocardial infarction and mortality following myocardial infarction.55 Thus, MPV was suggested to be a potentially useful prognostic biomarker in patients with cardiovascular disease. Moreover, in another large cohort study, hypertension was a strong predictor of high MPV in RA patients.56 Traditional cardiovascular risk factors, such as smoking, hypertension, diabetes, as well as age and gender can modify shifts of MPV, affecting the expected inverse relationship between MPV and platelet count seen in inflammatory thrombocytosis.48
5) What would be the therapeutic consequences of these findings in a translational perspective?
The first question that arises is whether the available platelet inhibitors, such as aspirin and clopidogrel, could influence arthritis. Surprisingly, clopidogrel has been implicated in several cases of spontaneous acute inflammatory arthritis.57,58 A possible explanation could be that platelet activation pathways involved in thrombosis and those involved in inflammation are not quite the same. Thus, the drugs currently used in the context of thrombosis are not necessarily efficient in the context of arthritis and may even aggravate the disease. Inflammation-induced thrombosis may respond to immunosuppressive treatment, as in the case of Behçet disease. However, effectiveness of this treatment cannot be generalized to all other inflammatory diseases. Reciprocally, there is now growing evidence that antiplatelet agents, such as clopidogrel, also have some anti-inflammatory activity.59 This complex reciprocal crosstalk between inflammation and hemostasis is one of the topics of high interest in rheumatology nowadays.
Furthermore, a better understanding of the signaling and activation pathways of platelets may lead to new and innovative therapeutic pathways. The previously exposed experimental data are substantially relevant for human disease. On the one hand, mice or humans lacking GPVI remain healthy; antagonism of this receptor represents a novel therapeutic approach.14 On the other hand, the potential therapeutic utility of BTK inhibitors in RA therapy, by inhibiting GPVI-mediated platelet activation is now supported by potent experimental data.15 Experimentally, membrane-associated MP IL-1 was unusually difficult to antagonize.4 This observation may help to explain the limited effect of IL-1 blockade in RA,60 and the prominence of IL-1α within MPs poses potential constraints on the efficacy of IL-1β-specific agents. Moreover, The unexpected paracrine pathway whereby platelets participate in synovitis via Cox-1-dependent synthesis of prostacyclin should probably make us reinvest the pharmacologic inhibition of prostanoid production in the treatment of inflammatory arthritis.
Since platelets activation is correlated with disease activity in RA, and given the importance of platelets and platelets MPs in cardiovascular diseases, this may be one reason for the enhanced cardiovascular morbidity and mortality in RA. Therefore, targeting platelets pathways would be probably interesting not only to control the disease itself, but also to reduce the related cardiovascular risk. In an era, in which all biologics compete to demonstrate a protective effect for cardiovascular disease, targeting platelets seems to be a very attractive therapeutic approach.
In conclusion, not long ago, the role of platelets was thought to be limited to hemostasis and thrombosis. However, abundant new insights into the pathogenic contribution of platelets and MPs in inflammatory and immune joint responses have changed this dogma. However, the mechanisms elucidated to date explain only a part of platelet contribution to autoimmune diseases and other pathways linking, platelets to immunomodulation await discovery. This would allow a better understanding of autoimmune diseases pathophysiology, and open new therapeutic perspectives. A new set of biological targets is probably on the way to emerge.
Acknowledgment
The authors gratefully acknowledge Mr. Eihab Kamal Zain for his help in drawing the figures.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.