


Abstract
Objectives: To describe the patterns of childhood cancers in Hadhramout Sector, Yemen between January 2002 and December 2014.
Methods: This descriptive retrospective study was based on secondary data from Hadhramout Cancer Registry, Hadhramout, Yemen. All Yemeni children under age of 15 years, who were diagnosed with cancer were included. The International Childhood Cancer Classification system was used to categorize cancer types.
Results: A total of 406 childhood cancers of both gender <15 years of age were reported. These represented 8.5% of all cases registered. The mean age was 7.34 ± 4.18 years. There were 240 males (59.1%) and 166 females (40.9%) with a male to female ratio of 1.4:1. Calculated incidence of cancer in children in this population is 1.9 per 100,000. The predominant age group was 5-9 years (35%) followed by 10-14 years (33.7%), and 0-4 years group (31%). The most common group of malignancies were hematological malignancies accounting for 47% of cases, followed by nervous system malignancies (15%). The most frequently reported cancer types were lymphoma (24%), leukemia (23%), carcinoma (13.1%), and central nervous system (CNS) tumors (11.6%).
Conclusions: There is a lower frequency of childhood cancer in Hadhramout Sector when compared with developed countries. The most common cancers among children were lymphoma, leukemia, carcinoma, and CNS tumors.
Pediatric malignancies affect more than 175,000 children younger than 15 years annually and account for 1.4% of all cancers worldwide.1,2 In Yemen, although there is no proper cancer registry, available data shows that approximately 753 cases of childhood malignancies were detected with an annual incidence of 34 cases. The calculated incidence of cancer in children in this population is 1.9 per 100,000. The most common types of cancers reported in Yemen are leukemia, lymphoma, and central nervous system (CNS) tumors.3-5 The cancer registry is considered the corner stone for the documentation of basic data of cancer patients and an entry into a computerized register, and this is considered as an initial step in the establishment of the epidemiology of cancer.6,7 Cancer registries are currently available in many Arab countries, including Yemen.8 Hadhramout Cancer Center (HCC) was established by the Ministry of Healthin 2002 to serve people in the Hadhramout sector, which consists of 3 governorates (Hadhramout, Shabwa, and Almahra) with a population of approximately 1,820,163 inhabitants, and children <15-years-old represent 46% from Hadhramout setor population.9 This study was conducted to describe the problem of cancer, and to assess the prevalence and pattern of different types of cancer by age distribution and gender among Yemeni children in Hadhramout sector, Yemen during a 13 years period from January 2002 to December 2014
Methods
This descriptive retrospective study was based on secondary data from Hadhramout Cancer Registry (HCR). The collected details were entered into the computerized package CanReg510 (Software for cancer registries) and revised for any duplication or incompleteness. Validation of data was carried out by the computer system on each data item to ensure that no invalid codes are fed into the database. Confidentiality of the received data is one of the important tasks of the working group.
Neoplasms are coded and classified according to the International Classification of Diseases for Oncology (ICD-O).11 and the 10th revision12 An updated childhood classification allows the new and expanded coding of cancer, which have been introduced.11 It has to be noted that upon establishing HCR, data from Hadhramout Cancer Center were retrospectively entered into the newly established electronic registry using the data from the paper charts. In this study, the basic epidemiologic data was retrieved from the records of children with cancer who were <15 years of age at diagnosis, who were diagnosed between January 2002 and December 2014. Analysis included identification of the patient demographic characteristics, gender, age, year of diagnosis, site, morphology, histology, and topography of cancer, and place of residence.
Different types of pediatric malignancies were grouped into 12 major diagnostic groups with further sub-classification according to the International Classification of Childhood Cancer (ICCC) into 3 age-groups: 0-4 years, 5-9 years, 10-14 years.13,14 Data was reviewed for incompleteness or missing entries; any registered case with incomplete or missing data was excluded from the study.
Sample size
A total of 406 children <15 years of age with cancer registered in HCR from January 2002 to December 2014. Inclusion criteria were cancer children aged <15 years with complete registered data. Exclusion criteria were cancer children >15 years old, and children <15 years old with incomplete registered data.
Ethical considerations
The research protocol was conducted according to the principles of the Helsinki Declaration, as well as reviewed and approved by the College Ethical Research Committee. There was no need for informed consent from patients because the data was secondary data with no linking to patient identity.
Statistical analysis
The data were processed and analyzed using the Statistical Package for Social Sciences for windows version 16 (SPSS Inc, Chicago, IL, USA). Statistical analysis included quantitative descriptive analysis and summary statistics for describing the frequency of diagnostic group and subgroups of childhood cancer. Quantitative analysis of the studied variables included Chi squares, Fischer exact test, and rates stratified by gender and age. We also used data from previous publications to compare the frequency of different cancer types registered from Aden,3,4 Sanaa,5 and the Surveillance, Epidemiology, and End Results (SEER) Program and SEER*Stat Database of the National cancer institute, USA that works to provide information on cancer statistics.15
Results
A total of 406 childhood cancers of both gender, comprising 8.5% of all malignancies (n=4796)that were registered in the HCR from January 2002 to December 2014. The mean age was 7.34 ± 4.18 years. There were 240 (59.1%) males and 166 (40.9%) females with a male to female ratio of 1.4:1. The highest frequency was reported in the 5-9 years group (n=143, 35.2%) followed by 10-14 years group (n=137, 33.7%), and 0-4 years group (n=126, 31%) as shown in Tables 1 & 2. When different cancer groups were evaluated, the most common group was hematological malignancies, followed by nervous system malignancies. The most frequent cancers among children based on the ICCC were lymphoma (24%), leukemia (23%), carcinomas (13.1%), and CNS tumors (11.6%) (Table 1).
Distribution of different pediatric cancer types according to age-group and gender in the Hadhramout region of Yemen.
Frequencies of different hematologic malignancies according to age-group and gender among pediatric patients in the Hadhramout region of Yemen.
In the 0-4 years age-group (n=126), lymphoma ranked first (n=26), followed by leukemia (n=25), renal (n=16) and eye tumors (n=16), CNS tumors (n=13), and sympathetic nervous system (SNS) tumors (n=8) (Table 1). In the 5-9 years age-group (n=143), leukemia ranked first (n=38), followed by lymphoma (n=35). Carcinomas represents the third cancer in this group (n=22), followed by CNS tumors (n=18), soft tissue sarcomas (n=9), bone (n=6), and SNS tumors (n=6). In the 10-14 years age-group (n=137), lymphoma ranked first (n=36), followed by leukemia (n=30), carcinoma (n=25), and CNS tumors (n=16).
The common cancer types among boys (compared with girls) in order of frequency were lymphomas (75.3%), leukemia (52.7%), carcinoma (54%), CNS tumors (54.2%), eye tumors (68.4%), soft tissue sarcomas (45.8%), bone tumors (47.6%), renal tumors (36.4%), SNS tumors (42.9%), and hepatic tumors (6.7%) (Table 1).
Leukemias and lymphomas were the most numerous histiotypes, comprised of 47% of the total number of cancers (Table 2).
All lymphomas were more or less frequent in males than females. Hodgkin’s disease (HD) predominated over non-Hodgkin’s lymphoma (NHL). Both of them are more common in males than females, with a stronger male to female ratio of 5.8:1 in case of HD, and 2.7:1 in case of NHL, Burkit’s lymphoma shows equal gender incidence (Table 2).
Table 3 summarizes the different nervous system malignancies by age-group and gender. Medulloblastoma and gliomas were the most common CNS tumor with equal incidence, followed by astrocytoma, primitive neuroectodermal tumors, and ependymoma.
Frequencies of different nervous system malignancies by age-group and gender among pediatric patients in the Hadhramout region of Yemen.
Table 4 summarizes the different solid tumors by age-group and gender. Rhabdomyosarcoma was the most common soft-tissue sarcomas, other rare tumors in our study were fibrosarcoma, angiomyosarcoma, lymphangiosarcoma. Skin carcinoma was the most common carcinoma, it is more common in the age group of 5-9 years, followed by nasopharyngeal carcinoma. Carcinoma is more common in males than females (Table 4).
Frequencies of different solid tumors by age-group and gender among pediatric patients in the Hadhramout region of Yemen.
Gonadal and germ cell neoplasms all occur in males, there was one case of langerhans cell histiocytosis in male, and other unspecified malignant tumors (6 cases). Further analysis of nervous system tumors, bone tumors, and other solid tumors according to age is presented in Tables 3 & 4.
Comparison of pediatric cancer in Yemen and the SEER database
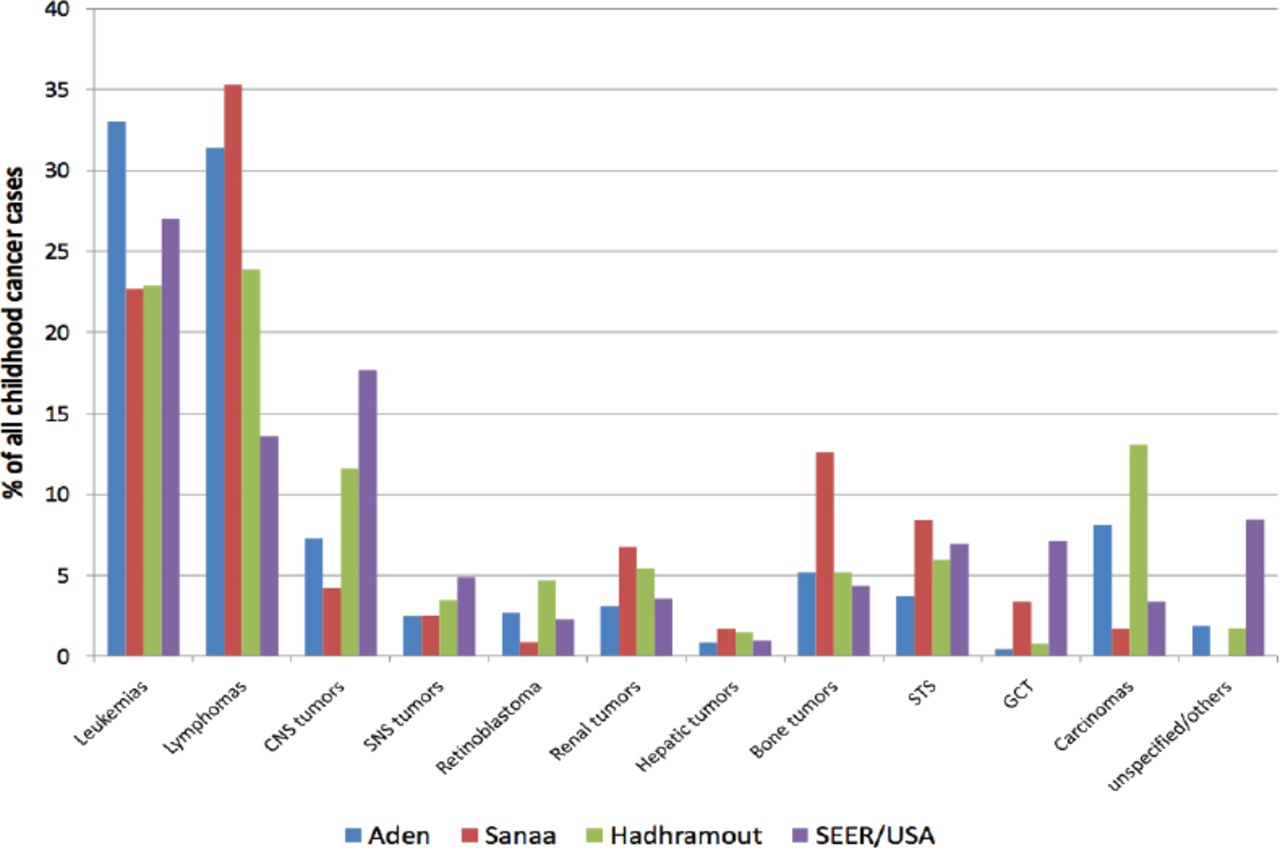
The distribution of different pediatric cancer types in HCR was compared with those reported previously from Aden, Sanaa, and the SEER database (Figure 1). The most common cancer type in Hadhramout (24%) and Sanaa (35%) was lymphomas. There was a higher percentage of retinoblastoma in Hadhramout (4.7%) compared with other reports. The percentage of carcinomas in HCR (13%) was much higher than that reported in Sanaa (1.7%), as well as the SEER report (3.4%).3-5,14

Distribution of pediatric cancer types reported in Aden, Sanaa, Hadhramout, and the Surveillance, Epidemiology, and End Results (SEER) database.
Discussion
A total of 406 childhood cancers of both sexes comprising 8.5% of all malignancies (n=4796) were registered at the HCR from January 2002 through December 2014. This is also comparable with reports from developing countries, where the childhood cancer incidence varies between 4.1-12.6%.3 A study conducted in Saudi Arabia16 reported a childhood cancer accounted for approximately 8% of total cancer cases, which is comparable with our results. A previous study3 from the Yemen was conducted using the data from Aden Cancer Registerfor patients registered from 1997 until 2006, and showed that childhood cancers constitute 12.7% of all malignancies. In this study, the childhood cancer incidence was higher among Yemeni boys than girls, with a male to female ratio of 1.4:1. Similar to other reports from other Arab countries, male predominance was noticed with a male to female ration of 1.4:1.17-20
There was variable age-specific incidence pattern in our study with the predominant age group of 5-9 years (36% of all cases), a finding that is in a accordance with other studies from Yemen.3,5 Also, our study showed that lymphomas are the most common childhood cancers (24%) followed by leukemias (23%), carcinomas (13.1%), and CNS tumors (11.6%). Our results are similar to developing countries especially African countries such as Sudan20 and Nigeria,21,22 and also to a study conducted in Yemen,5 where lymphomas were the most common cancers.23
We showed a relatively high proportion of hematological malignancies (47% of cases). Acute lymphoblastic leukemia has tendency to occur in young children with approximately 70% of cases occurring in children less than 9 years. It also has the preference to occur more in males than females.2-5,23,24 Acute myeloid leukemia occurs more frequently in females than males; this is an uncommon finding, but similar results were also found in another study conducted in Yemen.3 Only one case of chronic juvenile myeloid leukemia was found in our study, which is a rare disease worldwide.2,24
Most cases of lymphoma were reported in late childhood with 73.2% of cases reported in children 5-14 years. A male predominance was observed in all lymphoma subtypes, except for Burkitt’s lymphoma. The higher than expected incidence of lymphoma in our population is similar to other reports from Africa. It is possible that genetic mixing or certain unknown environmental factors contribute to this similarity.22
An important observation in our study was the large number of non specific CNS tumors (38.3%). This may be due to lack of advanced pathologic diagnostic facilities or to the fact that most patients with brain tumors travel abroad for diagnosis and treatment, even before their data is captured in our registry. Neuroblastoma is the most common SNS tumor. As expected, all cases were reported in children <9 years with the majority reported in children <4 years.1,25
Ewing sarcoma was the most common bone tumor with more than half of cases reported in children 10-14 years. This is in contrast to other studies that reported osteosarcoma to be more common,1,3 but it agrees with the pattern of bone tumors in Africa2 especially in Surinam and Nigeria.21 Rhabdomyosarcoma is the most common soft tissue sarcoma with most cases reported in children <9 years, this contrasts with the behavior of rhabdomyosarcoma described in literatures and with similar results found in other studies.3,22
Carcinoma represented 13.1% of cases with the majority of cases (88.7%) reported in children more than 5 years; most cases were reported in males (60%). An unusual finding is the large number of skin cancers representing more than half of all cases of carcinoma (51%) with the majority of these cases occuring in children more than 5 years. This may be explained by the finding of high consanguineous marriages in Shabowa and Hadhramout governarates with relative high incidence of cutaneous precancerous conditions such as xerodermapigmentosum.27,28 Nasopharyngeal carcinoma is the second most common type in children as it represented 11.3% of all carcinomas, a finding that is in line with other reports.29,30 Other rare carcinomas reported were adenocarcinoma, thyroid carcinoma, and adrenocortical carcinoma, with a low incidence similar to reports in the literature.31-33
Nephroblastoma was the most common renal tumor in our study accounts for most cases reported in children <4 years, which is similar to the results found in other studies.34 Primary neoplasms of the liver constitute 0.5-2% of cases in children <15 years.35 In our study, hepatocellular carcinoma is the most common hepatic tumor accounting for two-thirds of hepatic tumors, followed by hepatoblastoma; this differs from other studies in Yemen,3,4 which found that hepatoblastoma was more common than hepatocellular carcinoma. Retinoblastoma is the most common eye tumor accounting for 78.9% of cases, most of them occur in children <4 years, this is similar to results found in other studies.3,36
Study limitations
Absence of specialized diagnostic facilities, and incomplete cancer notification to the registry since many patients with malignancy travel abroad, and scanty available information on cancer in Yemen.
In conclusion, when the distribution of our cases was compared with other reports from Yemen and to the SEER database, interesting differences were identified. Higher numbers of patients with lymphoma and carcinomas were observed, especially in our study. Also, a lower frequency of CNS tumors was also observed. Further studies into the genetic and environmental causes of these differences are warranted.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided
Non-indexed materials
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 31, 2016.
- Accepted February 26, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.