


Abstract
Objectives: To report the ipsilateral lung dosimetry data of breast cancer (BC) patients treated with loco-regional hypofractionated radiotherapy (HFRT).
Methods: Treatment plans of 150 patients treated in the Radiotherapy Unit, King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia between January 2012 and March 2015 by HFRT for BC were retrospectively reviewed. All patients received 42.4 Gy in 16 fractions by tangential and supra-clavicular fields with 6 MV, 18 MV, or mixed energies. Ipsilateral lung dosimetric data V20Gy and mean lung dose (MLD) were recorded. Correlations between lung dose, patient characteristics, and treatment delivery parameters were assessed by a logistic regression test.
Results: The mean ipsilateral lung V20Gy was 24.6% and mean MLD was 11.9 Gy. A weak, but statistically significant correlation was found between lung dose and lung volume (p=0.043). The lung dose was significantly decreasing with patient separation and depth of axillary lymph node (ALN) and supra-claviculary lymph nodes (SCLN) (p<0.0001), and increasing with ALN (p=0.001) and SCLN (p=0.003) dose coverage. Lung dose significantly decreased with beam energy (p<0.0001): mean V20Gy was 27.8%, 25.4% for 6 MV, mixed energy, and 21.2% for 18 MV. The use of a low breast-board angle correlates with low lung dose.
Conclusion: Our data suggest that the use of high energy photon beams and low breast-board angulation can reduce the lung dose.
Adjuvant radiotherapy (RT) after breast conservative surgery is the standard of care for patients with breast carcinomas (BC), and indicated after mastectomy, according to the stage of the disease.1-5 Loco-regional RT to the ipsilateral supra-claviculary (SCLN), axillary lymph nodes (ALN), or internal mammary nodes (IMN) could be added, according to the status of LN involvment. Although the conventional RT course consists of 50 Gy delivered in 25 daily fractions over 5 weeks, evidence from large randomized trials demonstrated that hypofractionated (HF) RT yield to equivalent results in terms of local control, survival, and radiation related toxicity.6-8 Hypofractionated dose regimen of 42.4 Gy in 16 fractions is routinely used at our institution, for various BC presentations. Regional lymph node (LN) irradiation includes: level 2 and 3 of ALN and supra-clavicular LNs. While most of level 1 ALN is irradiated by tangential fields, we assure its optimal dose coverage when more than 50% of lymph nodes are positive, in inadequate ALN dissection, or when there was extra capsular extension. One of the organs-at-risk in breast RT is the ipsilateral lung and established toxicities are radiation-induced pneumonitis and fibrosis.9 To date, there are no clear guidelines or recommendation regarding the acceptable dose limits for the lung. However, a recent meta-analysis showed that the strongest dose-volume-histogram (DVH) parameters associated with ipsilateral lung radiation-induced pneumonitis are the lung volume receiving 20 Gy or more (V20Gy) and mean lung dose (MLD).10 The authors recommended keeping the V20Gy < 24% and MLD <15 Gy without compromising the required dose coverage, and revealed that the use of supra-clavicular, or IMN irradiation fields correlates with an increased risk of pneumonitis.10 The purpose of this retrospective study is to report the ipsilateral lung dosimetry data of our patients treated with breast HF RT, seeking for possible correlations between lung dose, patient characteristics, and treatment delivery parameters.
Methods
One-hundred-fifty patients treated in the Radiotherapy Unit, King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia, between January 2012 and March 2015 for BC after breast conservative surgery, or mastectomy by HFRT were included in this retrospective study. The study was conducted according to the principles of Helsinki Declaration and approved by the institutional Research Ethics Committee. All patients underwent CT-simulation in supine position on an angled board, with both arms placed above their head, which was rotated to the contralateral side (Somatom Sensation CT-scanner, Siemens Medical Systems, Erlangen, Germany). The CT axial images were acquired with 3 mm slice thickness, from the chin to the upper abdomen, including bilateral breasts and lungs. Patients received 42.4 Gy in 16 fractions by tangential and supra-clavicular fields. Lymph nodes were contoured according to the Radiation Therapy Oncology Group (RTOG) consensus definitions.11 Lungs were delineated using threshold auto-contouring and manually edited to smooth the visible lung borders. Dose calculation was performed by eclipse treatment planning system, versions 10 and 11, using analytical anisotropic algorithm (AAA) and inhomogeneity correction (Varian Medical Systems, Palo Alto, CA, USA). All treatment plans were mono-isocentric, used field-in-field forward planning optimization, and 6 MV, 18 MV, or mixed beam energies. Treatment planning aimed at adequate dose coverage of breast, or chest wall and LNs, according to individual clinical condition. Dose homogeneity was achieved according to the International Commission on Radiation Units and Measurement (ICRU 50/62) recommendations.12,13 All treatment plans were retrospectively reviewed and ipsilateral lung dosimetric data, such as percentage of lung volume receiving 20 Gy or more (V20Gy), and mean lung dose were recorded.
Correlations between lung dose, patient characteristics (lung volume, chest wall separation, depth and coverage of ALN and SCLN), and treatment delivery parameters (beam energy, breast board angle, posterior supra-clavicular field) were assessed by a logistic regression test and a p value of <0.05 was considered significant. Statistical analysis was performed using IBM SPSS Statistics software version 20 (IBM Corporation, NY, USA).
Results
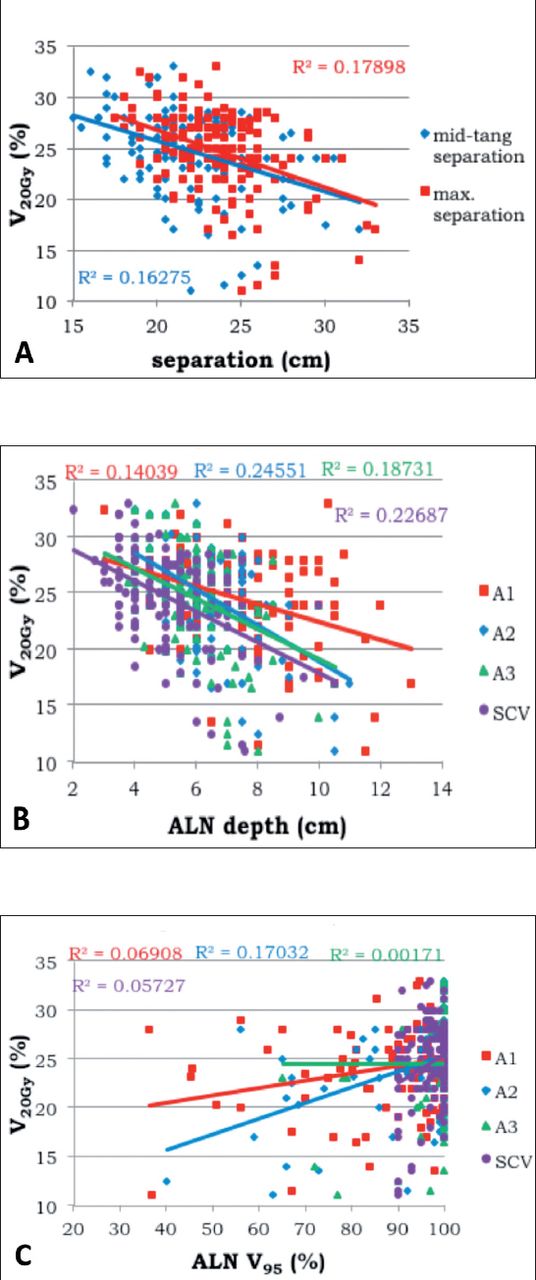
We identified 65 (43%) left-sided and 85 (57%) right-sided BC patients; 46 (30%) had conservative surgery and 104 (70%) mastectomy. A weak, but significant correlation was found between V20Gy and lung volume (R2 = 0.027, p=0.043), not between MLD and lung volume (R2 = 0.013, p=0.171). However, on differential analysis, V20Gy appeared to fairly and significantly associate with the lung volume for left-sided cases (R2 = 0.113, p=0.006), but not for the right-sided ones (R2 = 0.14, p=0.283). Ipsilateral lung dosimetric data (n=150) are summarized in Table 1. The lung dose assessed by V20Gy was decreasing with patient separation and depth of ALN and SCLN (p<0.0001). Multivariate analysis showed that the beam energy is the strongest factor affecting V20Gy (p<0.0001), when compared to patient separation (p=0.169) and depth of ALN (p=0.073) and SCLN (p=0.001). Lung V20Gy was significantly increasing with ALN (p=0.001) and SCLN (p=0.003) coverage were measured by the percentage volume of ALN and SCLN covered by at least 95% of the prescribed dose (V95%). The addition of a posterior axillary boost field had no effect on the lung dose. The use of a low breast board angle seems to decrease the lung dose. Due to the small number of patients treated on breast board with 10 and 20 degree angles, analysis of the correlation between ipsilateral lung dose and board angle was not performed. Figure 1 summarizes the correlation between ipsilateral lung V20Gy and patient separation. Figure 2 shows the correlation between ipsilateral lung V20Gy and MLD, and beam energy.
Ipsilateral lung dosimetric data (n=150).

Correlation between ipsilateral lung volume receiving A) 20 Gy or more (V20Gy) and patient separation, B) depth of lymph nodes (LN), and C) coverage of LN. R-squared values are displayed on the chart.

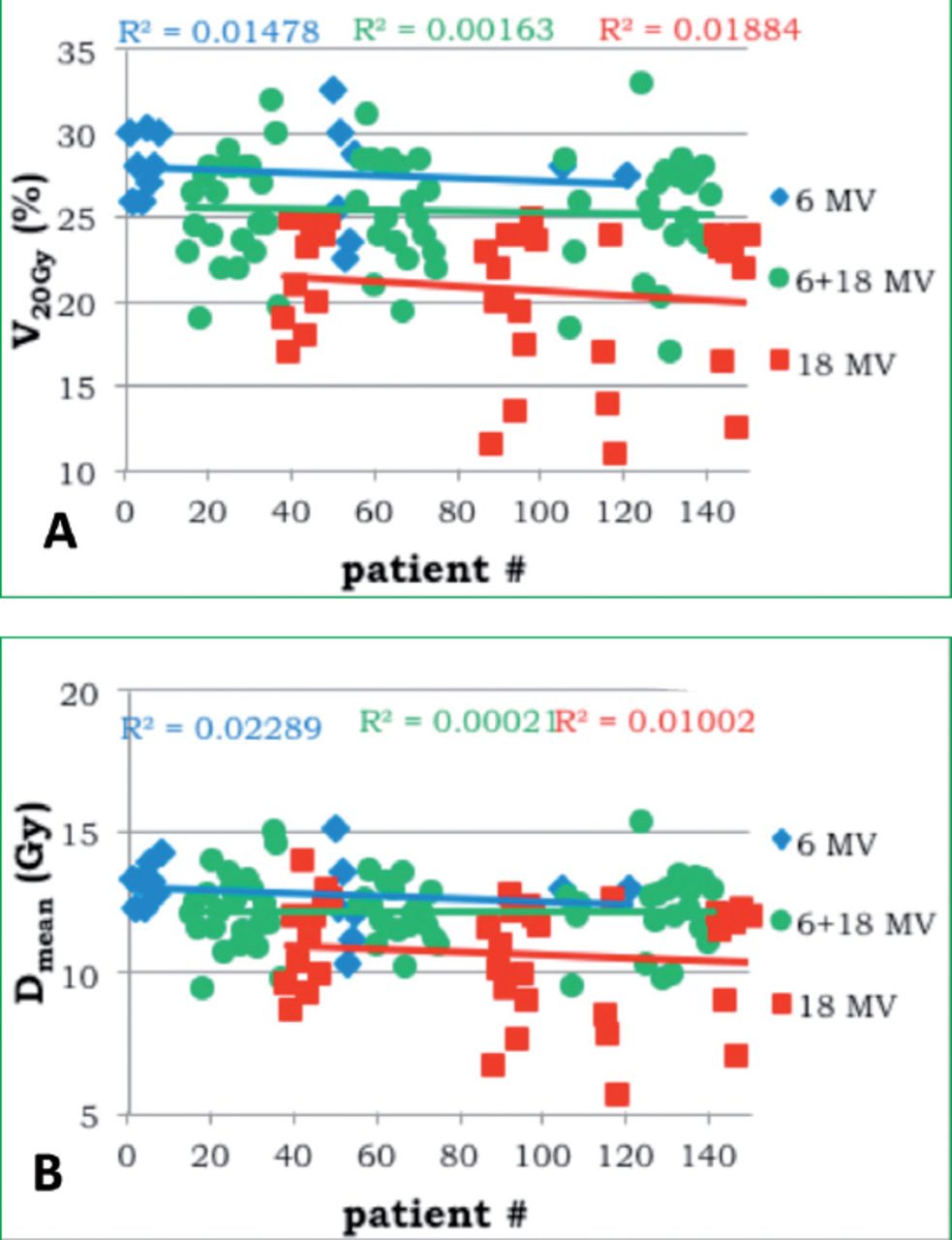
Correlation between beam energy and the ipsilateral lung volume receiving A) 20 Gy or more (V20Gy) and B) mean lung dose (MLD).
Discussion
The recent advances in technology and knowledge in radiotherapy had driven attempts of minimizing toxicity. In the particular case of breast RT, the ipsilateral lung is one of the main organ-at-risks, as its irradiation can induce pneumonitis, or fibrosis.9,10 The literature on lung toxicity in breast irradiation is very heterogeneous: different simulation techniques (conventional fluoroscopy versus CT), different treatment planning systems (2-dimensional conformal radiotherapy versus 3-dimensional conformal radiotherapy), different sites treated (chest wall/breast ± ALN/SCN/IMN) were reported. Gokula et al10 demonstrated in a recent meta-analysis that the strongest DVH parameters associated with ipsilateral lung radiation-induced pneumonitis were V20Gy and MLD. They recommended to keep the V20Gy < 24% and MLD < 15 Gy without compromising the required dose coverage, and to consider other RT techniques when V20Gy >30%, or MLD >15 Gy. We also emphasized that the use of SCN, or IMN irradiation fields correlates with an increased incidence of pneumonitis. In our institution, HF dose regimen of 42.4 Gy in 16 fractions was implemented in postoperative breast RT in January 2010 and for whole breast, or chest wall, with or without supra-clavicular field. Providing the relatively long life expectation of BC patients treated by the current therapies and the potential impact of lung damage on their quality of life, it important to analyze the dose received by lung and its possible correlations with patient’s characteristics and treatment delivery parameters. Our data showed that the recommendations of Gokula et al10 for ipsilateral lung dose can be achieved even if a supra-clavicular field is used: we found mean values of 24.6% for V20Gy and 11.9 Gy for MLD. The contribution to V20Gy from tangential was almost double that of supra-clavicular fields (16% versus 8.6%). Adding a posterior axillary boost field did not significantly increased the lung dose (p=0.476). Contouring the regional LNs makes the planner aware in evaluating the need for a posterior axillary boost field, and helps in applying different weights of anterior supra-clavicular and posterior axillary boost fields during the plan optimization process, aiming to achieve adequate coverage for ALN and SCN without unnecessarily irradiate the lung. Using a mono-isocentric technique and field-in-field optimization is a common practice in breast RT, widely described in the literature.14-18 A single iso-center has the advantage of a simple and reproducible positioning of the patient on linac couch and is reducing the workload of radiation therapists. Field-in-field technique is a very simplified form of intensity modulated radiation therapy (IMRT), which uses few sub-fields whose shape and weight are adjusted by the planner in order to achieve a homogenous dose distribution. Yet, the plan optimization by field-in-field technique may require the use of high energy photons to achieve an adequate homogeneity of the dose, especially if large volumes are to be irradiated.17,18 Our data showed a weak, but significant correlation between V20Gy and lung volume (p=0.043), not between MLD and lung volume (p=0.171). While these results are predictable for MLD, the correlation of V20Gy with lung volume was expected to be relevant, as V20Gy is defined as percentage of lung volume receiving 20 Gy or more. The volume of the left lung is usually smaller than the right one, we further proceeded to differential analysis, and found that V20Gy significantly associated with the lung volume for left-sided cases (p=0.006), but not for the right-sided ones (p=0.283). As 43% of our patients were left-sided and 57% were right-sided, the overall effect of the relation between V20Gy and lung volume appeared lessened. Twenty-four (16%) of our patients were treated with 6 MV, 81 (54%) with mixed energy (6 and 18 MV), and 45 (30%) with 18 MV. Lung dose significantly decreased with beam energy (p<0.0001): mean V20Gy was 27.8% for 6 MV, 25.4% for mixed energy, and 21.2% for 18 MV. These results are not surprising. The increased lateral range of secondary electrons in low density tissue, such as lung, when using photon energies higher than 10 MV generates a build-up region in lung tumors and increases the beam penumbra, resulting in reduced dose to the periphery of the target near the beam edge. This is a well-known phenomenon, which has been widely assessed in phantom measurement and Monte Carlo calculations.19-25 DesRosiers et al19 compared 6 MV to 15 MV photons in a Monte Carlo simulation for different beam arrangements in low density media and demonstrated that for every beam arrangement 15 MV photons delivered 5-10% lower dose than 6 MV photons. In a similar study, comparing 6 MV to 18 MV for IMRT treatment for lung cancer, Madani et al24 found significant difference in target coverage between the 2 energies, and highlighted the need for highly accurate dose calculation algorithms for heterogeneous media. The performance of AAA algorithm used in our study was evaluated against Monte Carlo calculation in low density tissue by several investigators, and found to be an adequate alternative.25-31 Based on the research evidence, there is a preference of low photon energies for the radiotherapy of lung cancer, that are even required in lung cancer radiation Therapy Oncology Group (RTOG) protocols and American Association of Physicists in Medicine (AAPM) guidelines.32-35 While the lung dose sparing by high energy photons is detrimental in lung radiotherapy, it appears to be a significant advantage in breast irradiation, where the lung is an organ-at-risk. Nevertheless, the choice of appropriate beam energy in breast RT planning is determined by patient separation for tangential, and depth of LNs for supra-clavicular fields. This explains the results of our study: the lung dose was decreasing with patient separation and depth of ALN and SCLN (p<0.0001), as a large separation and deep LNs required the use of high energy in order to achieve acceptable dose coverage and homogeneity. However, multivariate analysis indicated the beam energy being the strongest factor affecting V20Gy (p<0.0001), when compared to patient separation (p=0.169), depth of ALN (p=0.073), and SCLN (p=0.001). High energy photons will generate a characteristic skin-sparing effect, under-dosing the subcutaneous tissue, which is a possible area of clinical failure in breast RT. The effect can be easily outweighed by using a bolus.36,37
Treatment planning takes into account the individual clinical condition of the patient, ensuring adequate dose coverage to regional LNs that may not have been properly addressed surgically, or are known to be involved. The different range of dose coverage for different nodal regions are shown in Figure 1C. The aimed dose coverage of LNs had a significant effect on the lung dose: V20Gy was increasing with ALN (p=0.001) and SCLN (p=0.003) coverage assessed by V95%. For patients receiving breast radiotherapy, the conventional set-up is supine position, on an angulated breast board. The breast board angle is chosen to align patient’s sternum with the horizontal plane, thus, eliminating the need for collimator angulation on tangential fields and reducing the irradiated lung volume in cranio-caudal direction. In our practice, the 15 degrees breast board angulation is usually selected, but in certain circumstances different angles might be used. While lower angle, such as 10 degrees were applied for large, or pendulous breast and obese patients, aiming to decrease the inframammary fold, larger angle of 20 degrees is occasionally preferred by some patients, for better comfort. The board angulation causes an increased lung volume exposed to the supra-clavicular field. The literature is lacking studies assessing the effect of breast board angulations on plan dosimetry. However, Yang et al38 demonstrated that a 90 degrees rotation of the couch along with a gantry tilt for supra-clavicular field, can outweigh the effect of the board angle, and significantly reduce the lung volume irradiated by the supra-clavicular field from 14.9-5.3%.38 Nevertheless, the technique they proposed does not allow the shield of the spinal cord and a compromise between cord avoidance and lung dose reduction is needed. Our study shows similar results: a trend between lung dose and breast board angle was noticed, favoring a low board angle (mean V20Gy was 22.9% for 10 degrees, 24.5% for 15 degrees and 25.2% for 20 degrees). As the contribution to lung dose from supra-clavicular field is approximately one third, the benefit appears low. Only 9 (6%) patients were treated on 10 and 20 degrees board, a statistical evaluation was not performed.
Study limitations
Selection of a hypofractionated dose regimen for breast cancer radiotherapy. Obviously, if conventional dose fractionation is to be considered, our results will not be accurate and further research work will be needed to assess the lung dose. Our findings concerning the correlation trends between lung dose, patient characteristics, and treatment delivery parameters stil valid.
In conclusion, we are reporting acceptable ipsilateral lung doses in HFBR, even if supra-clavicular fields are required. Our data suggest that the use of high beam energy significantly reduces the lung dose. Low breast board angulation appears to correlate with a decreased lung dose, and further investigation of this finding is needed.
Saudi Medical Journal Online features
*Instructions to Authors
*Uniform Requirements
*STARD
*Free access to the Journal’s Current issue
*Future Contents
*Advertising and Subscription Information
All Subscribers have access to full text articles in HTML and
PDF format. Abstracts and Editorials are available to all
Online Guests free of charge.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 1, 2015.
- Accepted April 27, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.