


Abstract
Objectives: To characterize overlap syndrome, investigate its impact on airflow limitation and blood oxygen condition, and detect the risk factors that affect its airway resistance.
Methods: We reviewed retrospectively the clinical data of 158 patients with overlap syndrome (OS), chronic obstructive pulmonary disease (COPD), and obstructive sleep apnea (OSA), treated in the Critical Care Medicine Department of the People’s Hospital of Liaocheng, Liaocheng, China from May 2014 to March 2015. The lowest and average oxyhemoglobin saturation were measured using polysomnography. The pulmonary functions were tested using the cardiopulmonary measuring instruments, and the viscous resistance at oscillation frequencies of 5, 10, 15, 20 Hz was measured using the impulse oscillation system for all the patients.
Results: The values of forced expiratory volume (FEV)1/FVC, FEV1% predicted, and the lowest SaO2 in the OS group were significantly lower than those in the OSA (p<0.01, p<0.01, p=0.01), or the COPD group (p=0.03, p=0.02, p=0.03), but the value of viscous resistance at 5 Hz was significantly higher than that in the 2 groups (p<0.01). Old age, body mass index, and smoking history were significantly correlated with the viscous resistance in OS patients, at an oscillation frequency of 5Hz (p=0.03, p=0.04).
Conclusion: The OS patients present with higher viscous resistance and more severe oxygen deficit, when compared with OSA and COPD patients, and weight decrease and smoking cessation are necessary for these patients.
Both chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) are the most common chronic respiratory disorders. COPD accounts for approximately 4% of all American deaths and is the third common cause of death in the US.1 In 1985, Flenley defined the coexistence of the 2 conditions in a single patient as the “overlap syndrome (OS)”.2 It was reported that the prevalence of OS in patients over 40 years was 1%.3 In addition, the patients had been surmised to have a worse prognosis than those with only one of these diseases.4 OS is associated with an increased risk of nocturnal oxygen desaturation and may develop complete respiratory failure with increased carbon dioxide retention, more frequently,5 as a result, OS may result in a higher mortality rate compared to COPD. However, despite a high prevalence of COPD in the population, the clinical features of patients with OS have not been well described up to now. As OS is the coexistence of COPD and OSA, it may result in higher airway resistance and more severe hypoxemia than either of the 2 conditions, but few studies have been carried out to confirm the issues. We believe that a better understanding of the clinical features as well as the related risk factors of OS may facilitate physicians to identify treatment strategies. Therefore, we reviewed the clinical data of 158 patients with OS, COPD, or OSA. The aim of our study was to Characterize OS and investigate its impact on airflow limitation and the blood oxygen condition and to detect the risk factors that affect the airway resistance of OS, to facilitate identifying treatment strategies.
Methods
Our study subjects included patients diagnosed with OS, COPD, or OSA and treated in the Department of Critical Care Medicine of the People’s Hospital of Liaocheng from May 2014 through March 2015. The patients were divided into 3 groups of OS, COPD, or OSA according to the diagnosis. In the study, the diagnosis of COPD was defined as subjects having an FEV1/FVC ratio of <0.7 without any history of self-reported wheezing.6 OSA was defined by a respiratory disturbance index [RDI] score of ≥5, with or without symptoms.7 Those with the coexistence of COPD and OSA were diagnosed as “overlap syndrome (OS)”. The patients with the following conditions were excluded from the current study: 1) abnormal lung parenchymal lesions including interstitial pneumonia; 2) congestive heart failure; 3) lung cancer; 4) other obstructive lung diseases such as obliterative bronchiolitis or diffuse panbronchiolitis; 5) infectious disease including lung tuberculosis, and 6) cognitive disorders.8 This study was approved by the Ethical Committee of our hospital and was performed according to the principles of the Helsinki Declaration. All the included patients gave their informed consent. To find previous related clinical studies, we searched the literature on MEDLINE from July 1985 through June 2015. The search was carried out by using the text words “chronic obstructive pulmonary disease,” “obstructive sleep apnea,” “overlap syndrome,” and “chronic respiratory disorders,” by 2 physicians in our department.
Procedure
The clinical data of all the included cases, including age, gender, smoking history, and BMI were recorded. The lowest and average oxyhemoglobin saturation, apnea-hypopnea index (AHI), oxygen desaturation index (ODI), and total sleep time with SaO2 under 90% (T90) were measured using polysomnography. The pulmonary function tests, including the forced vital capacity (FVC), forced expiration volume of one second (FEV1), and the percentage of forced expiration volume of one second from the predicted value (FEV1% pred) were measured using the cardiopulmonary measuring instruments.9 In addition, the pulmonary function was tested with the impulse oscillation system to detect the viscous resistance of all patients at oscillation frequencies of 5, 10, 15, and 20 Hz.
Statistical analysis
it was carried out using SPSS20.0 (Chicago, IL, USA). The measurement data, including age, BMI, smoking history, FEV1/FVC, FEV1% pred, mean SaO2, lowest SaO2, AHI, ODI, T90, and the viscous resistance at different oscillation frequencies were given as mean ± standard deviation, and the comparison was performed using the analysis of variance (ANOVA). The enumeration data were compared using the Chi-Square test. The correlation between different variables was studied using the multivariable linear regression analysis. A p-value less than 0.05 was considered to indicate the statistical significance.
Results
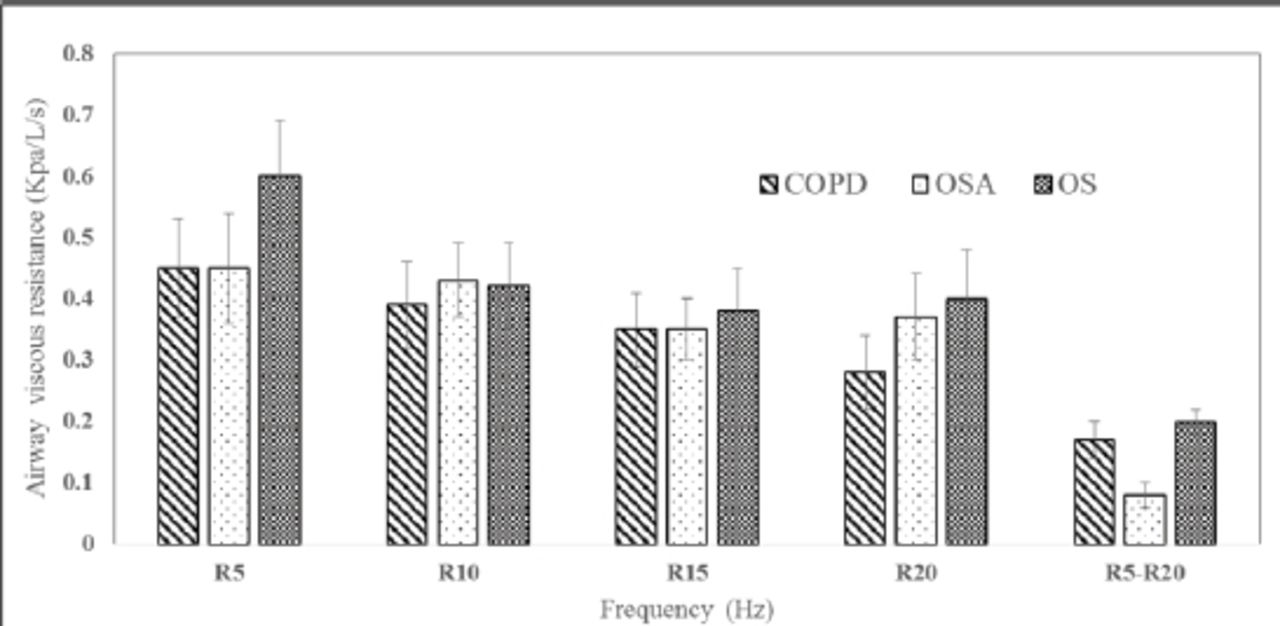
In the current study, a total of 158 patients were included and 56 patients were allocated to the OS, 61 with COPD, and 41 with OSA groups. The basic clinical data, including age, gender, smoking history, and BMI is listed in Table 1. There was no significant difference in gender between the 3 groups (p=0.743), but the patients in the OS group were significantly elder than those in the OSA group (p=0.01), and presented with a higher value of BMI than those in the COPD group (p=0.02). They had a longer smoking history than those in the OSA group (p<0.01). In addition, the values of FEV1/FVC, FEV1% pred, and the lowest SaO2 in the OS group were significantly lower than those in the OSA (p<0.01, p<0.01, p=0.01), or COPD groups (p=0.03, p=0.02, p=0.03), but T90 was significantly higher in the OS group than those in the 2 groups (p<0.01). The values of AHI (p<0.01) and ODI (p<0.01) in the OS and OSA group were significantly higher than those in the COPD group. However, in terms of the values of the mean SaO2, no significant difference was found between the COPD and OSA groups (p=0.06), but the values in the OS group was significantly lower than those in the OSA group (p=0.04) (Table 1). The values of the viscous resistance of all patients at oscillation frequencies of 5, 10, 15, and 20 Hz are listed in Figure 1. The values of viscous resistance at 5 Hz were significantly higher in the OS group than those in the OSA (p<0.01) or COPD groups (p<0.01), and the values at 20 Hz were higher than those in the COPD group (p=0.01), but there was no significant difference between the OS and OSA groups (p=0.08). In terms of the values of R5-R20, a significant difference was detected between the OS and OSA groups (p<0.01), but there was no significant difference between the OS and COPD groups (p=0.09) (Figure 1).
General characteristics of patients in the 3 groups.

The comparison of airway viscous resistance in the group of Chronic obstructive pulmonary disease (COPD), Obstructive sleep apnea (OSA), and Overlap syndrome (OS).
In the multi-variable linear regression analysis, we found that age was significantly correlated with the viscous resistance of OS patients at oscillation frequencies of 5 (p=0.03), 10 (p=0.02), 15 (p=0.03), and 20 (p=0.01) Hz. In addition, the BMI and smoking history were closely correlated with the viscous resistance of OS patients at oscillation frequencies of 5 Hz (p=0.03 and 0.04.). Also, a negative correlation was found between the value of viscous resistance and FEV1/FVC (p=0.01), FEV1% pred (p=0.02), and the lowest SaO2 (p=0.02), in the OS group.
Discussion
In the current study, the values of FEV1/FVC, FEV1% pred, and the lowest SaO2 in the OS group were significantly lower than those in the OSA or COPD groups. However, no significant difference was found in the mean SaO2 between the COPD and OS groups. This may be attributed to the small sample size. Some studies advocate that OS, in which hypoxemia, hypercapnia, and pulmonary hypertension can be observed, has an increased risk of developing hypercapnic respiratory failure and pulmonary hypertension, when compared with patients having OSA or COPD alone.10 Our outcome indicates a similar viewpoint as that in the above-mentioned literature. In addition, we found that the value of viscous resistance at 5 Hz was significantly higher in the OS group than those in the OSA or COPD groups, and at 20 Hz it was also higher than that in the COPD group. Significant difference in R5-R20 was detected between the OS and OSA groups. In terms of airway viscous resistance, OS patients presented with higher values in most of the conditions, demonstrating that the airway obstruction in OS was significantly more severe than those in OSA or COPD. Both COPD and OSA are characterized by local and systemic inflammations,11 indicating the important role of inflammation in the development of airway obstruction in OS patients. Some studies have confirmed an increase of local biomarkers of inflammations, polymorphonuclear leukocytes in the nasal mucosa12 and the neutrophilic percentage in induced sputum in patients with OSA.11 In addition, airway remodeling and parenchymal destruction resulted from airway inflammation.13 Moreover, the important role for CD103 in the control of airway inflammation14 was also confirmed. At the same time, some other factors could also affect airway obstruction. The soft tissues at the base of the tongue and throat were very easily relax in OS patients when they were sleeping, which could block the respiratory tract, and increase the airway obstruction.15 We also found a negative correlation between viscous resistance and FEV1/FVC, FEV1% pred, and the lowest SaO2 in OS patients. This demonstrates that airway obstruction aggravates the difficulty in breathing and subsequently leads to hypoxia. Moreover, in the current study, multivariable linear regression analysis has been carried out to determine the factors that may affect the viscous resistance of airways in OS patients and we have found that old age, BMI, as well as smoking history are significantly correlated with the viscous resistance. Smoking, which may result in a large airway resistance, inflammation, and edema, is a primary factor in the occurrence of COPD. Smoking cessation is regarded as the only strategy that has shown a lasting reduction in the decline of lung function in patients with COPD.16 In addition, obesity can disturb respiratory system mechanics adversely, in isolation or in association with upper airway pathology.17 Subsequently, weight decrease and smoking cessation are necessary for OS patients.
In conclusion, we have found in the current study that OS patients present with higher viscous resistance and severe oxygen deficit when compared to OSA and COPD patients, and weight decrease and smoking cessation are necessary for these patients. However, our study has its limitation. The sample size is relatively small because this study has been carried out at a single institute. It is difficult to conduct a large-scale clinical study. Moreover, some comparisons between variables may have no significance as a result of the small sample size. A large-scale clinical trial may be better for clarifying the issues. Subsequently, more studies need be performed in the future.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received November 29, 2015.
- Accepted April 20, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.