


Abstract
Objectives: To assess patients’ perceptions of the communication skills of family medicine residents.
Methods: This is a cross-sectional study. Data were collected from patients, seeing 23 residents from 4 family medicine residency programs in Riyadh, Kingdom of Saudi Arabia namely, King Khalid University Hospital, Riyadh Military Hospital, Security Forces Hospital, and King Abdul-Aziz Medical City. The translated version of the Communication Assessment Tool (CAT) was used. Data were collected during January and February 2013.
Results: A total of 350 patients completed the CAT, with an 87.5% response rate. Patients rated each resident differently, but the mean percentage of items, which residents rated as excellent was 71%. In general, male residents were rated higher 72.8 ± 27.2 than female residents 67.8 ± 32.2 with a significant difference; (p<0.005). Also, significant differences were found based on the gender of the residents, when each item of the CAT was compared. Comparing training centers, there were no significant differences found in the overall percentage of items rated as excellent or among items of the CAT.
Conclusion: The study identified areas of strength and weaknesses that need to be addressed to improve communication skills of physicians.
Communication skills are an essential component of physicians’ patient management skills and overall competence. It improves the physician-patient relationship and health outcomes for patients, such as improved compliance, satisfaction with care, and benefits to their physical and psychological health. It has an impact on patient health promotion and health education, especially in primary care practice where they get first contact with the doctors.1 Many studies locally and internationally, have shown that patient satisfaction is strongly affected by doctors’ communication skills.2,3 In order to change doctors’ behavior in communication skills, many programs introduced courses for their students and residents. Experience alone can be a poor teacher when it comes to developing communication skills. There are different methods to assess the communication skills among doctors. These include behavioral checklist for direct or video observation, objective-structured clinical examinations (OSCE), and patient satisfaction surveys. The patient’s feedback is of vital importance, when evaluating physician interpersonal and communication skills, and should be considered in all evaluation systems. However, many studies tend to mix treatment satisfaction items with communication skill items, combine multiple communication skill elements into single items, and/or ask patients to rate their satisfaction over a period.4,5 Such concerns often make it difficult to use these tools to provide concrete feedback that could facilitate physician learning and possible behavior change.6 The Communication Assessment Tool (CAT) was developed to assess patients’ perceptions of physician interpersonal and communication skills, while addressing the previously noted limitations of other patient satisfaction tools. Patients are asked to reflect only on the encounter that they just had with the physician, and the CAT items focus on essential communication skill elements. The objective of this study was to use patient perceptions to assess communication skills of the residents in family medicine programs in Riyadh city, Kingdom of Saudi Arabia (KSA) and hence to use the results to improve communication skills among residents. In order to achieve that, the investigators studied various aspects from patient feedback on residents’ communication skills and compared the differences between residents based on their gender and training center.
Methods
This cross sectional study employed the questionnaire CAT, developed to assess patients’ perceptions of the interpersonal and communication skills of physicians. We followed the WHO criteria for translating CAT into Arabic. It was piloted and found to be suitable for our patients. The CAT is a 14-item survey that is easily administered in a paper-and-pencil format. The CAT asks the patients to rate different areas of the communication and interpersonal skills of the physician using a 5-point rating scale (1=poor, 2=fair, 3=good, 4=very good, 5=excellent). Scoring the CAT based on the proportion of items rated as excellent has been found more meaningful than summarizing the scores using other means.5 Data were collected during January and February 2013. A research proposal was reviewed and approved by the Institutional Review Board. Setting description. The Saudi Board of Family Medicine (SBFM) has 4 recognized program centers in Riyadh, KSA. These are King Khalid University Hospital (KKUH), Riyadh Military Hospital (RMH), Security Forces Hospital (SFH), and King Abdulaziz Medical City (KAMC, or National Guard hospital). The programs entail a 4-year residency and represent urban practice settings. All (23 residents) final year residents (R4) in family medicine programs in Riyadh region agreed to participate in the study. Residents who are in a family medicine program during their final year are working in primary care clinics after they rotated in different specialties for first 3 years. The study aimed to investigate family medicine residents during their rotation in family medicine setting. Residents from all years of training are usually rotating in other disciplines of different setting to family practice. First, data were collected for each resident and coded regarding their age, gender, level of training, training center, and the average number of patient seen per session (Table 1). Residents and patient’s participation were voluntary and all data were kept anonymous and confidential. Selection and description of patients. Patients attending clinics of family medicine residency training centers completed a self-administered, paper-and-pencil version of the CAT. It takes less than 5 minutes to fill out the form. Inclusion criteria for the patients included: 1) any patient who came for a follow-up or new patients (male or female), and 2) the first 5 patients in the morning and first 3 patients in the afternoon. We excluded patients who could not communicate due to deafness or other disability. At the end of their appointments, the patients were given the Arabic version of the CAT by support staff. Illiterate patients were interviewed, and if the patient was a child, the child’s parents were asked to fill the form. We collected 15-20 responses for each resident. The patients returned the completed CAT to a secure location at the head nurse office, and residents did not have access to the surveys at the time of completion. Outcome measures and analysis. The percentage of items scored as excellent was calculated as the percentage of items with a score of 5 (excellent) out of the total number of items answered. The overall mean score and overall percentage of excellent scores were summarized across surveys and stratified by gender of the resident and by training center. Chi-square tests were used to compare the groups. Statistical significance was defined as p-value less than 0.05. We used the Statistical Package for the Social Sciences software version 17 (SPSS Inc., Chicago, ILL, USA) for data entry and analysis.7
Demographic characteristics of the patients (n=350)
Results
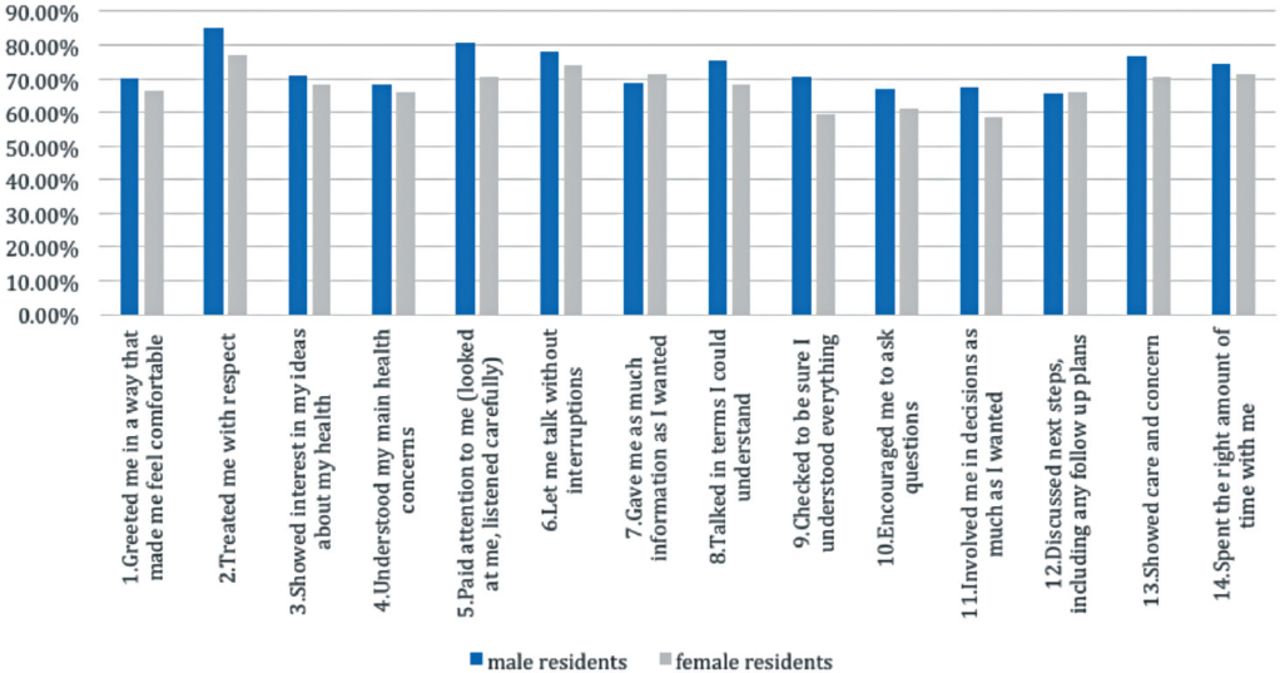
Four hundred questionnaires were distributed; only 350 patients completed the questionnaire over a period of 4 weeks with response rate of 87.5%. Almost all patients were Saudis. The overall mean rating score on the CAT was 4.597 (standard deviation [SD] ± 0.40) and the overall mean percent for “excellent” was 71% (SD±29) (Table 1). The 3 items that were rated most frequently as excellent were “Treated me with respect” (82.3%), “Paid attention to me (looked at me, listened carefully)” (77.1%), and “Let me talk without interruptions” (76.6%). On the other hand, the 3 items rated least frequently as excellent were, “Encouraged me to ask questions” (64.9%), “Involved me in decisions as much as I wanted” {64.3%), and “Discussed next steps, including any follow up plans” (65.7%) (Table 2). Differences by gender of the resident. There were 227 surveys collected from patients seen by male residents and 123 surveys collected from patients seen by female residents. The overall percentage (mean ± SD) of items rated as excellent for female residents was (67.8 ± 32.2) and male residents (72.8 ± 27.2) with a significant difference p<0.005. There were also significant differences between the 2 groups by comparing individual CAT items (Figure 1). Item 5 “Paid attention to me (looked at me, listened carefully)” (p=0.036), and item 9 “Checked to be sure I understood everything”(p=0.035), showed significant differences (Figure 1). Differences by training center. The overall rating of the residents in the National Guard hospital (72.1%) was higher than that of the other programs (70.5%). However, there were no statistically significant differences found in the overall percentage of items rated as excellent (70.5 ± 29.5) versus (KAMC) (72.1 ± 27.9), p=0.241.
Overall percentage (%) of excellent ratings and means for individual communication assessment tool (CAT) items.
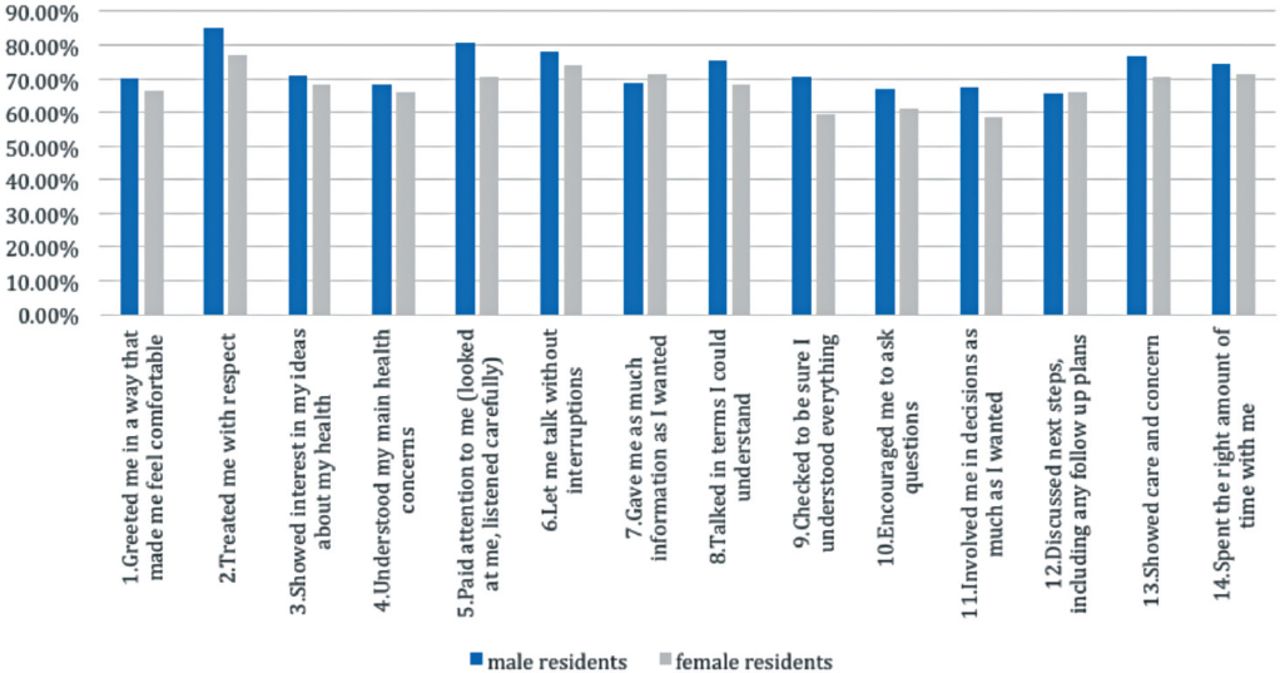
Mean percentage of excellent rate based on gender of the residents.
Discussion
Gathering enough surveys to be able to generalize the finding was a challenge. Based on the Rasch generalizability theory,8 “12-30 ratings per examinee are required when seeking a reliability of 0.96 for data collected on a 5-point scale”. There was a different number of data collected for each resident due to differences in the number of patients seen per resident, but we maintained a minimum of 12 questionnaires per resident. In general, patient rating was high, with the lowest mean ratings on items was(4.5) on a 5-point scale. This might be correlated with what was seen on patient satisfaction surveys, which shows a relatively high score for doctors’ communication skills.9,10 In addition, R4 residents are expected to receive courses during their training, which could explain why most of the residents get a high mean rating. We could not find a similar study carried out in Saudi Arabia to compare our findings with. However, there are some similarities with the 2 studies carried out previously in USA.5,6 The comparisons were made among residents from different training centers with different facilities and family practice setting. Furthermore, the finding was compared with the international literature. It was found that the items rated the highest, were item 2 “Treated me with respect” and item 5 “Paid attention to me (looked at me, listened carefully)”, which is similar to our findings. For most patients, this encounter was their first contact with their resident. This difference can be explained by the lack of follow-up system with the same physician in primary health care. Patients who had seen their resident before, either once or more than once, gave a higher percentage of excellent rating compared with those who had never seen the resident before. However, comparing the 2 groups shows no statistical difference. In our study, there was significant gender differences. Usually both male and female residents see almost the same number of patients. But the gender differences may be due to that female patients have more complaints and take more time. Just by mere speculation this may affect patient satisfaction adversely.
There is some evidence that attitudes toward communication skills training may also be associated with demographic variables, such as gender.11 While few studies have explored the relationship between gender and perceptions of doctors’ communication skills, some small gender differences can be expected. A recent meta-analysis indicated that female physicians are more likely to exhibit patient-centered communication behaviors, such as collaborative and empathic communication, and give psychosocial information.12 Other researchers have found that male medical students are slower at learning communication skills than their female counterparts.13 The differences found between male and female residents need to be interpreted with caution because fewer surveys were completed on females than on males. It seems that the residents’ “training center” did not appear to make a substantial difference on patient perception of overall communication skills as rated using the CAT. There were no significant differences based on the overall percentage of items rated as excellent. While participating programs represented all training centers in the Riyadh and a diversity of settings and populations served, they do not represent the scope of family medicine residency programs across the kingdom. Other difficulties faced during this study were shortage of time and commuting among training centers.
In conclusion, residents in this study have shown good communication skills. The present study also identified strengths and weaknesses that may need to be addressed to help residents in the training program. A systematic feedback to each resident can increase the awareness of patients’ perceptions regarding their communication skills. Items that had the lowest score are signaling the opportunity to be emphasized during supervised consultations and group training for example, during the half day release course. Furthermore, repeating the study at the end of the training program and after a period of say one year may show the trend of improvement or otherwise.
Acknowledgment
The authors would like to acknowledge the cooperation of Dr. Gregory Makoul, PhD, for his permission to use CAT. Authors would also like to express their thanks to the residents and patients who took part in the study.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study (Research project No. E-12-820) was approved and supported by the College of Medicine Research Center and the Chair of Health Education and Health Promotion, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
- Received December 28, 2015.
- Accepted March 27, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.