


Abstract
Aneurysmal bone cyst (ABC) is an expanding osteolytic lesion. ABC represents 1% of all primary benign bone tumors, whereby 4-12% occur in the pelvis. The etiology of this disease remains vague. Aneurysmal bone cyst can exist either as primary bone lesion (70%) or as secondary lesion arising from another bone disorder (30%). Moreover, pelvic ABCs are characterized by their large size and high vascularity. We present a rare pediatric case with ABC involving the ischial region. A 5-year-old girl presented with left pelvic pain and limping for the past 6 months. Initial imaging showed an expansile lesion in the left ischium, and computed tomography guided biopsy showed giant cells in histopathology study with no evidence of metastasis. The patient underwent intraoperative frozen section followed by extensive intra-lesional bone excision. Bone curettage was pursued along with bone grafting. The case was successfully managed without postoperative complications after the 6-month follow-up period.
In 1893, Van Arsdale described aneurysmal bone cyst (ABC) as an ossifying hematoma. Thereafter, in 1942 Jaffe and Lichtenstein were the first to define ABC as an intra-osseous, osteolytic lesion, mostly affecting the metaphyseal region of long bones and vertebrae. ABCs are classified as locally aggressive lesions that infrequently undergo spontaneous healing.1 The ABC is a highly vascular lesion of unknown etiology.2 This condition is more common among children and adolescents, with more than 70% of the cases occurring during the first 2 decades of life. It is commonly occurring in the metaphysis of long bones, and especially in the distal femur and tibia. However, ABC rarely occurs in the pelvis of pediatric patients with a prevalence of only approximately 4-12%.1-4 Treatment options for ABC include direct injection of the cyst with a fibrosing agent, embolization, resection, and intralesional curettage with or without local adjuvant therapies.1,3 The adjuvant therapies might incorporate a high-speed burr, phenol or liquid nitrogen, and argon beam coagulation. The bone void can be packed with cement, bone graft substitutes, such as calcium phosphate, or definitive bone graft whether autogenic and/or allogenic.1,5 Management of pelvic ABC is challenging because of a multitude of factors, including the high vascularization of the lesion, the relative inaccessibility of the tumor, the juxtaposition of the lesion to neurovascular structures, and the vulnerability of the cartilage at the hip joint.6,7 Moreover, the reported recurrence rate of pelvic ABCs after surgical treatment is around 14%.2,7 The purpose of this case is to report an uncommon case of ABC in the ischial area that was successfully managed with intralesional excision and bone grafting.
Case Report
A 5-year-old girl presented with her parents to the orthopedic clinic at King Fahad Medical City in Riyadh, Kingdom of Saudi Arabia complaining of pain and limping on her left lower limb. Her pain started around 6 months prior to her presentation; it increased while walking, localized to her left hip area, and occasionally waking her up from sleep. According to her parents, the pain was rarely associated with episodes of night sweats. There was no history of previous trauma or falls. There was no history of concomitant fever or weight loss. The patient was not complaining of any urinary symptoms or change in her bowel habits.
The patient is a product of a normal spontaneous vaginal delivery. She was born as a full-term baby without any complications or Neonatal Intensive Care Unit (NICU) admissions. Her growth was normal and aligned with her age. The patient’s vaccination history was up-to-date when she showed up to our clinic.
The past surgical history was unremarkable. She had no known allergies and she was not on any medication at time of presentation. There was no history of similar illness occurring in her family and the family denied recent history of any kind of infection including tuberculosis (TB). In addition, the patient’s family denied any history of raw unpasteurized cattle milk ingestion.
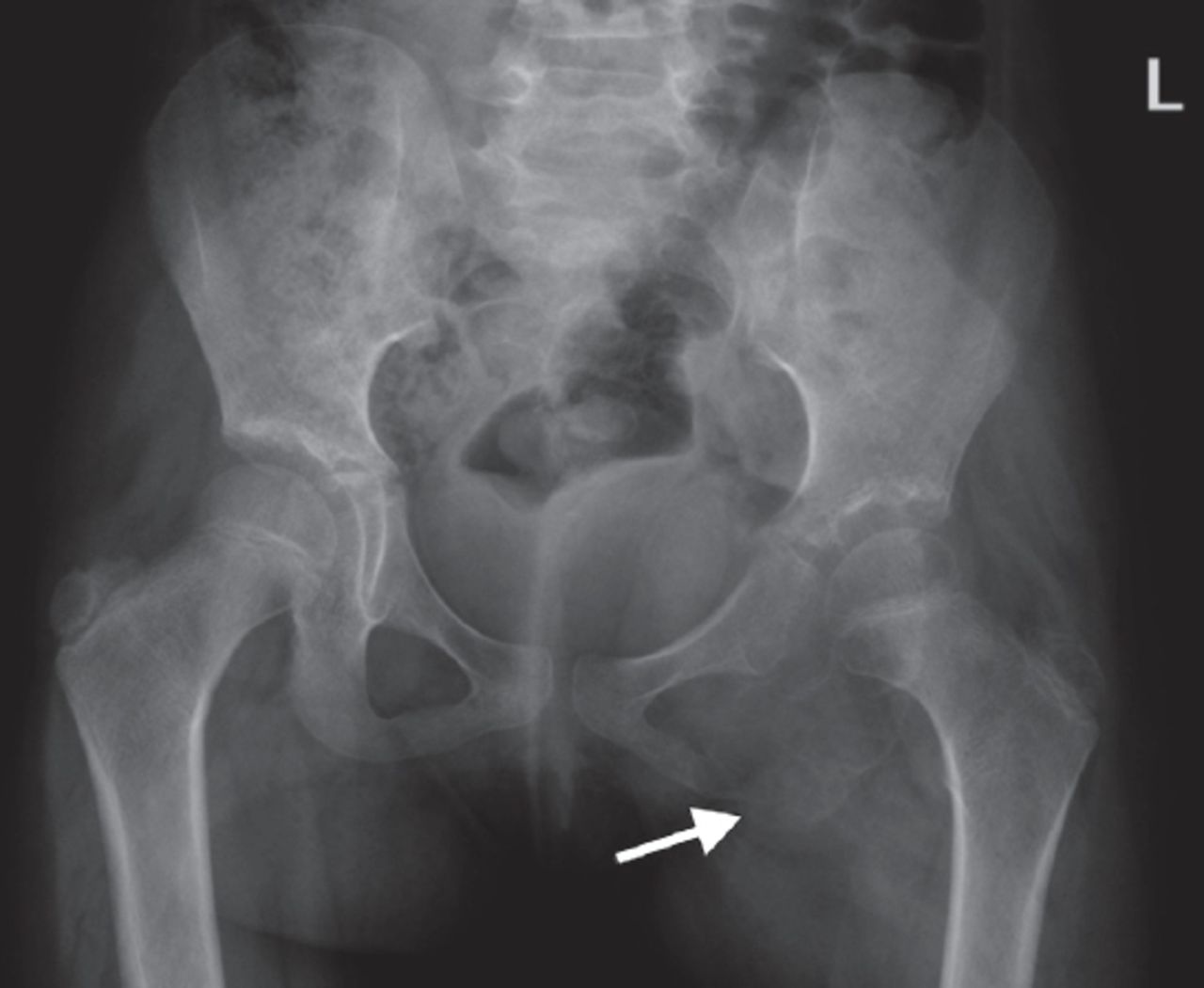
The physical examination showed a healthy looking girl. She was afebrile and her vitals signs were stable. The patient was limping on the left lower limb. On the local left lower limb exam, there was no swelling, redness, muscle spasms, or loss of sensory or motor function. Her bloodwork was normal except for a slightly elevated Erythrocyte Sedimentation Rate (ESR) of 23 mm/hr and slightly elevated plasma phosphate level of 1.5 mmol/L. The patient’s pelvic x-ray revealed expansive lytic lesion involving the ischium, suggestive of aneurysmal bone cyst (ABC) (Figure 1).

Pelvic x-ray with arrow pointing to an expansive lytic lesion involving the left ischium, suggestive of aneurysmal bone cyst (ABC).
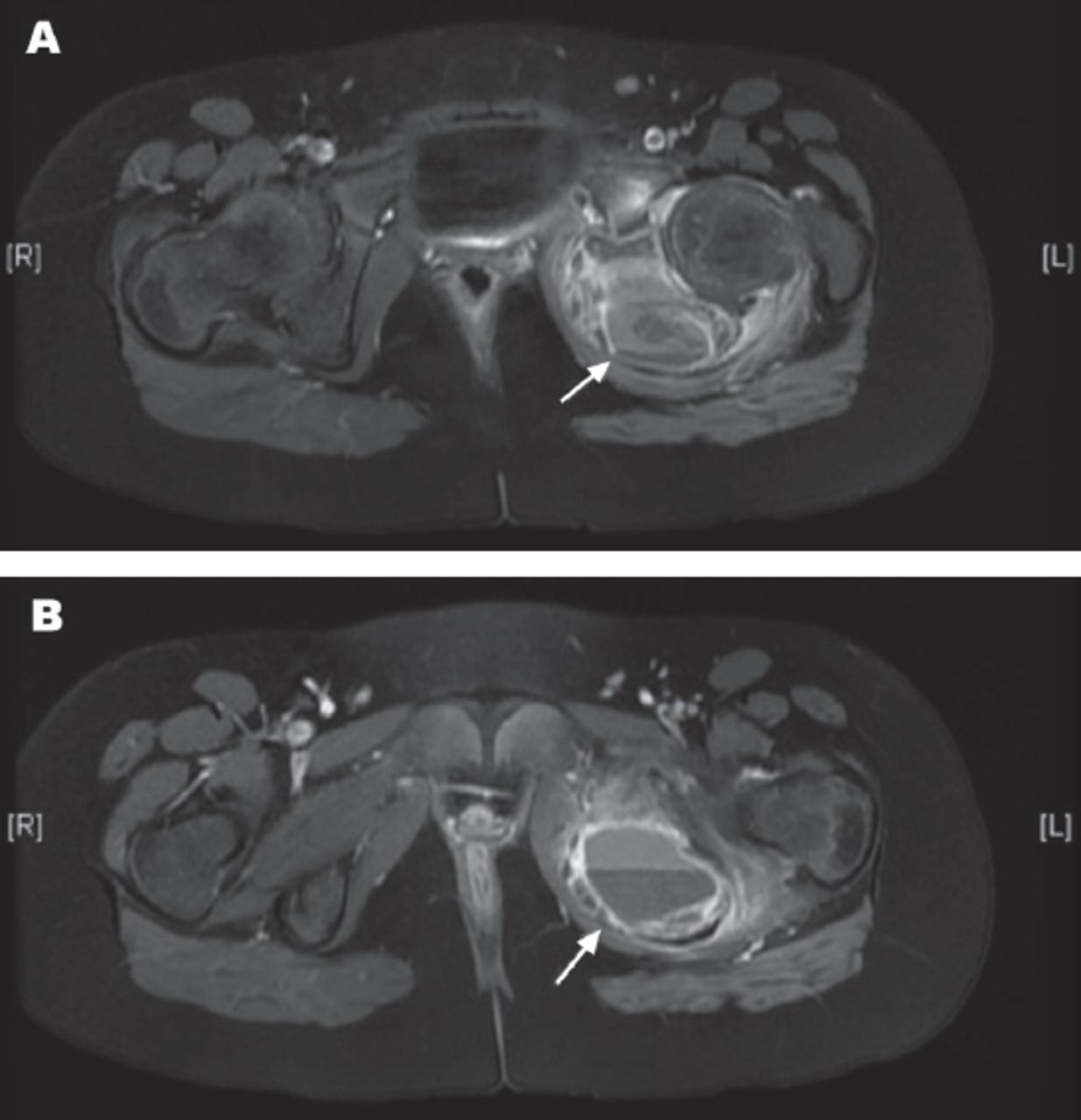
Magnetic Resonance Imaging (MRI) of the pelvis showed an expansile lesion arising from the left ischium extending to the inferior pubic ramus with multiple fluid-fluid levels of hemorrhagic component (Figure 2). The differential diagnosis at this stage included aneurysmal bone cyst, or chondroblastoma with possible ABC component, and the possibility of telangiectatic osteosarcoma was less likely, however, we kept it in consideration. The patient underwent a bone scan 2 days later to rule out any bone metastasis. The bone scan presented the same finding of the previous MRI with no evidence of bone metastasis (Figure 3).
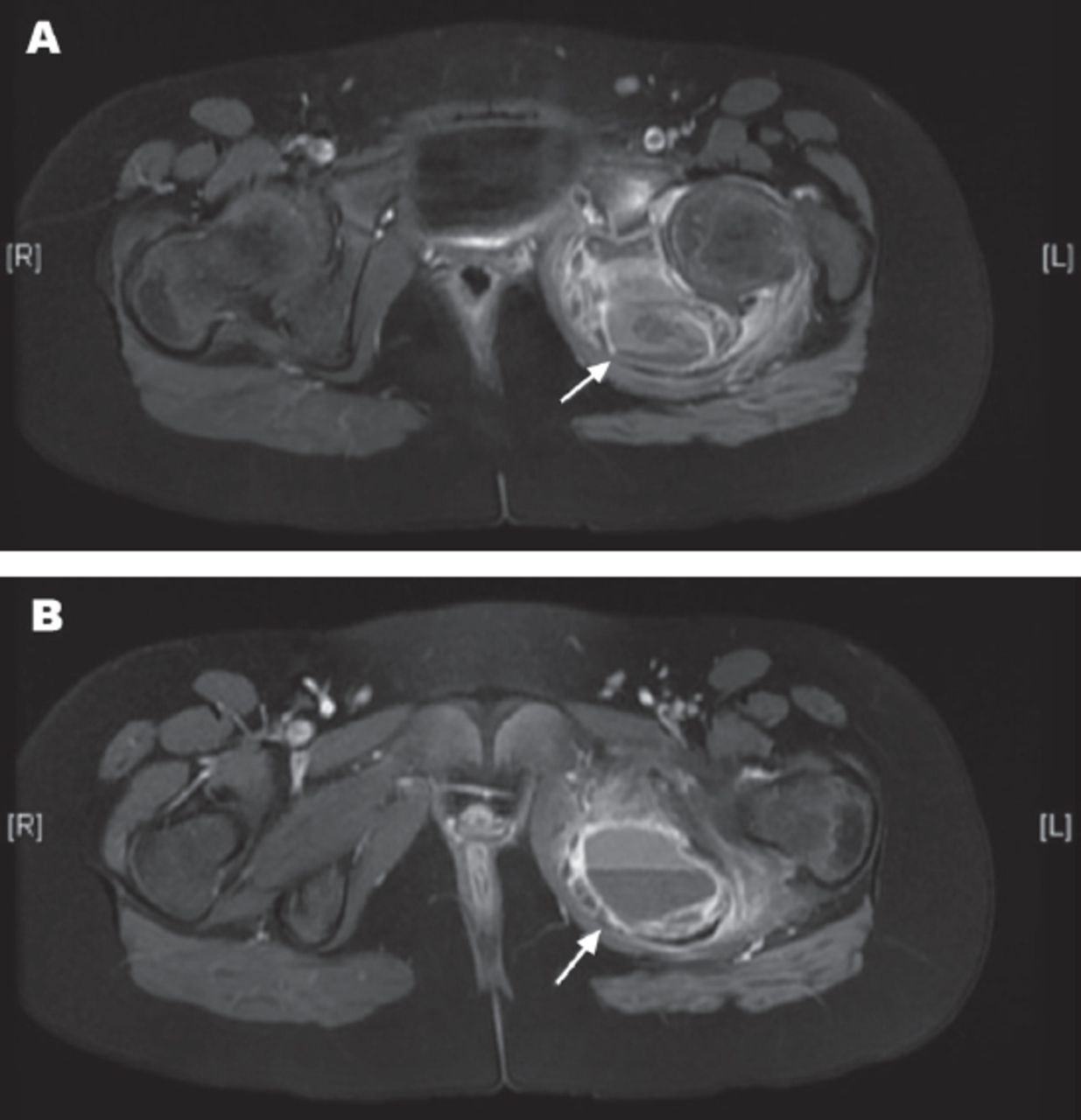
Axial MRI of the pelvis showing an expansile lesion arising from the left ischium extending to the inferior pubic ramus with multiple fluid-fluid levels (arrows) of hemorrhagic component (A & B).

Bone scan presented the same finding of the previous MRI with no evidence of bone metastasis.
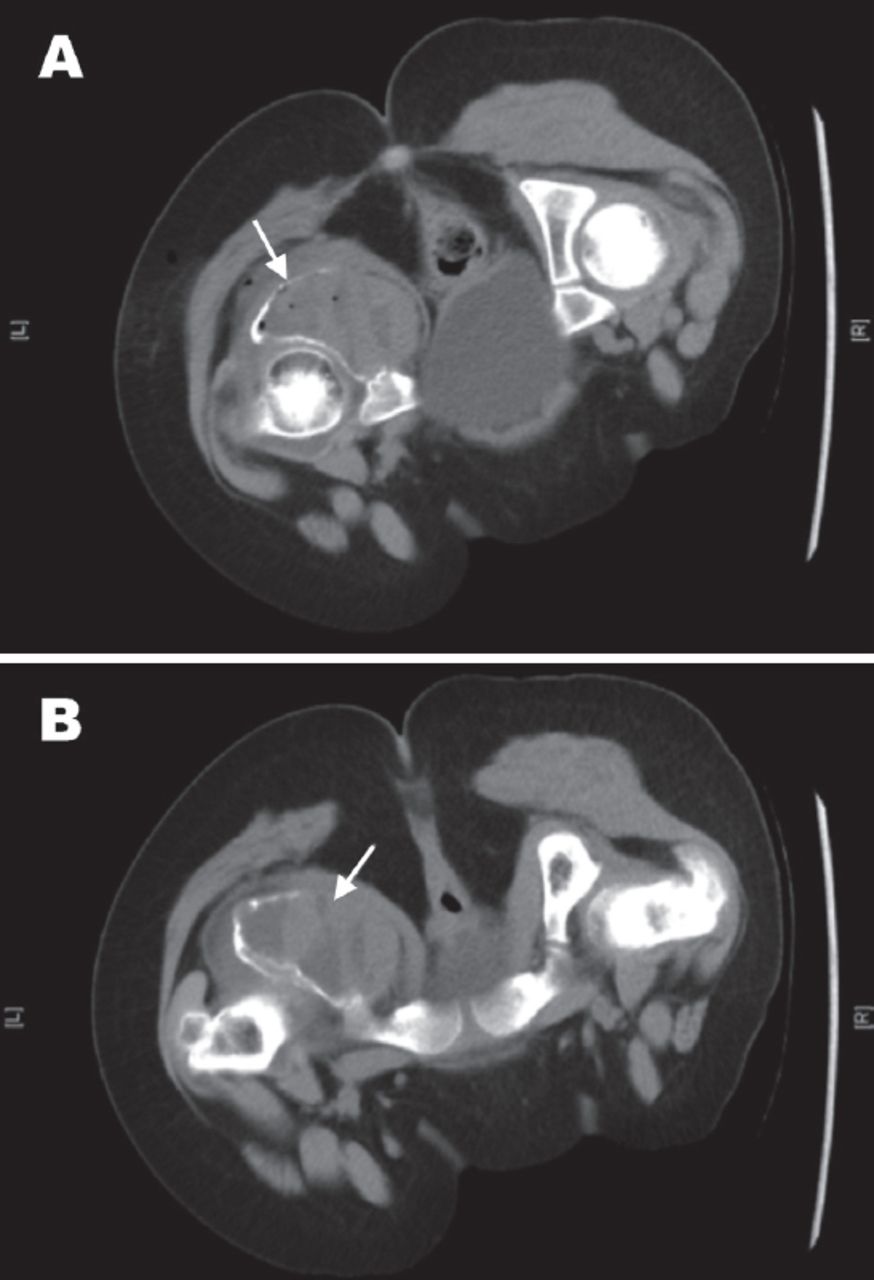
Ten days after the patient presentation, the CT guided biopsy was performed and showed Giant Cell-Rich Lesion with differential diagnosis suggestive of either giant cell tumor (GCT) or ABC. The CT images are shown in Figure 4.

Computed tomography (CT) images during the CT-guided biopsy, which showed the large expansile lesion involving the left ischium (arrows).
We discussed the case to the tumor board of our hospital. The diagnosis of pelvic ABC with involvement of the ischium was made based on the patient’s age, clinical, laboratory, and imaging findings. The surgeon sat with the family and fully explained to them the diagnosis and available treatment options. After getting consent for the surgery from the family, we booked the patient for extended intralesional curettage of ischial bone ABC and bone grafting. The surgery was performed after approximately 45 days of the patient’s initial presentation. We decided to avoid preoperative embolization in this case because there was no primary major vessel supplying the ABC in the magnetic resonance angiography imaging.
Surgery
Under general anesthesia; the patient was positioned in right lateral decubitus position and was draped in the classical manner with padding of the bony prominences. We gave a dose of preoperative antibiotic. We incorporated intraoperative fluoroscopy to identify the exact location of the tumor, and then used a posterior approach to the acetabulum. We identified the greater trochanter and the sciatic nerves. Then, we gently detached the visible tumor from the adjacent bone by periosteal elevator. Afterward, we punctured the cyst by 18-gauge spinal needle, where we sent its content to the histopathology for urgent frozen section analysis. The tissue biopsy showed abundant giant cells with no atypia, necrosis, or mitosis, which was suggestive of ABC. Subsequently, we proceeded with the bone curettage and high speed burr, followed by filling the bony defect with calcium sulfate and calcium phosphate (bone graft substitutes). Accordingly, we closed the wound in layers.
Post operatively, the patient was doing fine with no complications. We instructed the patient on postoperative rehabilitation that encompassed a strict non-weight bearing gait-training program for 6 weeks. Then, we shifted her into partial weight bearing physiotherapy program on the affected side until we gradually moved her to a full weight bearing status.
The patient continued following up with our clinic for the past 6 months. Her last x-ray 6 months postoperatively showed normal alignment of the hip joint with no sign of avascular necrosis or collapse in the femoral head (Figure 5).

Six months postoperative x-ray showing normal alignment of the left hip joint with no sign of avascular necrosis or collapse in the femoral head.
Discussion
The ABC is a benign, aggressive tumor that arises infrequently in the pelvis of the pediatric population. Primary ABCs are rare, representing 1.4% of all primary bone tumors.1,2 Rameirez et al3 in their case series reviewed 28 cases of pediatric ABCs. They identified that children with ABC had a distinct clinical and pathologic entity, where it arises de novo and rarely, if ever, represents a degenerative form of pre-existing tumors.3
Aneurysmal bone cyst clinical features vary, but most often the patient presents with local pain, tenderness, and swelling or a pathologic fracture. The plain radiographs display a radiolucent area with expansion and apparent septations.4,5 In magnetic resonance imaging (MRI), ABC regularly reveals a double fluid density with low-intensity signals on T1 and high-intensity signals on T2. The theory behind the double fluid density is the illustration of settling of cellular blood components from the serum portion of the fluid, while the patient is immobilized during the MRI study.8
Pelvic ABCs could involve the acetabulum or the triradiate cartilage, which increase the technical challenges during surgical treatment and has potential implications on the growth and development of the hip joint.4 In our case, the ABC originated from the ischium. The lesion did not fairly damage the acetabulum and the triradiate cartilage. This will hopefully reduce the likelihood of developing a delay in her lower limb growth or early arthritis in her hip joint. Cottalorda et al2 in a study of 15 children with pelvic ABCs pointed out that the most common presenting symptom of pelvic ABC was hip pain followed by a limp, which was also observed in our study.
Treatment of pelvic ABCs is difficult because of the relative inaccessibility of the tumor, and high vascularization of the lesion, which increase the risk of intraoperative bleeding, proximity of the lesions to neurovascular structures, and the vulnerability of the cartilage at the hip joint. Treatment modalities for pelvic ABCs include injection with a fibrosing agent, embolization, resection and intralesional curettage with or without local adjuvant therapies.4,8,9 In our case report, we decided to manage the patient with excision-curettage (extended intralesional curettage) and filling the void with bone graft substitutes. We elected this management approach due to the location of the lesion in the ischium and the size of the lesion, which is more than 5 cm. Our management is in alignment with Papagelopoulos et al,7 who suggested to adjust method of treatment in pelvic ABCs according to the extent and aggressiveness of the lesion. They recommended intralesional curettage, with or without bone grafting for lesions <5 cm that exhibit minimal destruction, which do not threaten the integrity of the acetabulum. On the other hand, lesions of >5 cm necessitate a more aggressive approach with the excision-curettage technique.
In conclusion, management of pelvic ABC is challenging due to the aforementioned factors. Intralesional curettage and bone grafting are still valid treatment options for ABC in the ischial region. Aggressive excision is required for large destructive lesions.
References
*References should be primary source and numbered in the order in which they appear in the text. At the end of the article the full list of references should follow the Vancouver style.
*Unpublished data and personal communications should be cited only in the text, not as a formal reference.
*The author is responsible for the accuracy and completeness of references and for their correct textual citation.
*When a citation is referred to in the text by name, the accompanying reference must be from the original source.
*Upon acceptance of a paper all authors must be able to provide the full paper for each reference cited upon request at any time up to publication.
*Only 1-2 up to date references should be used for each particular point in the text.
Sample references are available from: http://www.nlm.nih.gov/bsd/uniform_requirements.html
Acknowledgment
The authors would like to thank Dr. Walid Asaad, Radiologist at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia for participating in attesting to the imaging clarity and correctness.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received November 16, 2015.
- Accepted May 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.