


Abstract
Objectives: To assess the rate of bacterial contamination of the multi-use vial and single-use packed glucose meter strips, and to identify the type and frequency of various bacterial contamination in different hospital wards.
Methods: This prospective observational study was conducted by a team from the Strategic Center for Diabetes Research in 7 general hospitals in the Central region of Saudi Arabia during the period from August to September 2014 to assess the bacterial contamination rate of the unused strips. A total of 10,447 strips were cultured using proper agar media and incubated both aerobically and anaerobically.
Results: The total bacterial contamination rate for the multi-use vials glucose strips was 31.7%, while single-use packed strips were not contaminated at all. Ministry of Health hospitals had the highest contamination rates compared with other hospitals. Critical, obstetric, and surgical wards had the highest bacterial isolates number, where most were in the risk group 3 according to the National Institute of Health guidelines. Staphylococcus species were the most common bacteria found.
Conclusion: Glucose meter strips should be recognized as a source of bacterial contamination that could be behind serious hospital acquired infections. The hospital infection control team should adopt proper measures to implement protocols for glucose meter cleaning and glucose strips handling.
There is no doubt that hospital-acquired infections (HAIs), are the most frequently occurring adverse events in health-care delivery worldwide, and there is significantly a high mortality rate as a result of nosocomial infections resulting in 17,500-70,000 deaths annually in the United States (US) only.1,2 There are also significant annual financial losses occurring due to HAIs worldwide, wherein, it was estimated to be 7 billion Euro in Europe and 6.5 billion United States Dollar in the US.3 The roles of medical equipments, categorized as; critical, semi-critical, and non-critical in the transmission of HAIs, has long been documented in the hospital setting.4-6 Medical devices, such as glucose meters and its associated glucose strips can be a source of nosocomial infection, especially with immune-compromised patients like patients with diabetes. For instance, glucose meters have been held responsible for the transmission of viral and bacterial infection via blood contamination or human handling,7-10 especially when these portable glucose meters have become a standard practice for routine glucose assessment in hospital wards.11,12 Previous studies7,13 showed that the incidence of cross contamination in glucose meters strips was much higher when using multi-use vials when compared with the single-use packed glucose meters test strips. It was also found that the prevalence of bacterial contamination with pathogenic bacteria ranged from 25.7-80% in multi-use vials, while it was only 3-7% in individually packaged strips.13 Moreover, in 2 Spanish7 and French13 multi-use glucose meters strips studies, the bacterial contamination rate ranged between 25.7-33%, where most of the contamination occurred in both surgical and medical wards. Even though these studies were limited with the number of hospitals involved and strips distributed, one important conclusion derived from these previous studies was that using dedicated single-use packed glucose strips would limit or eliminate cross contamination. Therefore, the current study aimed to investigate the rate of contamination and type of bacteria for both multi-use vials and single-use packed glucose strips in larger number of hospitals, in wider spectrum of hospital wards with a higher number of distributed strips in Riyadh, Kingdom of Saudi Arabia (KSA). Factors behind the high contamination rates were studied and the type of bacterial contamination was classified according to the National Institute of Health (NIH) microorganism risk categories.14
Methods
Study design and setting
This is a prospective observational study conducted in various randomly selected hospital wards in 7 general hospitals during the months of August-September 2014 assessing the contamination rate for single used packed glucose strips versus multi-use vials glucose strips.
The selection of these hospitals was aimed at including all different health sectors, providing health services in the Kingdom. Three Ministry of Health (MOH) general hospitals, including Al Iman General Hospital, Al Yamama Hospital, and King Salman Hospital were selected with bed capacity ranging between 207-305 referred to as MOH1, MOH2, and MOH3, and 2 university hospitals (UH), including: King Abdulaziz University Hospital, and King Khalid University Hospital referred to as UH1 and UH2 with bed capacity of 98 and 974 beds. One military hospital: Security Forces Hospital referred to as (MH) with bed capacity of 600 beds, and one private hospital: Sulaiman AL-Habib referred to as (PH) with 463 beds capacity were selected to be enrolled in this study. Those hospitals were randomly selected from a total of 50 hospitals in Riyadh city, KSA including hospitals from different health sectors that have different hospital management system.
To ensure a broader age spectrum, different hospital wards were selected, which included neonatal, pediatrics, and adults, and the following hospital wards, namely: medicine, surgery, Obstetrics and Gynecology (OB GYN), ear, nose, and throat (ENT), and Ophthalmology were included to ensure different medical subspecialties. Intensive Care Units (ICU) were also involved to show the intensity of care with regards to general wards as shown in Table 1.
Percentage of distributed, cultured, and contaminated glucose strips for the multi-used vials and single used according to the participated hospital wards.
Equal number of the multi-use vials (OneTouch, LifeScan, Inc. Johnson and Johnson [Middle East] Inc. Dubai-UAE), and single-use packed glucose meters test strips (FreeStyle Optium, Abbott Diabetes Care Ltd., [Witney, UK], distributed by Mediserv, Riyadh, KSA) were distributed in the selected hospital wards through a well-trained research team, wherein, each ward received 200-300 strips for each glucose meter. These strips were distributed using an aseptic transportation system. All the nurses of each ward enrolled in this study, received training on the usage of the 2 glucose meters. All these nurses in the selected wards were unaware of the objectives of this study to eliminate any bias and were instructed to use both glucose meters alternatively when testing blood glucose at the patient’s bedside.
The research team was also instructed to collect the remaining glucose meter strips in aseptic bags when more than half of the package had been used. The ward exposure for each glucose meter’s strips ranged between 3-8 days averaging at 5.5 days.
All the unused glucose meters’ strips were collected in aseptic bags and transported to the main microbiology laboratory located at the Strategic Center for Diabetes Research using sealed containers at temperature between 4-10°C.
On the same collection day, each strip was placed in 10 ml of peptone water (Watin-biolife, Saudi Arabia) and vortexed (Vortex Mixer, Gemmy industrial cooperation, USA) for 10 minutes. Then 100 µl of each sample was spread over sheep blood agar plates, Clostridium difficile selective media, Eosin Methylene Blue medium and MacConkey agar medium (Watin-biolife, Saudi Arabia) and incubated both aerobically and anaerobically at 37°C (Memmert, Germany). Viable bacteria were counted after 3 days of culture. One or more colony forming units (CFUs) per strip was considered as a positive result. Bacterial colonies were then stained using PREVI® Color Gram Automated Gram Staining (Biomeriux, France). Microbial identification for the recovered bacteria was conducted using automated VITEK® 2 system using the VITEK®2 GN ID for Gram-negative bacteria and VITEK®2 GP ID for Gram-positive bacteria (Biomeriux, France). A list of names for screened Gram positive and Gram-negative microorganisms using VITEK® 2 system (Biomeriux, France) could be found at the following link: http://www.biomerieux-diagnostics.com/vitek-2-identification-cards.
All the bacteria were classified to its corresponding health risk group using NIH 2002 guidelines for research involving recombinant DNA molecules. Risk group 1 consisted of microorganisms that are not associated with human disease, while risk group 2 consisted of those microorganisms that are rarely serious and can be treated, risk group 3 consisted of microorganisms that are serious or lethal to humans with available therapeutic intervention, and risk group 4 consisted of microorganisms that are serious or lethal for humans and for which therapeutic interventions are not usually available. The cultured bacteria were classified in these groups according to the currently available evidence.
This study was reviewed and approved by the Institutional Review Board in the College of Medicine, King Saud University, Riyadh, KSA. Consent was not obtained for the data used in this publication since this study did not compromise anonymity or confidentiality, or breach of local data protection laws. Additionally, blood glucose testing is a part of the standard procedures for glucose monitoring for admitted patients, and no additional risks have occurred due to study procedures.
Statistical Analysis
The statistical analysis was performed using the Statistical Package for Social Sciences version 21 (IBM Corp., Armonk, NY, USA). Frequencies and percentages were used to represent the data. P<0.05 was used as a level of significance.
Results
This study was conducted at 7 hospitals with a total bed capacity of 2861 beds in different randomly selected wards as shown in Table 1. The total number of nurses involved in this study was 493 nurses, ranging between 3-40 nurses per hospital ward and averaging at 12.3 nurses per ward. The total number of patients subjected to this study was 488 patients, ranging between 7-60 patients and averaging at 12.2 patients per hospital ward.
The total number of distributed strips was 17,800 strips averaging at 445 strips per ward with 8900 of single-use packed and 8900 of multi-use vials glucose meter strips, ranging between 400-600 strips per ward. A total of 7353 strips were used for glucose testing from the total distributed strips in all hospitals averaging to 183.8 strips per ward, while the unused 10,447 (58.7%) strips were transported for contamination study averaging at 261.2 strips per ward. Out of the total distributed strips, 59.5% from multi-use vials and 57.9% from single-use packed strips were unused and were cultured and further tested for contamination. This implies that equal numbers of strips were received from the 2 glucose meters used in this study.
Contamination rate
The overall bacterial contamination rate for multi-use vials strips was 31.7%, while it was 0% for the single-use packed strips. The highest contamination rate was 50.9% in MOH1 hospital. The other MOH hospitals showed contamination rates of 37.6% for MOH2, and 29% for MOH3. The lowest rate of contamination was found in UH2 at 24.3%, while it was higher in UH1 reaching 30.3%. The MH had a contamination rate of 26.2% and the PH had a contamination rate of 27.3% (Figure 1). The percentages of cultured glucose meter strips from the total distributed stripes for each hospital were almost identical at a range between 55-60%.

Number of contaminated and uncontaminated tested glucose strips and contamination rate in the participated hospitals. MOH - Ministry of Health hospital, PH - private hospital, UH - university teaching hospitals
This study showed that 2 surgical and one medical male wards, in addition to one OB GYN general ward had contamination rates more than 50% in the multi-use vial strips, while there was no contamination in those wards in the single-use packed strips. All those 3 wards were in the MOH hospitals. On the contrary, one medical ward in the MH and 2 general OB GYN wards in the UH and MOH hospitals did not demonstrate any contamination in the 2 glucose meter strips.
Seventeen wards showed bacterial contamination rates above the average of the total hospital wards (31.7%) but less than 50%, where most of them were from MOH hospitals, while 16 wards had contamination rate below the overall average rate, mainly UH, MH, and PH hospitals as shown in Table 1.
Types of microorganisms
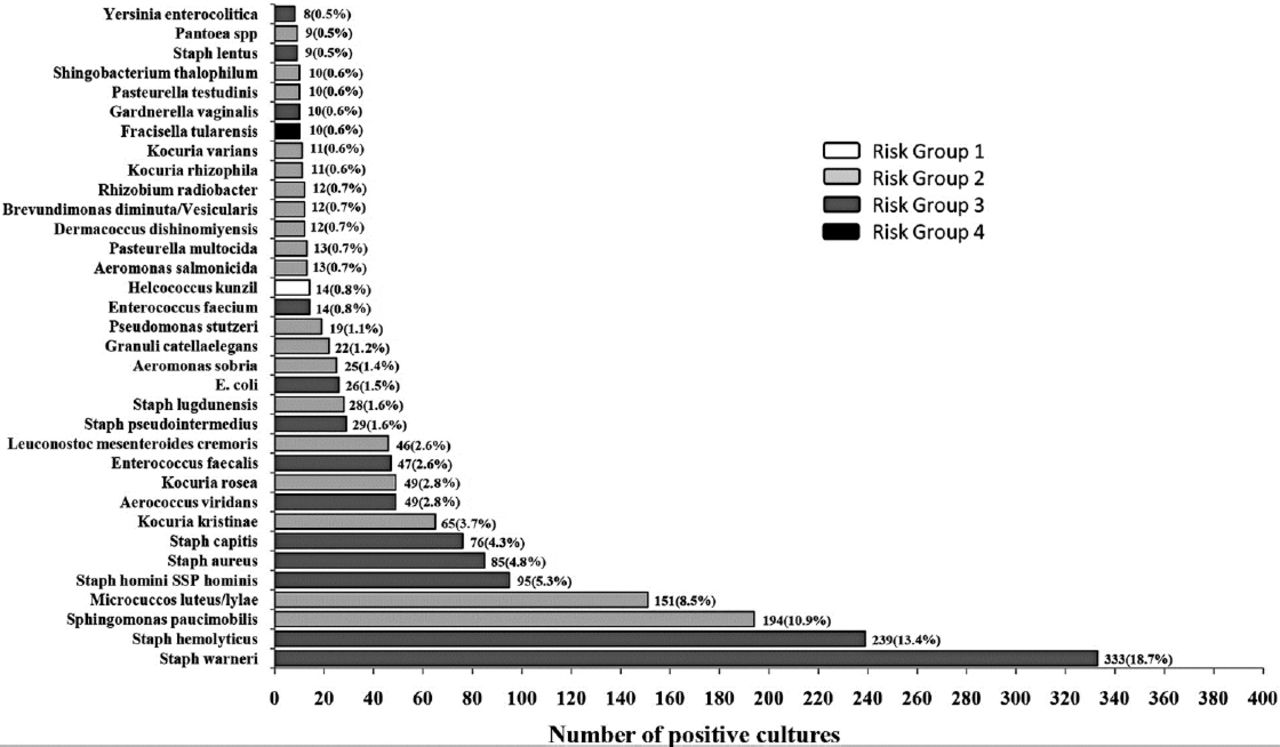
Figure 2 demonstrates the rate of contamination according to bacterial type using NIH infectious microorganism risk guidelines.14 There was only one microorganism classified as risk group 1, namely: Helcococcus kunzii bacteria, which was found in pediatrics ward at UH2 contributing to 0.8% of the total contamination rate. There were 19 microorganisms classified as risk group 2 ranging between 0.51-10.9% of the total contamination rate. Risk group 3 microorganisms were higher in frequency when compared with other risk groups ranging between 0.45-18.7%. The most frequent bacteria were Staphylococcus warneri contributing to 18.7% and Staphylococcus haemolyticus contributing to 13.4% of the total contamination rate. Francisella tularensis was the only bacteria in the risk group 4 and was discovered in the Neonatal Intensive Care Unit (NICU) at MOH1 hospital.
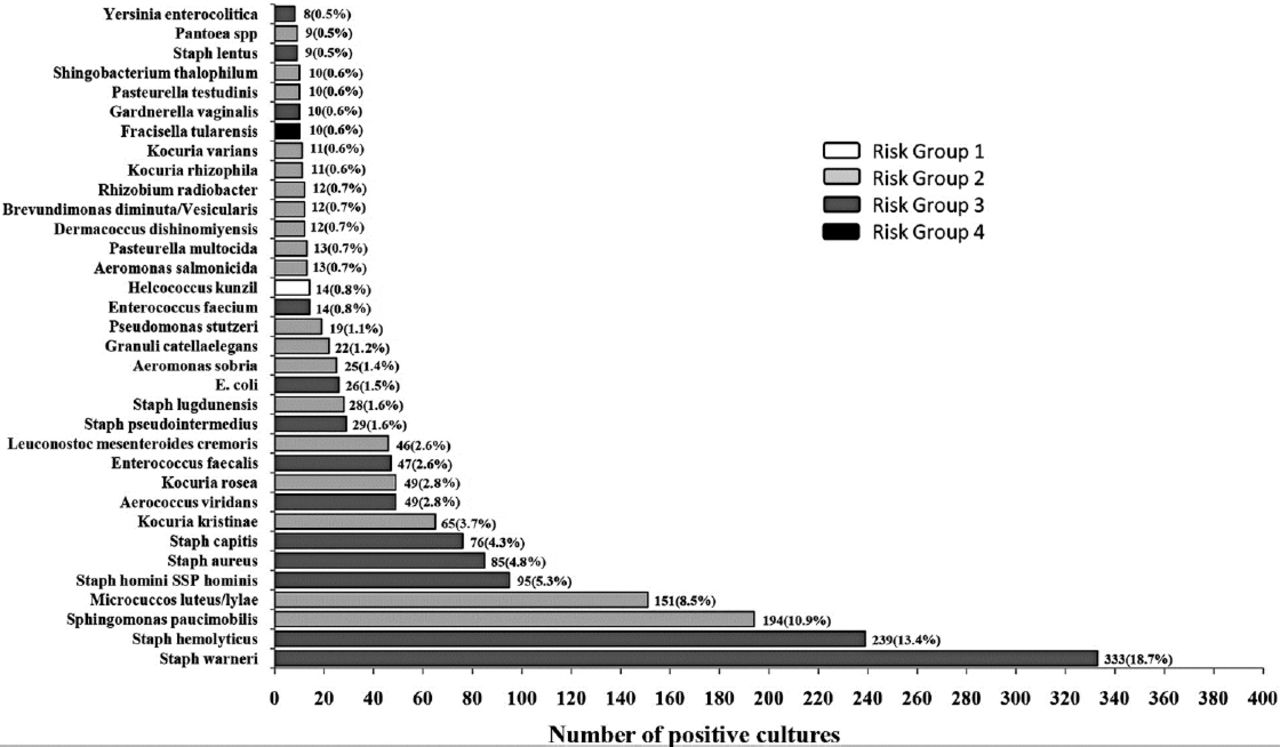
The number and frequency of different microorganisms classified according to the NIH risk classification. E. Coli - Escherichia coli, MOH - Ministry of Health hospital, UH - university teaching hospital, PH - private hospital, MH - military hospital
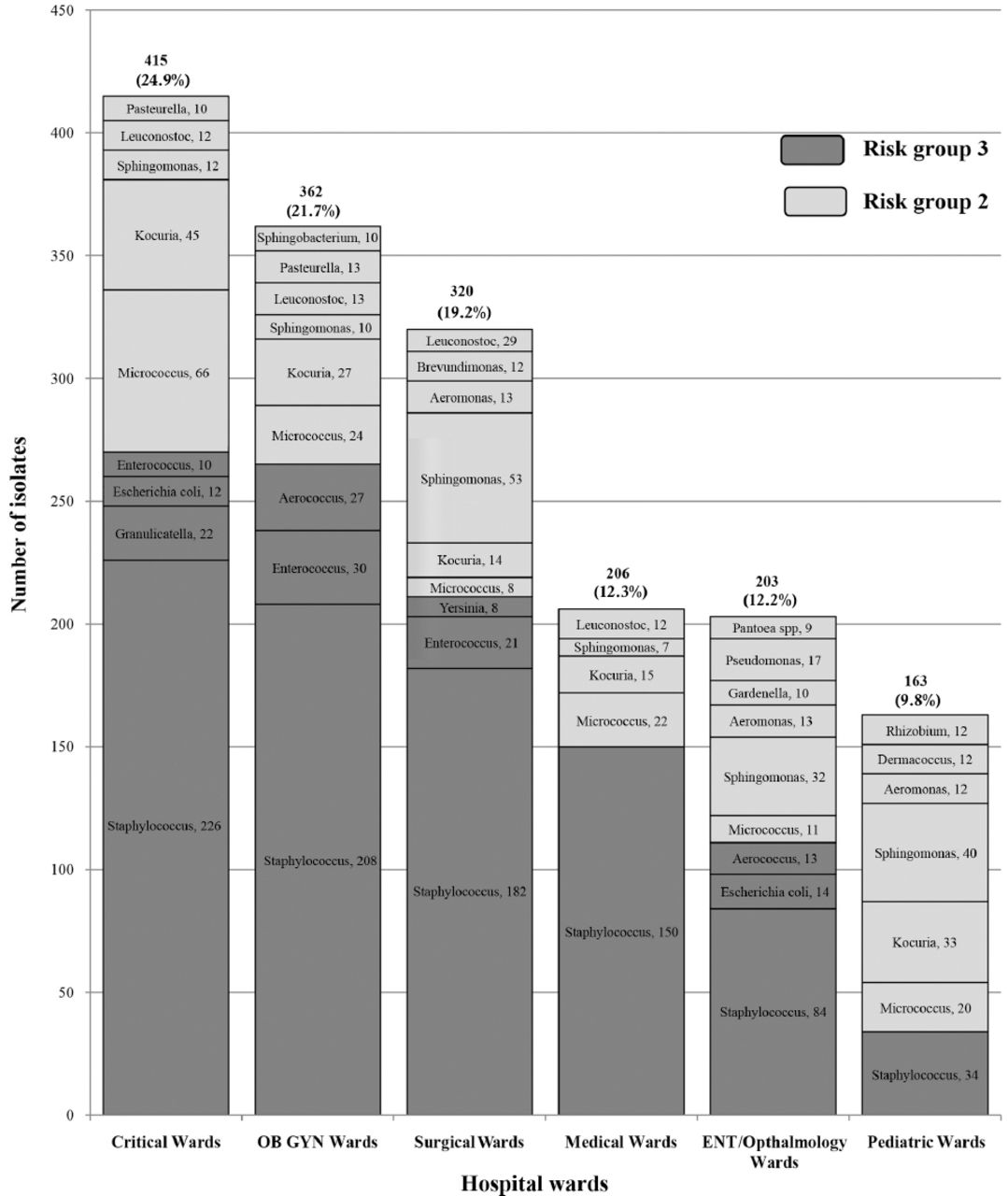
The highest numbers of contamination isolates were found in the critical care wards, namely: Intensive Care Unit (ICU), NICU, and Critical Care Unit (CCU), where it exceeded 400 isolates accounting for 24.9% of the total isolates. The OB GYN ward exceeded 350 (21.7%) isolates, which was followed by surgical ward that exceeded 300 (19.2%) isolates. The lowest contamination isolates were in the Medical wards at 206 (12.3%), ENT/Ophthalmology at 203 (12.2%), and the Pediatrics ward at 163 (9.8%) (Figure 3). The Staphylococcus species were the most frequent isolates in all hospital wards, followed by Micrococcus and Sphingomonas species isolates from all wards. Kocuria was present in all the previously mentioned hospital wards except ENT/Ophthalmology. The Leuconostoc species were isolated from critical care, OB GYN, and medical wards, while Aeromonas species were isolated from other hospital wards, namely: ENT, surgical, and Pediatrics wards.
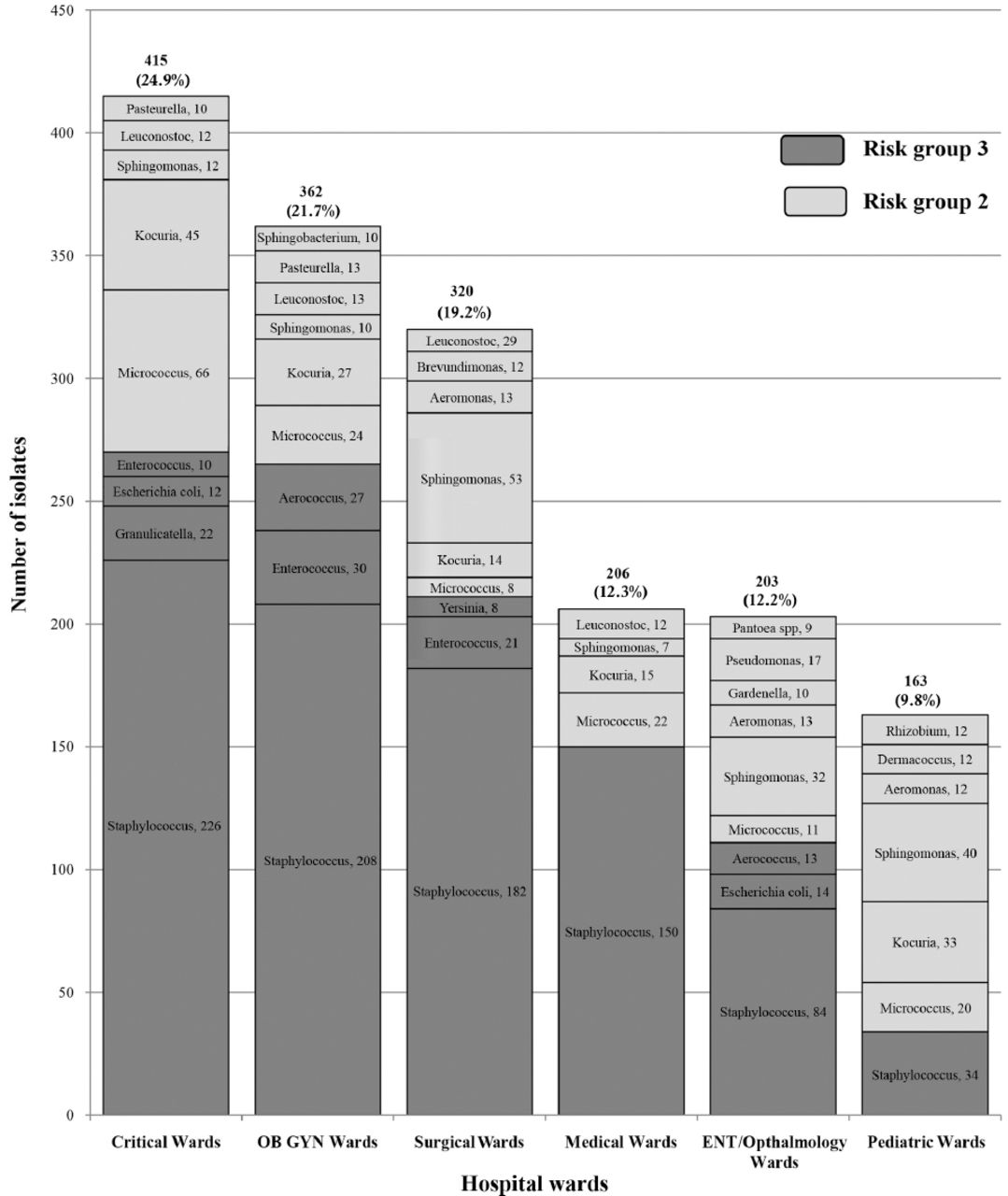
Number of contaminated isolates according to the identified microorganisms distributed according to major hospital wards. ENT - ear, nose, and throat, OB GYN - obstetrics and gynecology
In the critical (CCU, ICU, and NICU), OB GYN and surgical wards, more than 50% of the cultured bacteria belonged to risk group 3 microorganisms. Medical, ENT, and Ophthalmology wards were having identical numbers of contamination isolates, where more than 60% were considered to be risk group 3 microorganism. The lowest number of isolates classified as risk group 3 was found in the pediatric ward, where it was less than the quarter of the total isolates. The Staphylococcus, Enterococcus, and Aerococcus were the most common bacteria belonging to risk group 3 microorganisms isolated from almost all hospital wards, while Micrococcus, Kocuria, Sphingomonas, and Leuconostoc were the most common in risk group 2 microorganisms that were found in most of the hospital wards.
Hospital wards contamination
When compiling the bacterial contamination rates for different hospital wards, the OB GYN, and critical wards had the highest contamination rate at 49.8% followed by surgical male wards (46.4%), female (45.4%), and surgical day care wards at 45%. The ENT had bacterial contamination rates of 40.7% and the Ophthalmology wards had bacterial contamination rates of 39.9%. Critical care units had a wide range of contamination rate being with the highest contamination rates observed in NICU and the lowest in CCU. The lowest bacterial contamination rate was observed in ENT/Ophthalmology female ward at 13.4% in Table 2.
The classification of microorganisms’ species according National Institute of Health guidelines for all participating hospital wards arranged according to the contamination rate.
As mentioned previously, there was only one microorganism that belonged to risk group 1, which was Helcococcus kunzii and another one, Francisella tularensis belonging to risk group 4, while rest of the bacterial isolates were categorized as risk group 2 and 3 (Table 2). Among risk group 2 microorganisms, Kocuria species were found in most of the hospital wards followed by Micrococcus and Sphingomonas species with different percentages, while the other types of microorganisms among this group were also seen in almost all hospital wards. The Staphylococcus with its different pathogenic species were the most grown bacteria found in almost all the wards that were categorized as risk group 3. Enterococcus species were found in surgical, NICU, and OB GYN wards. Other bacteria among this group were also cultured, but in less frequency as shown in Table 2.
Discussion
The overall contamination rate was 31.7%, which is similar to what the French13 and Spanish7 studies have found in the years 2011 and 2013. The 3 MOH hospitals in this study were found to have the highest rate of bacterial contamination averaging at 39.2% that could be a reflection of poor adherence to infection control guidelines, especially when the rest of the hospitals: UH, MH, and PH had significantly lower rates of bacterial contamination.
Although there have been no studies that looked into hospital wards glucose meter bacterial contamination rates, studies on other hospital equipments reported that more than 70% of all sampled equipment were contaminated ranging between 31-100%.15 Another study showed that, the overall frequency of glucose meters contamination with blood was 30.2% with a range of 0.0-60.5% and 34.6% as a median,10 that may indicate the high possibility of bacterial contamination of glucose meters device.
Since glucose meters are less likely to have a standard cleaning protocol, they could be the source of bacterial contamination for the glucose strips that will be in direct contact with the patient. On the other hand, it has also been reported that, the health care workers would clean their hands only After handling 30% of the patients contact and after 50% of their daily activities; which could also be a source of glucose strips contamination.16 This could explain the wide variation in the bacterial contamination rates in this study from no contamination to almost 60% that was observed in different hospitals wards.
This study has shown that using multi-use glucose strips vials is associated with bacterial contamination; while single-use packed strips did not demonstrate any contamination in the studied hospitals wards. This could be the result of the strict aseptic technique used in glucose strips delivery to the hospital wards and transportation of unused strips to the microbiology laboratory. The single-use packed strips were subjected to the same hospital environment as the other multi-use strips vials and they were only opened in the laboratory where there was no direct hospital staff contact with those strips. Our study differs from what the Spanish study had previously shown, where they had a 7% contamination rate of the single-use packed strips, which could not be explained and they also did not mention the way those strips got contaminated, unless they were contaminated in the microbiology laboratory when they were opened. In our study, having 0% bacterial contamination rate of single-use packed strips functions as a quality assurance of the different study steps involving distribution, hospitals ward exposure, and transportation. The patient to nurse ratio was 2 to 1 in this study, although it was lower in MOH hospitals when compared with other hospitals, while the glucose strips distributed to patients ratio was 20 to 1 in almost all hospitals. This may have contributed to the wide variation in the bacterial contamination rate seen in different wards, where it was the highest in MOH1 OB GYN general ward with the patient to nurse ratio of 3 to 1 and no contamination in the UH2 OB GYN ward, with a ratio of 1 to 1. This could also indicate that, less number of nurses would expose them to more workload and there would be less chance to adhere to cross infection guidelines protocols. The high rate of bacterial contamination was seen in the general wards: medical, surgical, or OB GYN, where patient to nurse ratio was the lowest being 3 to 1. Each intensive care units, namely: ICU, NICU, and CCU had an average bacterial contamination rate of 31.8% which is considered very high relating to the nature of patients in these wards that warrant good attention to cross infection. When all those units were added together, they had the highest bacterial contamination rate, mainly with risk group 3 bacteria (Figure 3). These neglected serious problems need more focus on the cross infection protocol used in these units since patients to nurses’ ratio is appropriate.
Half of the wards involved in this study regardless of their nature, were having bacterial contamination rates above the average rate seen in this study (31.7%), with around half of them being from the 3 MOH hospitals. One quarter of the studied hospital wards had no or less than average bacterial contamination rate distributed in all the 7 hospitals.
This study, demonstrates similar findings to other studies, where Staphylococcus with its different species is the most common microorganism, which is among the risk group 3 according to the NIH guidelines.14 The second most common bacteria among this group was Enterococcus and Escherichia coli, which was consistent with both Spanish7 and French13 findings, although both studies screened for very limited number of bacteria. Among risk group 2, which is less virulent, Kocuria, Micrococcus and Sphingomonas species were the most common bacteria cultured from glucose meters’ strips in different wards. This was similar to the observation also found in the French13 study, although they did not report the contamination rate, which could have been compared with our data.
Our study also showed an alarming observation that risk group 3 microorganisms, which are more virulent had an average bacterial contamination rate 2 times higher than risk group 2 at 4.4% versus 2.1%. When looking at the critical, OB GYN, and surgical wards, this study showed that these wards had a larger number of bacterial contamination isolates with the highest percentage of risk group 3 microorganisms, similar to other studies that showed the contamination rate in ICU equipments to be at 88%.17 Since those 3 hospital wards had patients susceptible for HAIs due to the nature of patients’ illness or the presence of surgical wounds, this observation acts as a strong evidence to recognize the glucose meter strips to be a source of cross contamination. As expected, medical, ENT, Ophthalmology, and pediatrics wards had less number of bacterial contamination isolates and lower percentage of risk group 3 microorganisms. This could be a reflection of better adherence to hospital cross infection guidelines or the nature of patients admitted in those wards or less workload among medical staff.
Current studies18 indicate that up to one third of the infection acquired in the health care setting could be prevented by proper hand washing and equipment cleaning guidelines. The non-critical equipment and their disposable accessories are unlikely to have cleaning protocols making them more susceptible to be contaminated with microorganisms. It is now the time to draw more attention toward this problem and to implement strict guidelines that would minimize cross infection by adopting proper handling and cleaning protocols.
Strengths and limitations
The main strength of this study lies in being a large study related to the number of strips distributed and the widest in acquiring different hospitals from various health sectors covering almost all types of hospital wards. This study was adjusted for the number of distributed strips, wards’, patients’ number, and number of nurses involved in the glucose testing, in addition to glucose strips exposure time eliminating any variation in contamination rate due to the length of exposure. The other strength of this study is in using a completely aseptic technique in the strips delivery to the hospital wards and transportation of unused strips to the microbiology laboratory, which eliminated any contamination outside the hospital wards. This study was limited by the use of VITK ID cards for identification of both Gram-positive and Gram-negative microorganisms that are commonly reported in hospital settings in Saudi Arabia, which might have missed some of the uncommon microorganisms. Another limitation was the lack of bacterial list for NIH risk group classification, which warranted us to classify cultured bacteria according to the best of our knowledge. In addition, we have chosen to omit the brand names for single-use packed and multi-use packed strips glucose meter strips to avoid any misinterpretation.
In conclusion, the high prevalence of glucose meter strips bacterial contamination could be attributed to many factors that can be modified. Multi-use glucose meter strips vials subject them to contamination, which is not the case when a single-use packed glucose meter strips are used. Adherence of hospital staff to cross infection protocols and proper hand wash guidelines may minimize contamination rate. Other factor, which could be important to minimize contamination and cross infection, is controlling hospital staff workload that will allow them to adhere to the cross infection protocols and reduce the frequency of contamination. As this study has shown variable rates of bacterial contamination in different hospital wards, these factors have to be taken more seriously in certain wards, especially critical and surgical wards that have been proven to have the highest bacterial contamination rates, which may be responsible for both morbidity and mortality. More than half of the bacteria contaminated multi-use glucose meter strip vials were classified as risk group 3 that are considered to be more virulent, especially Staphylococcus species. This indicates that cross contamination through glucose meter strips could be a source of bacterial infection, especially in immunocompromised patients, such as diabetic patients.
It is the time to consider glucose meter strips as a potential risk for hospital cross infection, which may result in serious infections and to adopt specific protocols for the cleaning of glucose meters and proper protocols for the handling of glucose strips. On the other hand, using single-use packed strips may minimize this problem in the hospital setting. This study also draws attention to the infection control team in each hospital stating clearly that glucose meter strips could be a source of hospital cross infection.
Acknowledgment
The authors would like to acknowledge the Research Unit team, the hospitals involved, and all staff nurses in different wards for their participation in conducting the study. The authors would also like to acknowledge the Pharmaceutical Company Abbott Laboratories S. A, Dubai Healthcare City, Dubai, United Arab Emirates for funding this study.
Footnotes
Disclosure. Authors have no conflict of interest. The study was funded by the Pharmaceutical Company Abbott Laboratories S. A, Dubai Healthcare City, Dubai, United Arab Emirates.
- Received March 9, 2016.
- Accepted June 29, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.