


Abstract
Objectives: To assess the number of Saudi patients diagnosed with narcolepsy in 2 tertiary centers before and after the introduction of the 2009 A(H1N1)pdm09 vaccine.
Methods: We started collecting data after the first international report of an association between the A(H1N1)pdm09 vaccine and narcolepsy between January 2010 and December 2016. All patients diagnosed with narcolepsy after 2009 were included and data were collected for 7 years to account for any possible delays in the diagnosis of narcolepsy.
Results: One-hundred and seventy-three patients with narcolepsy were identified. The majority (144 patients, 83%) had symptom onset before June 2009. Only 29 patients (17%) had symptom onset after 2009. No difference in the annual number of narcolepsy cases was found before and after 2009.
Conclusion: Based on data obtained from 2 tertiary care sleep disorders center, there was no increase in the number of cases of narcolepsy among Saudis following the introduction of the influenza A(H1N1)pdm09 vaccination.
Narcolepsy is a chronic disabling sleep disorder characterized by excessive daytime sleepiness with or without cataplexy. Other less consistent symptoms include hypnagogic/hypnopompic hallucinations, sleep interruptions, and sleep paralysis.1 The prevalence of narcolepsy has been reported to be between 25 and 50 per 100,000 individuals, with an incidence of 0.74 per 100,000 person-years.2 A prevalence of 40/100,000 has been reported in Saudi Arabia.3,4 The causes of narcolepsy are still unknown. Nevertheless, both genetic and environmental factors have been proposed to be involved in the etiology of narcolepsy. Recently, there has been increasing evidence supporting an autoimmune process in the development of narcolepsy.5 This theory has gained more strength following the introduction of the H1N1 pandemic vaccine in June 2009. The H1N1 ASO3-adjuvanted pandemic vaccine (Pandemrix™) was the main H1N1 vaccine used in the European Union.5,6 In August 2010, Finland and Sweden raised concerns regarding a possible association between narcolepsy and Pandemrix™.7,8 A cohort study in Finland reported a 13-fold increase in the risk of narcolepsy following Pandemrix™ vaccination in children aged 4 to 19 years.8,9 This was subsequently confirmed by further studies in England, Ireland, and Norway.10-12 Although the initial association was reported in children, adult cases have been reported subsequently.5,13 In contrast to the above studies, reports from the United States, Italy, Canada, and South Korea found no indication of any association between H1N1 vaccination and narcolepsy.9,14-17
No data from the Middle East regarding the association between H1N1 vaccination and narcolepsy following the H1N1 pandemic have been reported. The Ministry of Health in Saudi Arabia organized a campaign to administer the (H1N1)pdm09 vaccine to the public and school children throughout the country in November 2009.18 All Saudis without exception had free access to the pandemic influenza A(H1N1) vaccine. However, the vaccination was not compulsory. Although Saudi Arabia does not have national vaccination records, a report on 2009 indicated that GlaxoSmithKline vaccine (Pandemrix™) was Saudi Arabia’s sole supplier of a vaccine for the H1N1 flu virus,19 which is the H1N1 ASO3-adjuvanted pandemic vaccine.
Based on our experience in our practice and communications with our colleagues in other sleep disorders centers in Saudi Arabia, we hypothesized that the introduction of H1N1 vaccine did not lead to any increase in the number of narcolepsy cases among Saudi patients. Therefore, we designed this study to assess the number of Saudi patients diagnosed with narcolepsy in 2 tertiary centers before and after the introduction of the A(H1N1)pdm09 vaccine.
Methods
Data were collected from 2 tertiary sleep disorders centers: the University Sleep Disorders Center (USDC) at King Saud University, and the Pediatrics Sleep Disorders Center (PSDC) at the Prince Sultan Military Medical City in Riyadh, Saudi Arabia. The USDC is a tertiary care center that accepts referrals of all age groups from all over the country with immediate access to all Saudi patients with suspected narcolepsy. The PSDC accepts all cases with sleep disorders in the pediatric age group from all military health care services across the country. The ethics committee at the College of Medicine, King Saud University approved the study and informed consent was obtained for all participants.
We started collecting data after the first international report of (2010) an association between the (H1N1)pdm09 vaccine and narcolepsy.20 We included all patients diagnosed with narcolepsy after 2009 (from January 2010 until the end of December 2016), and we collected data for 7 years to account for any possible delay in the diagnosis of narcolepsy, its presentation or access to specialized medical services, as a previous study showed that there is a delay of 7 tot 8 years between symptom onset and diagnosis in Saudi patients with narcolepsy.4,21 We used data from the databases of the participating centers beginning 7 years before 2009 until the time of the study conclusion (from January 2002 to end of December 2016) to compare the numbers of annual cases with new onset of narcolepsy symptoms after 2009 to those before and during 2009. None of the included patients had psychiatric or chronic medical illnesses. Exclusion criteria included patients who did not meet the International Classifications of Sleep Disorders Diagnostic (ICSD-2).22
Narcolepsy diagnosis
Narcolepsy was diagnosed based on the ICSD-2.22 The diagnosis of narcolepsy for each included patient was rechecked and verified by a sleep medicine specialist after full polysomnography followed by a multiple sleep latency test (MSLT) in accordance with the ICSD-2.22 Data from patients with narcolepsy diagnosed after September 2009 were analyzed to establish symptom onset details, whether the H1N1 vaccine was received, the time interval between the date of vaccination and the date of symptom onset, the date of diagnosis, clinical history, and sleep study results.
The earliest date of onset of excessive daytime sleepiness or cataplexy, as reported by the patient and recorded in his/her file, was used to define the date of symptom onset. The date of diagnosis was the date on which clinical assessment and sleep studies confirming narcolepsy were performed.
Statistical analysis
Numerical data were expressed as mean ± standard deviation, and categorical data as percentages. The comparison of categorical variables between groups was performed using the Chi-square test. The comparison of continuous variables was performed using Student’s t-test or Mann-Whitney U test if normality theory was violated. The data were analyzed using the Statistical Package for Social Sciences (SPSS), IBM version 22 (SPSS Inc., Chicago, IL, USA) software.
Results
Study cases
One-hundred and seventy-three patients with narcolepsy were identified in the databases. The majority of the patients (n=144, 83%) had symptom onset before June 2009. Only 29 patients (17%), had symptom onset after 2009.
Table 1 presents a comparison between patients with narcolepsy diagnosed before 2009 and diagnosed after 2009. There was no difference in the percentage of patients with cataplexy before versus after 2009 (92% versus 90%). Moreover, the age of symptom onset was similar in the 2 groups (19.1±8.9 versus 17.4±8.2, p=0.34).
Comparison between patients with narcolepsy diagnosed before and after 2009.
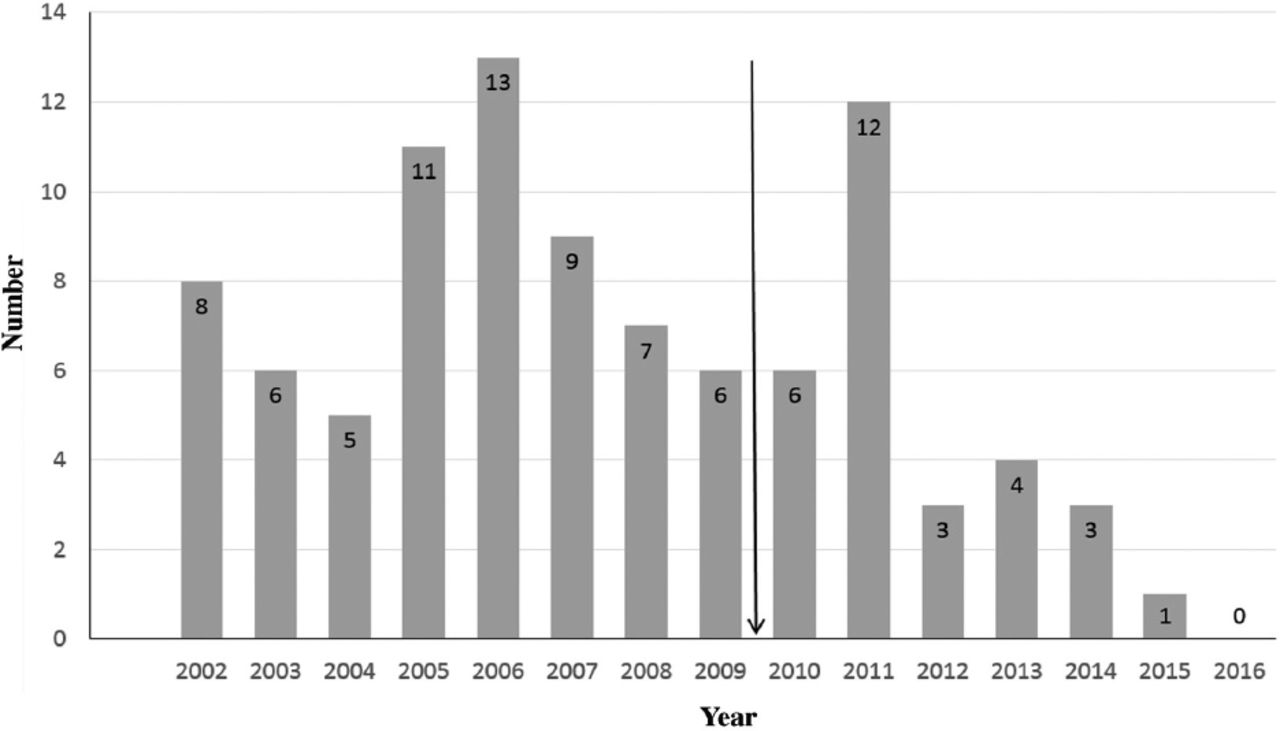
Figure 1 shows the annual number of patients who developed narcolepsy (based on symptom onset) in the years 2002 through 2016 (n=94). Although there was an increase in the number of patients who developed symptoms on 2011, none of them has received the H1N1 vaccine on 2009.

The annual number of patients who developed narcolepsy from 2002 to 2016.
Discussion
It has been postulated that both upper respiratory tract infections and vaccinations may trigger narcolepsy through autoimmune processes which could result in the loss of hypothalamic hypocretin/orexin-producing neurons.23 Although vaccination is an important public health strategy during influenza pandemics, many concerns have been raised regarding its safety following reports associating 2009 H1N1 vaccination with narcolepsy.
In this report, we started collecting data after the first report of an association between the H1N1 vaccine and narcolepsy.20 We observed no increase in the number of diagnosed cases of narcolepsy in children and adults during the H1N1 pandemic strain vaccine campaign in 2 major sleep disorders centers in Saudi Arabia.
Our findings are consistent with reports from South Korea, where the investigators found no increase in the number of cases or the incidence rate of narcolepsy after the A(H1N1)pdm09 vaccination campaign with the use of MF59-adjuvanted or non-adjuvanted A(H1N1)pdm09 vaccine.14 Similar results were reported in another study from the United States which also found that Influenza vaccines containing the A(H1N1)pdm09 virus strain are not associated with an increase in the risk of narcolepsy.15
One possibility to explain this lack of association between H1N1 vaccination and narcolepsy in the current study may involve unidentified factors, such as genetic susceptibility, in countries with an increased incidence of narcolepsy after the use of the H1N1 vaccine.24 It is also possible that previous studies with negative results did not evaluate and follow up the effects of the vaccine long enough, as there is usually a delay between the onset of symptoms and the actual diagnosis. To account for a possible delay in symptom onset or a delay in the diagnosis of narcolepsy, we investigated possible associations between H1N1 vaccination and narcolepsy 7 years after initiating the H1N1 vaccine campaign.
The strengths of this study include the fact that we collected data prospectively beginning at the time of the first report linking H1N1 vaccination to narcolepsy. Moreover, we collected our data over 7 years to account for any delays in presentation or referral.
Study limitations
Although both participating sleep disorders centers accept patients from all over the country, our results cannot be extrapolated to the whole country, as there is no national registry for narcolepsy in Saudi Arabia. Additionally, the percentage of the population that was vaccinated is not known. As there is no national vaccine registry, individuals who received vaccine could not be identified and monitored for possible development of narcolepsy. Third, it is possible that there are undiagnosed cases of narcolepsy that may have received the vaccine but have not presented to the sleep disorders centers participating in this study. Additionally, as vaccination coverage in Saudi Arabia is unknown, low vaccination coverage could explain the missing increase on incident narcolepsy cases. As there is no national health registry that includes vaccination type and history, it was not possible to have a proper and accurate assessment of the rates of narcolepsy before and after 2009. Finally, variation in the referral patterns over time is a possibility that cannot be excluded.
Although our data cannot be generalized to Saudi Arabia, we believe that our results indicate lack of association between H1N1 vaccination in 2 tertiary care sleep disorders centers in Saudi Arabia. Moreover, our observations in Saudi Arabia may provide baseline data that may be used to investigate the association between H1N1 vaccination and the development of narcolepsy in the region. Future studies should adopt a case-control design to accurately assess the association between the vaccine and narcolepsy.
In conclusion, based on data obtained from 2 tertiary care sleep disorders centers, there was no increase in the annual number of cases of narcolepsy among Saudis during the influenza A(H1N1)pdm09 vaccination period and the years that followed. As there is no national health registry, the results cannot be generalized to the whole country. Nevertheless, this report should encourage other sleep medicine specialists in Saudi Arabia and the region to collectively report data related to H1N1 vaccine and narcolepsy.
Clinical Practice Guidelines
Clinical Practice Guidelines must include a short abstract. There should be an Introduction section addressing the objective in producing the guideline, what the guideline is about and who will benefit from the guideline. It should describe the population, conditions, health care setting and clinical management/diagnostic test. Authors should adequately describe the methods used to collect and analyze evidence, recommendations and validation. If it is adapted, authors should include the source, how, and why it is adapted? The guidelines should include not more than 50 references, 2-4 illustrations/tables, and an algorithm.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. Dr. Ali M. Albarrak and Dr. Adel S. Alharbi are members of the Editorial Team, and were therefore excluded from any final editorial decisions regarding this paper. This study was supported by a grant from the Strategic Technologies Program of the National Plan for Sciences and Technology and Innovation in the Kingdom of Saudi Arabia (08-MED511-02).
- Received August 9, 2017.
- Accepted October 22, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.