


Abstract
Objectives: To determine whether perioperative fluid restrictive administration can reduce specific postoperative complications in adults undergoing major abdominal surgery.
Methods: We searched the MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials, Google scholar, and article reference lists (up to December 2015) for studies that assessed fluid therapy and morbidity or mortality in patients undergoing major abdominal surgeries. The quality of the trials was assessed using the Jadad scoring system, and a meta-analysis of the included randomized, controlled trials was conducted using Review Manager software, version 5.2.
Results: Ten studies with a total of 1160 patients undergoing major abdominal surgeries were included. We found that perioperative restrictive fluid therapy could reduce the risk of postoperative infectious complications (odds ratio [OR]=0.54, 95% confidence interval [CI]:0.39-0.74, p=0.0001, I2=37%), pulmonary complications (OR=0.49, 95% CI: 0.26-0.93, p=0.03, I2=50%), and cardiac complications (OR=0.45, 95% CI: 0.29-0.69, p=0.0003, I2=48%), but had no effect on the risk of gastrointestinal complications (OR=0.87, 95% CI: 0.51-1.46, p=0.59, I2=0%), renal complications (OR=0.76, 95% CI: 0.43-1.34, p=0.35, I2=0%), and postoperative mortality (OR=0.62, 95% CI: 0.25-1.50, p=0.29, I2=0%).
Conclusion: Perioperative restrictive fluid administration was superior to liberal fluid administration in reducing the infectious, pulmonary and cardiac complications after major abdominal surgeries.
The goal of perioperative fluid administration is to maintain optimal oxygen supply and tissue perfusion, but the optimal amount of fluid to be administered is still in question. Hypovolemia can cause organ hypoperfusion, systemic inflammatory response syndrome, sepsis, and multiple organ failure, while hypervolemia can cause edema, illeus, pulmonary and cardiac complications.1,2 According to the textbook, Miller’s Anesthesia, the perioperative liberal fluid therapy includes the replacements for the following components: the intravascular expansion caused by anesthesia, deficits from preoperative fasting, physiological maintenance, redistribution in the third space, and blood loss.3 Currently, the conception of the third space has been questioned by an increasing number of anesthesiologists, and whether it should be replaced intraoperatively is controversial. It has been shown that endothelial glycocalyx plays a key role in maintaining the endothelial integrity, and fluid overload from liberal fluid administration may precipitate the excretion of atrial natriuretic peptide (ANP), which can damage the endothelial integrity, and cause platelet aggregation, vascular permeability, and tissue edema as a result.4,5 Rahbari et al6 defined the terminology of liberal fluid therapy and restrictive fluid therapy in the meta-analysis, and the results showed that perioperative fluid restriction could decrease postoperative morbidity. But whether fluid restriction can reduce specific complications (such as, infective, pulmonary, cardiac, gastrointestinal and renal complications) after major abdominal surgery is still unclear, and new randomized, controlled clinical trials (RCTs) have been published in recent years. Therefore, a meta-analysis needs to be performed to determine whether perioperative fluid restrictive administration can reduce specific postoperative complications in adults undergoing major abdominal surgery.
Methods
Our systematic review and meta-analysis were conducted in accordance with the methods recommended by the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines.7 There was no registered protocol.
Liberal fluid administration was defined according to Miller’s Anesthesia,3 as mentioned previously. According to recent clinical trials, restrictive fluid administration generally consists of partial or no replacement for the intravascular expansion from anesthesia, in which case vasopressors are usually administered, no replacement for the third space loss, and only partial replacement for deficits from preoperative fasting. The replacements for physiological maintenance and blood loss were similar for both restrictive fluid strategy and the liberal fluid strategy.8,9
Literature search
MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, and Google scholar were searched up to December 2015, and the references of RCTs and published meta-analysis papers were checked for additional potential eligible trials. To reduce publication bias, the abstracts were searched in the databases without any language restrictions. The key words included abdominal surgery, colon resection, rectum resection, gastric resection, pancreas resection, pancreaticoduodenectomy, hemicolectomy, esophagectomy (abdominal route), and abdominal aortic aneurysm repair, fluid administration, restrictive fluid, liberal fluid, standard fluid, and conventional fluid. The inclusion criteria were defined as follows: RCTs, the comparison of liberal fluid administration and restrictive fluid administration, and major abdominal surgery. The exclusion criteria were defined as follows: only postoperative restrictive fluid therapy and liberal fluid therapy were compared, patients were younger than 18 years old, the participants included patients with critical illness or sepsis, or organ dysfunction established preoperatively.
Data collection and outcome parameters
Two authors independently conducted the search and screened the literature. To avoid translation and transcription bias, the data were rechecked by another reviewer. When any disagreement regarding the data occurred, all of the reviewers discussed and resolved it.
The primary outcomes included postoperative infectious complications, pulmonary complications, cardiac complications, and gastrointestinal complications. The secondary outcomes were postoperative renal complications and mortality (death in hospital from any cause after surgery).
Statistical analysis
The meta-analysis was performed using Review Manager version 5.2 for Windows (the Cochrane Collaboration, Oxford, UK). The calculations of effect size for dichotomous data were odds ratio (OR) with 95% confidence interval (CI). Statistical heterogeneity was assessed using I2 statistics,10 the levels of heterogeneity was defined as low when I2 levels are ≤25%, moderate when I2 levels range between 25-50%, or high levels when I2 levels are >50%. The fixed-effect model was used when I2<50%, and the random-effect model was used when I2≥50%.
The risk of bias was checked by appraising “adequate sequence generation”, “allocation concealment”, “blinding”, “incomplete outcome data addressed”, “free of selective reporting”, and “free of other bias”, as recommended by the Cochrane Collaboration. Publication bias was evaluated with funnel plot analysis, in which the OR is plotted against the standard error. Furthermore, Egger test was utilized to assess the funnel plot for significant asymmetry. There was no statistical publication bias if p>0.05 in Egger test.
The quality of the trials was assessed using the Jadad scoring system. The evaluated items included size calculation, generation of allocation sequence, allocation concealment, methods of randomization, blinding, and descriptions of protocol deviations, withdrawals, and dropouts.11 The trials with a quality score less than 3 were excluded.
Results
Characteristics of eligible trials
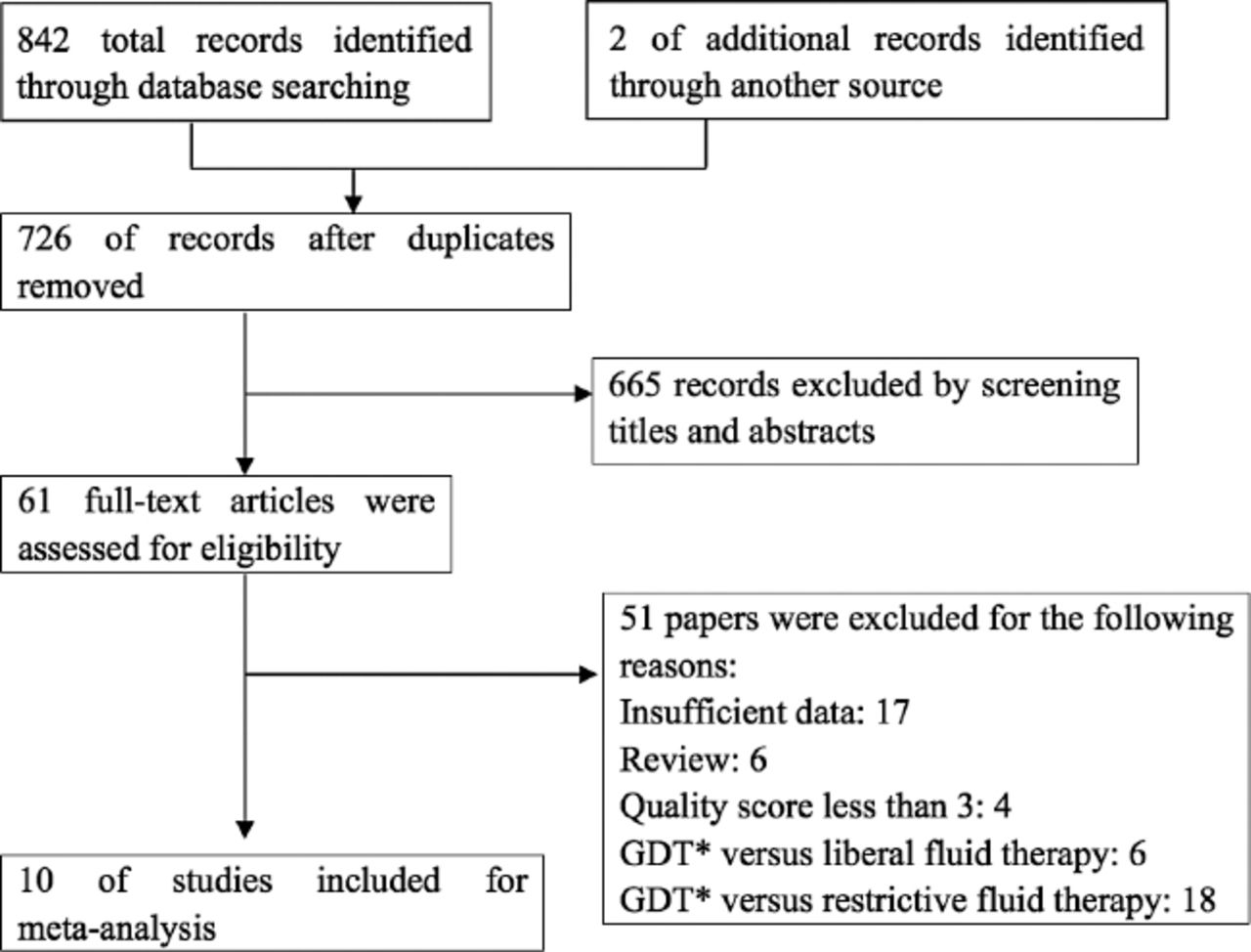
We identified 844 potential articles through the key words, 376 articles from MEDILINE, 410 articles from the Cochrane Library, 56 articles from EMBASE, and 2 articles from other sources. Seven hundred twenty-six papers remained after duplicates were removed, and 61 potentially relevant articles remained after an initial screening and reading the titles and abstracts. After a more detailed selection process, we excluded 24 trials investigating goal-directed fluid therapy versus liberal or restrictive fluid therapy, 17 trials with insufficient data, 6 reviews, and 4 trials with quality scores less than 3. Finally, 10 RCTs12-21 with a total of 1160 patients were included. The details of the eligibility process are presented in Figure 1.
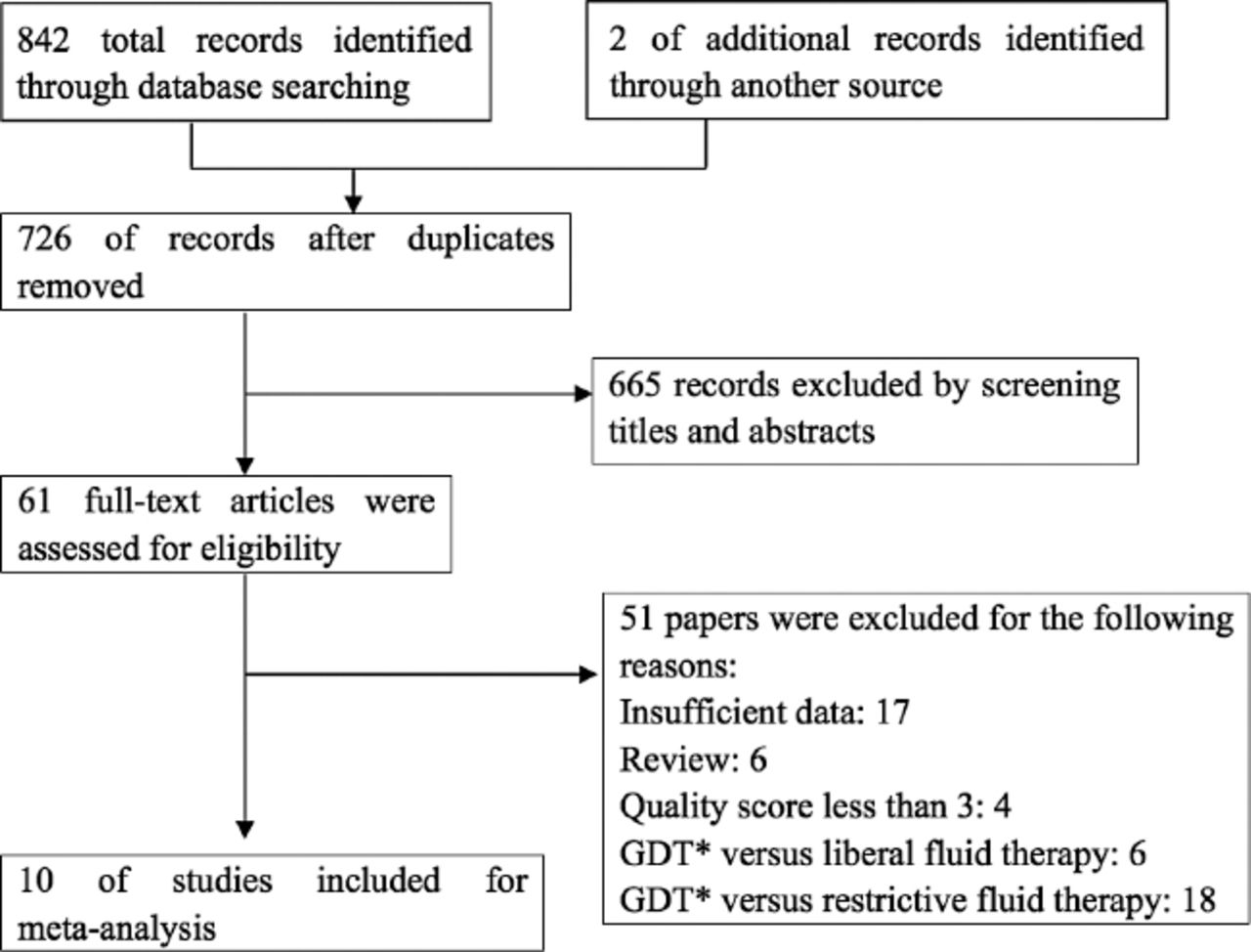
Flow chart summarizing the procedure of studies selection for the meta-analysis. GDT - goal-directed fluid therapy
These 10 trials were conducted in different countries (China, UK, Sweden, Northern Ireland, Brazil, Denmark, Belgium, Bosnia and Herzegovina), and were published from 2003 to 2015. The surgeries were all elective abdominal surgeries, including oesophagectomy, gastric resection, colon resection, rectum resection, hemicolectomy, pancreatoduodenectomy, and abdominal aortic aneurysm repair. The characteristics of the trials are presented in Table 1 A & 1 B.
Basic features of the included trials for postoperative complications analysis.
Continuation of basic features of the included trials for postoperative complications analysis.
Methodological quality of studies
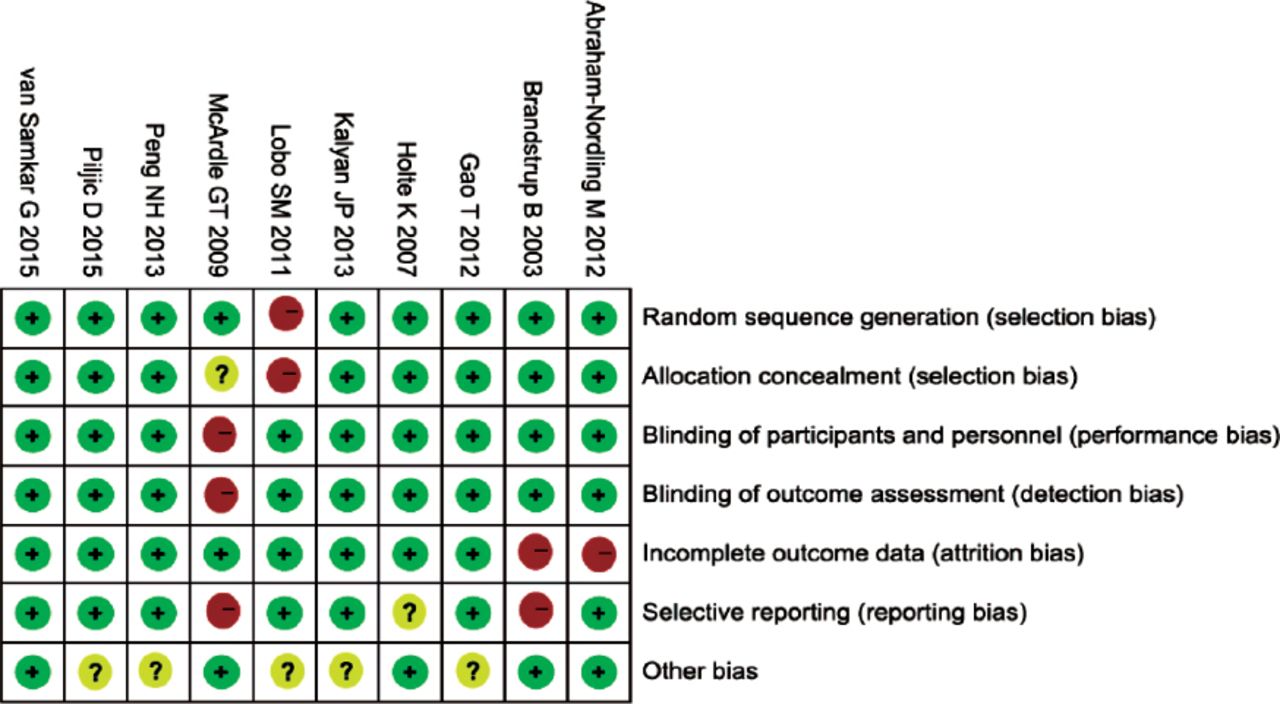
The quality of the trials was assessed using the Jadad score, and the results are presented in Table 1 A & 1 B. The quality scores was 5 in 5 trials,15,17,19-21 4 for 2 trials,12,16 and 3 for the other 3 trials.13,14,18 The risk of bias summary is shown in Figure 2. The Cohen κ statistic for agreement regarding study inclusion was 0.857.
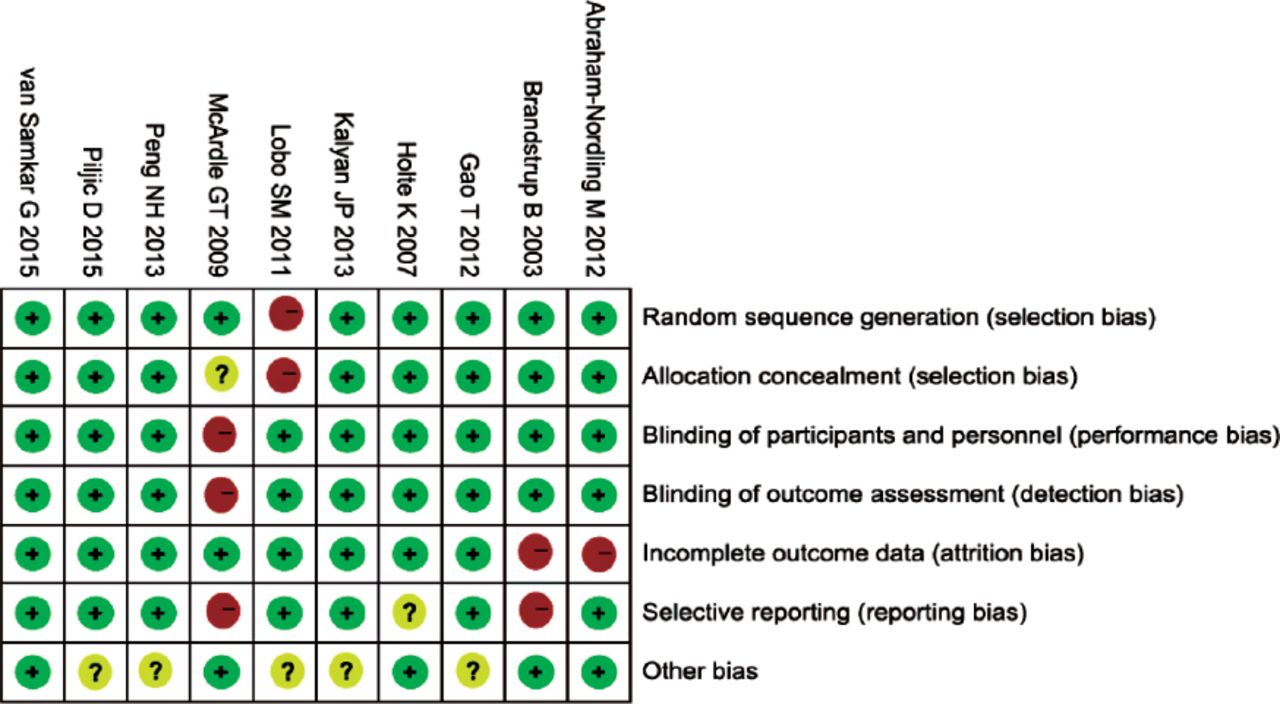
Risk of bias summary. Green indicates a low risk of bias, red indicates a high risk of bias, and yellow indicates an unclear risk of bias.
Results of the meta-analysis
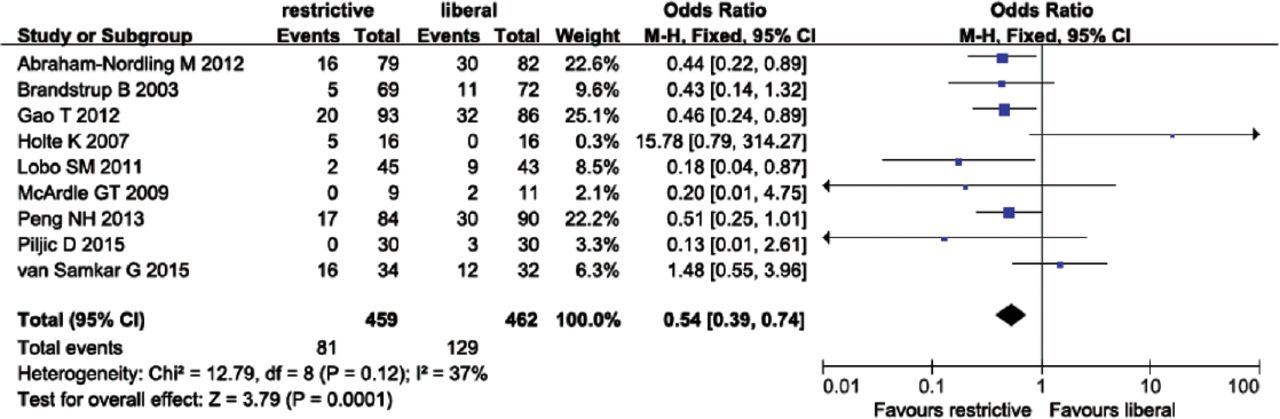
1) Data on postoperative infectious complications were from 9 trials of all, and the sample size was 921. Postoperative infectious complications included anastomotic leakage, wound dehiscence, wound infection, peritonitis, sepsis, and urinary tract infection. The fixed-effects model showed a significant reduction of postoperative infectious complications in restrictive fluid administration (OR=0.54, 95% CI: 0.39-0.74, p=0.0001, I2=37%) (Figure 3). There was no significant publication bias according to Egger test (p=0.129).

Forest plot of postoperative infectious complications comparing restrictive and liberal fluid administration.
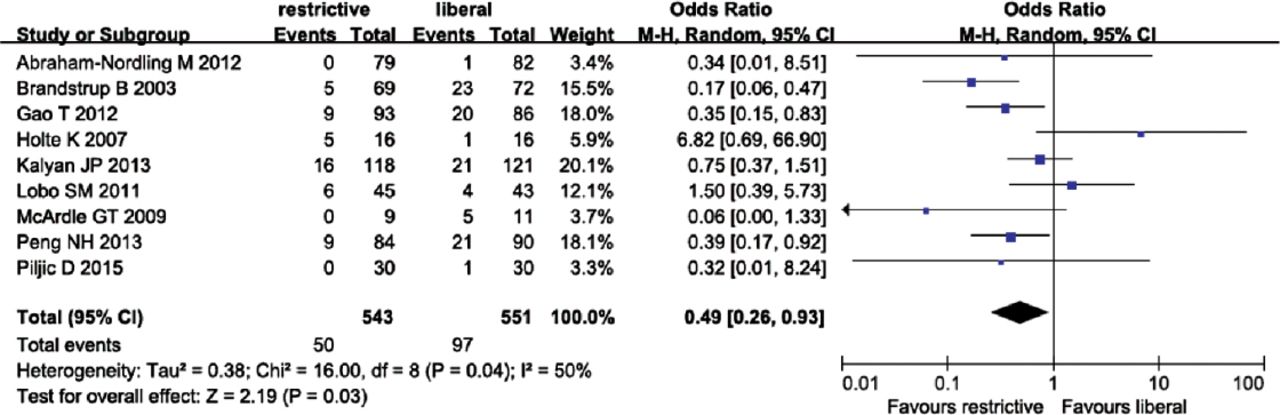
2) Data with respect to postoperative pulmonary complications were from 9 trials of all, and the sample size was of 1094. The random-effects model showed a significant reduction of postoperative pulmonary complications in restrictive fluid administration (OR=0.49, 95% CI: 0.26-0.93, p=0.03, I2=50%)(Figure 4), there was no significant publication bias according to Egger test (p=0.348).

Forest plot of postoperative pulmonary complications comparing restrictive and liberal fluid administration.
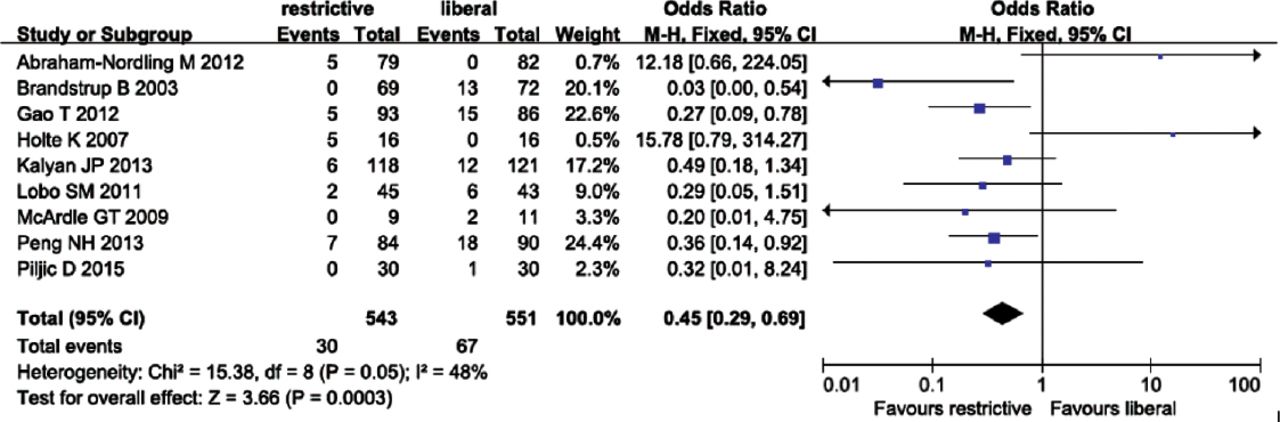
3) Nine trials (1094 patients) reported postoperative cardiac complications, which included arrhythmias, heart failure, and myocardial infarction. The fixed-effects model showed a significant reduction of postoperative cardiac complications in restrictive fluid group (OR=0.45, 95% CI: 0.29-0.69, p=0.0003, I2=48%) (Figure 5). There was no significant publication bias according to Egger test (p=0.775).
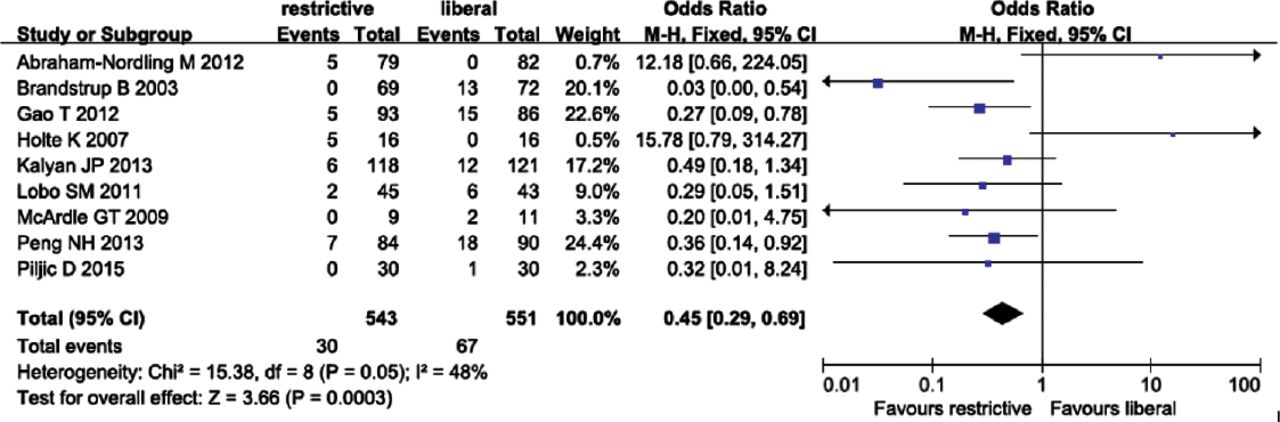
Forest plot of postoperative cardiac complications comparing restrictive and liberal fluid administration.
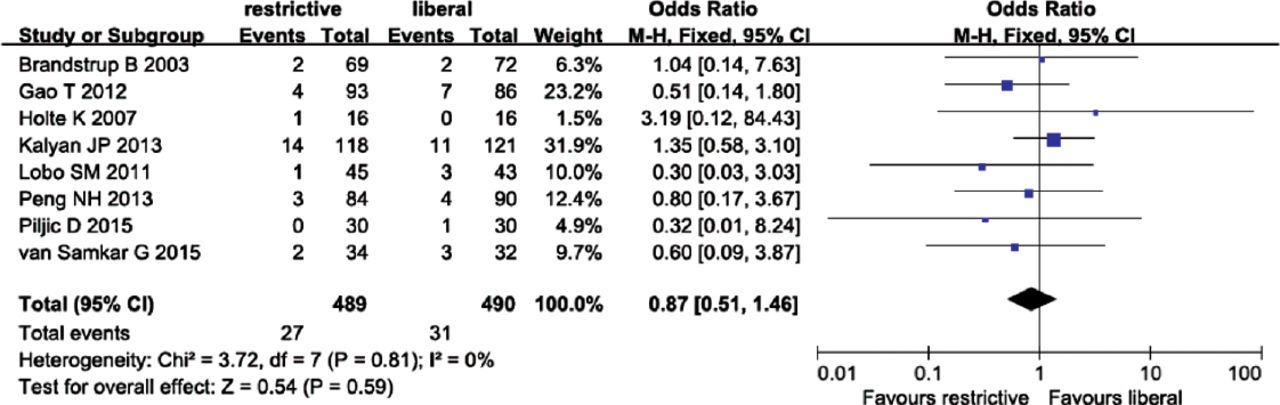
4) Eight of the 10 trials reported postoperative gastrointestinal complications, which included intestinal obstruction, bowel obstruction, and bleeding, the sample size was of 979. The fixed-effects model showed no reduction in restrictive fluid administration (OR=0.87, 95% CI: 0.51-1.46, p=0.59, I2=0%) (Figure 6). There was no significant publication bias according to Egger test (p=0.139).

Forest plot of postoperative gastrointestinal complications comparing restrictive and liberal fluid administration.
5) All 10 trials (1160 patients) reported postoperative renal complications. The fixed-effects model showed no difference between restrictive and liberal fluid administration (OR=0.76, 95% CI: 0.43-1.34, p=0.35, I2=0%). There was no significant publication bias according to Egger test (p=0.263).
6) Data on postoperative mortality were from 8 of the 10 trials, and 954 patients were included. The fixed-effects model showed no differences in postoperative mortality between restrictive and liberal strategy (OR=0.62, 95%CI: 0.25-1.50, p=0.29, I2=0%). Egger test revealed no significant publication bias (p=0.451).
Discussion
Ten clinical randomized controlled trials were included in our meta-analysis, intraoperative fluid restriction plus postoperative fluid restriction or intraoperative fluid restriction alone was used in these trials, the trials on postoperative fluid restriction alone were not included in our meta-analysis, because intraoperative fluid restriction was a requisite strategy. In most of the RCTs in our meta-analysis, the amount of postoperative fluid therapy was not shown. Rahbari et al6 reported in his meta-analysis that fluid restriction could reduce overall morbidity in colorectal surgery, but did not specify the postoperative complications, such as infectious, pulmonary, or cardiac complications, that were analyzed in our meta-analysis.
Boland et al8 conducted a meta-analysis of perioperative fluid restriction in major abdominal surgeries that included a much wider range of surgeries, than was described in the meta-analysis of Rahbari et al.6 The results showed that fluid restriction intraoperatively, postoperatively, or both, could not reduce overall postoperative complications. The specific postoperative morbidities were not presented.
Our meta-analysis suggested that perioperative restrictive fluid administration could reduce postoperative infectious, pulmonary and cardiac complications compared with perioperative liberal fluid administration, but there were no differences in other complications between the 2 strategies. Among the RCTs that were included in our meta-analysis, the length of hospital stay was expressed as medians (interquatile ranges) in 3 of the 10 trials,12,14,17,18,20 and as averages in other 2 trials.13,19 Consequently, the length of hospital stay could not be analyzed, but there were no significant differences between restrictive and liberal groups in all but 2 of these trials.13,19 Perioperative fluid restriction reduced the postoperative infectious, pulmonary and cardiac complications, this may be attributed to the endothelial glycocalyx, which plays a key role in maintaining the integrity and preventing the permeability of blood vessels.4 Liberal fluid therapy may induce fluid overload, which can lead to high levels of ANP excretion,5 and subsequent damage to endothelial glycocalyx. As a result, the permeability of the vessels eventually increased, and infectious pulmonary and cardiac complications can occur postoperatively. While restrictive fluid therapy can protect endothelial glycocalyx and reduce the complications, it should be considered in major abdominal surgeries.
In recent years, the safety of perioperative fluid restriction has been questioned by many clinicians. The main concern is that it has the potential to cause hypovolemia and postoperative organ dysfunction, of which acute kidney injury is the most concern.9 In our meta-analysis, there were no differences in postoperative renal complications and mortality between restrictive and liberal fluid therapy, nor were there differences in postoperative gastrointestinal complications. Gastrointestinal complications can be induced by gut hypoperfusion,22 too much or too little perioperative fluid administration is detrimental to gastrointestinal function. A recent study showed that goal-directed fluid therapy (GDT) is effective to reduce gastrointestinal complications.23 The criteria of fluid restriction varied among the RCTs, and the fluid amount also varied considerably among the 10 RCTs in our meta-analysis. This variation may explain why fluid restriction could not reduce gastrointestinal complications. The results of our meta-analysis suggest that perioperative fluid restriction is a safe strategy; it reduced postoperative infectious, pulmonary and cardiac complications, and was not harmful to other organs. Of the 10 RCTs included in our meta-analysis, the study by Holte et al12 was the only one that favoured liberal fluid therapy for avoiding infectious pulmonary and cardiac complications, our meta-analysis reached the opposite conclusion. In the study by Holte et al,12 the sample size was very small, and the type of surgery was fast-track colonic surgery, therefore, it is necessary to investigate the effect of restrictive and liberal fluid therapy on postoperative complications in fast-track colonic surgery with a large sample size. Since these clinical trials involved different types of surgery, further studies with large sample size should be conducted in the future to explore the safety of restrictive fluid therapy in specified types of abdominal surgery.
There are some limitations about our meta-analysis. First, it included a wide range of major abdominal surgeries. Second, the patients received different volumes of fluid therapy before surgery in each of the 10 trials in our meta-analysis. Third, the sample size was not large enough, and the clinical heterogeneity among these studies cannot be ignored. Different therapeutic methods including anesthetics, purgative bowel preparation, epidural anesthesia or analgesia, volume preloading before epidural block and intraoperative or postoperative fluid administration may have effects on the results.
In conclusion, our meta-analysis found that perioperative fluid restrictive administration could reduce postoperative infectious, pulmonary and cardiac complications in major abdominal surgeries, but had no effect on gastrointestinal, renal complications and postoperative mortality. Therefore, perioperative restrictive fluid therapy should be considered in major abdominal surgery.
Authorship entitlement
Excerpts from the Uniform Requirements for Manuscripts Submitted to Biomedical Journals updated November 2003.
Available from www.icmje.org
The international Committee of Medical Journal Editors has recommended the following criteria for authorship; these criteria are still appropriate for those journals that distinguish authors from other contributors.
Authorship credit should be based on 1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) intellectual content; and 3) final approval of the version to be published. Authors should meet conditions 1, 2, and 3.
Acquisition of funding, collection of data, or general supervision of the research group, alone, does not justify authorship.
An author should be prepared to explain the order in which authors are listed.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. This project was supported by Chongqing Municipal Health and Family Planning Commission, Chongqing, China. Grant No. 2011-2-364.
- Received March 17, 2016.
- Accepted September 22, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}