


Abstract
Objectives: To embrace a national screening program for prostate cancer, putting into consideration the cost, and the attitude of the general population towards such screening.
Methods: Men aged >45 and <70 years were invited to participate in the current prospective study conducted at King Saud University Medical City, Riyadh, Saudi Arabia between December 2014 and July 2015. Those with confirmed high prostate-specific antigen (PSA) (≥4 ng/ml) were referred to the urology clinic, then subjected to magnetic resonance imaging.
Results: The total cohort screened were 2898, we found 118 cases with high PSA (≥4 ng/ml). Fifty-two cases (60.4%) were confirmed high PSA. All of them were subjected to MRI and biopsy. The confirmed prostate cancer were 7 cases (0.24%). The age of confirmed prostate cancer cases ranged from 49 years to 68 years, Gleason score for 4 cases was low grade (3+3), while it was 3+4 for 2 cases, and only one case had advanced cancer (3+5). Approximately 12% of cases with high PSA did not show up for confirmation of their results for further examination.
Conclusions: The present study recommends against mass screening among Saudi population; however, men before 50 years of age should start PSA blood testing until before 70 years after discussing the benefits and harms of such screening through shared decision making.
The cost-effectiveness of certain diseases, particularly cancer could be achieved in a selected community if it is applied appropriately and conveniently.1 So far we do not have a sufficient evidence whether screening of prostate cancer reduces mortality. However, screening tests with prostate-specific antigen (PSA) or digital rectal examination (DRE) are capable of detecting prostate cancer in early stages, but there is no certainty that such early detection and treatment can lead to any change in the outcome of the disease.2 Two randomized trials show that there is no effect on mortality through 7 years, but the results are inconsistent beyond 7-10 years.2 Screening with PSA and/or DRE could result in the over diagnosis of prostate cancer and subsequently lead to over treatment. As screening, also could lead to false-positive results, which in turn leads to unnecessary diagnostic procedures. In addition, to adverse psychological effects in men who have a prostate biopsy, but do not have identified prostate cancer.2-5 On the other hand, not having this test can mean missing an early prostate cancer detection, and ultimately losing your life.4
In Saudi Arabia, the incidence of prostate cancer is very low in comparison to other European and even Gulf countries. According to Globocan, 2012 data, prostate cancer incidence in the Middle East Arab nations is expected to increase from 29,377 prostate cancer new cases in 2012 to 38,562 new cases in 2020 along with an increase in mortality from 15,422 deaths in 2012 to 19,681 deaths in 2020.6
The age-standardized incidence rate (ASIR) was 4.5/100,000 in 2012, the 2 regions with the highest ASR were the Eastern region and the Riyadh region. The highest ASIR of prostate cancer in the world (126.3/100,000) was reported from Ireland, which is 16-fold higher than Saudi Arabia. Yet, the pattern and trend of prostate cancer should be reported and not neglected due to low ASIR.7
The only screening program which is adopted in our region is the screening for breast cancer. With the increasing incidence of prostate cancer in the last years in our region, the current study sought if to embrace a national screening program for prostate cancer, putting into consideration the cost and the attitude of the general population towards such screening?
Methods
The current prospective study was conducted in King Saud University, Riyadh, Saudi Arabia outpatient clinic laboratory services between December 2014 and July 2015. Male >45 and <70 years old who were transferred for blood withdrawal from the primary care clinics for any reason were included in the study. They were informed about the purpose of the study and informed consent was taken before the study. Those who accepted to participate were asked to complete a concise questionnaire regarding their current and past disease history, smoking status, any prostate disease. Cases with a history of prostate cancer or any condition that might affect PSA levels such as coagulopathies and sepsis were excluded from the study.
An extra 4 ml was withdrawn from each subject for PSA analysis; and sera were isolated. The sera, centrifuged at 2000 G and kept at -20°C in a deep freezer until analyzed were processed for the total prostate-specific antigen (T-PSA) levels by the T-PSA kit using the Biomerieux Vidas PC Automated Immunoassay Analyzer, BioMerieux, France.
Any subject with high PSA (≥4 ng/ml) was contacted and encouraged to come again for the PSA retesting and confirmation of the result. Those with confirmed high PSA were referred to the urology clinic and then subjected to MRI. Patients with Py-rad >2 were subjected to MRI guided biopsy. Positive cases were managed accordingly, while negative cases were advised to follow-up with PSA testing.
The fieldwork was conducted after obtaining the approval from the Ethics Committee of the Faculty of Medicine, King Saud University, Riyadh, Saudi Arabia. All persons gave their informed consent prior to their inclusion in the study.
Results
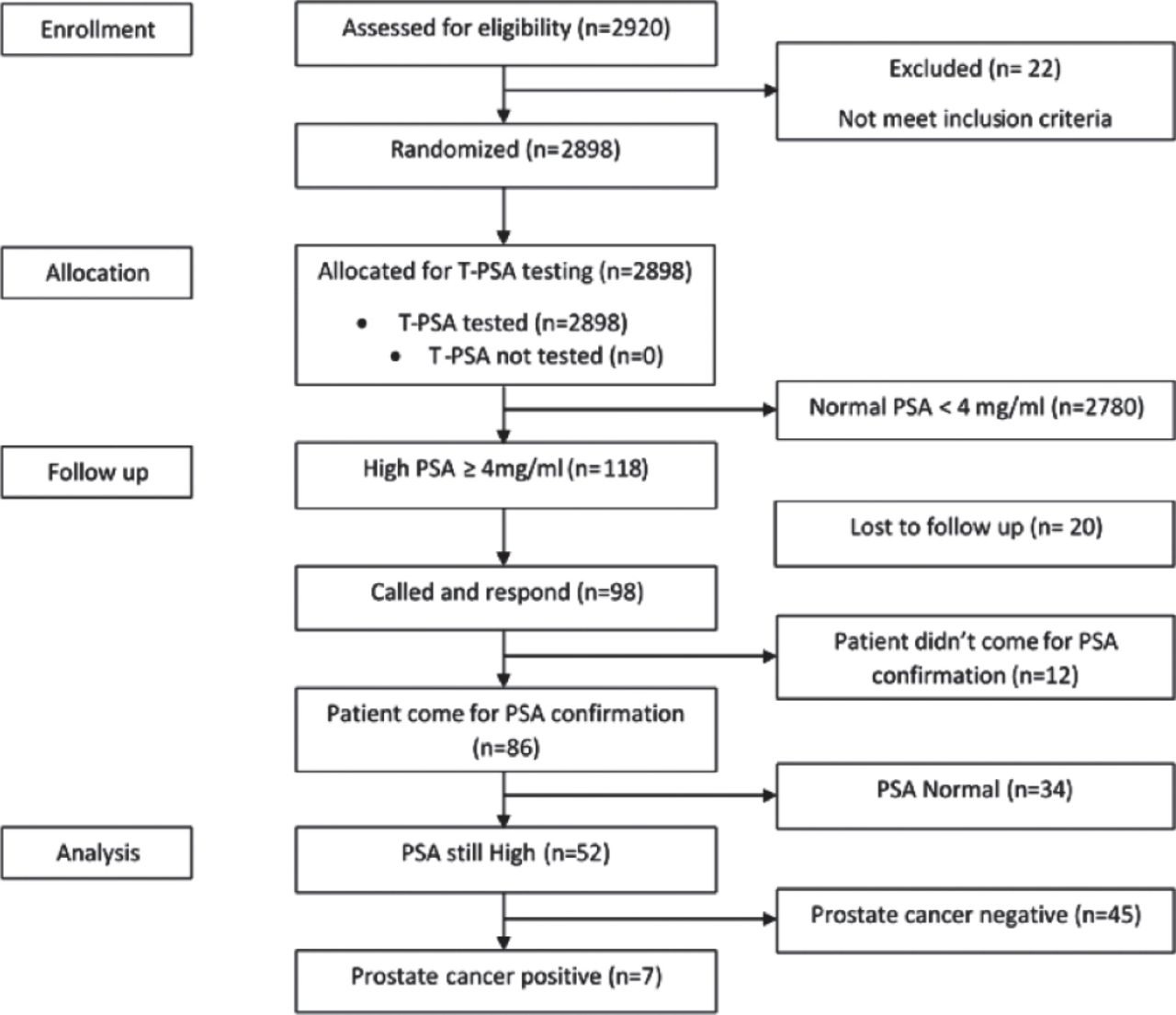
The total number of screened subjects was 2920, mean age was 56.61±6.74 years. Twenty-two subjects with a history of prostate cancer cases were excluded. The remaining 2898 subjects who met the inclusion criteria comprised our cohort. One hundred and eighteen cases were found to have a high PSA (≥4 ng/ml). All of them were contacted for reconfirmation of the PSA result where 20 cases (17%) were lost to follow-up. Of the 98 cases, 86 (87.7%) responded. Twelve cases (12.2%) did not show up for PSA retesting and confirmation of their results, even after they were contacted; and the team explained to them how much this finding is important and critical to them. Reconfirmation of PSA revealed 52 cases (60.4%) with high PSA. All of them were subject to MRI and biopsy. The confirmed prostate cancer cases were only 7 subjects, which indicated a percentage of 0.24% confirmed cancer prostate among our cohort (Figure 1). The age of confirmed prostate cancer cases ranged from 49-68 years, most of them were in the age category of 55-65 years. Their PSA ranged from 4.52-36.26 ng/ml. Gleason score for 4 cases was low grade (3+3), while it was 3+4 for 2 cases, while only one case was advanced cancer (3+5). It is worth mentioning that 96% of our cohort have no PSA testing before.
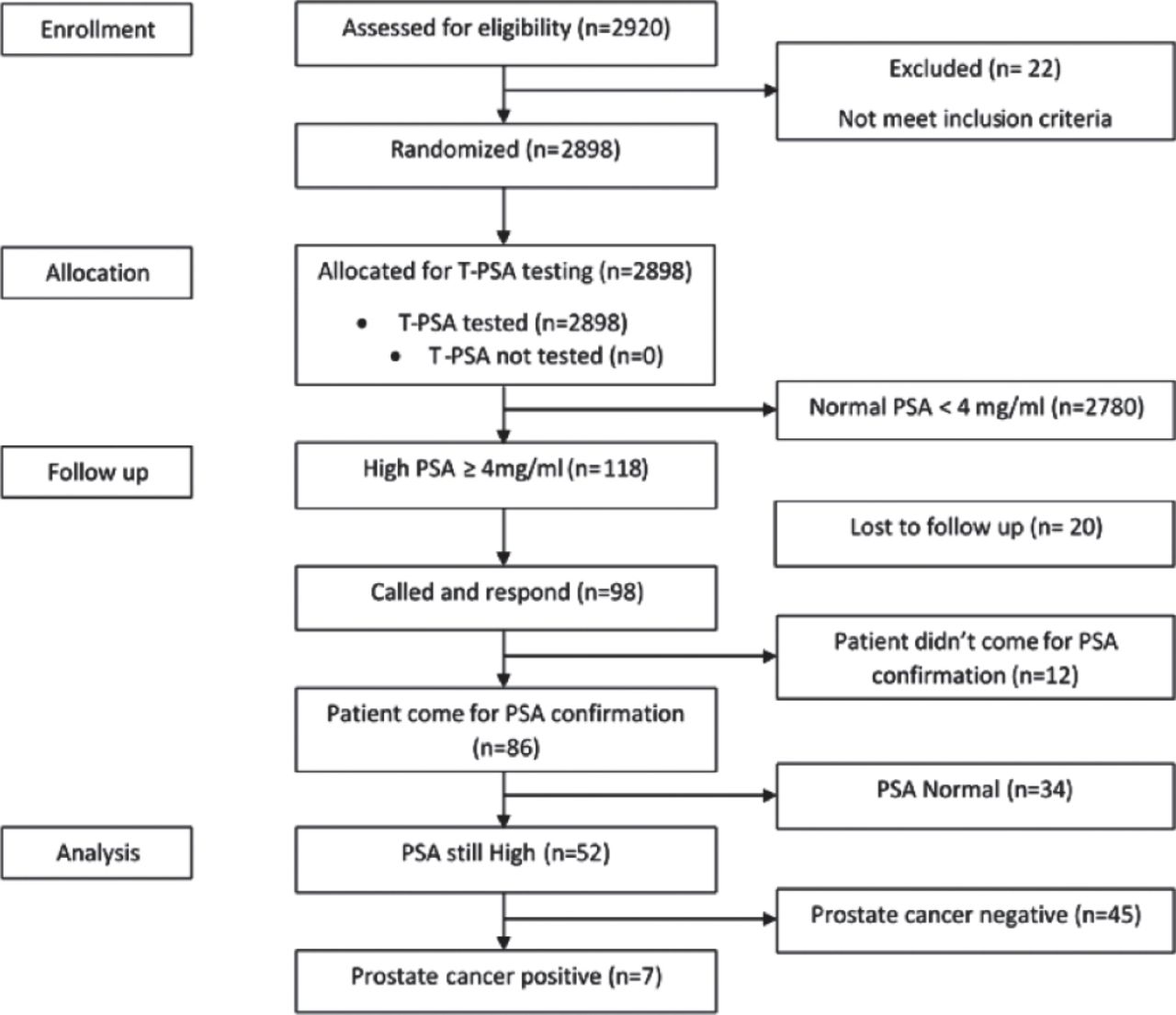
Consort flow diagram.
Discussion
The epidemiological analysis of the reports registered with the Saudi Cancer Registry from 2001 to 2008 reported that the crude incidence rate (CIR) and ASIR of prostate cancer are steadily increasing.8 The results of the present study confirmed the figures emerged from the Saudi Cancer registry, where the incidence rate among our studied cohort was very low (0.24%). In addition to poor attitude and meager behavior among men who were tested high by PSA testing (12%), where they did not show up for confirmation of their results, and further examination. Such an interesting finding was attributed to the fear of the results, anxiety, and lack of interest, as mentioned by most cases when they were re-contacted. In Arafa et al9 study, participants were sharing a common characteristic of poor knowledge and poor attitude towards prostate cancer examination and screening practice. The level of awareness could be the reason why people react poorly towards health issues; other reasons may also prevent them from seeking early detection and diagnosis of prostate cancer, namely, the mistrust of physicians, fear of diagnosis, fear of testing procedures, DRE threatens sexuality, and others.10 Randomized and non-randomized studies have pointed to the harms and opposing effects of screening of prostate cancer with a high incidence of such complications. It was reported that the various uses of shared-decision making process can increase participants knowledge scores, thereby reducing their conflict in making decisions. Therefore, promoting greater involvement in decision making is highly recommended.11 The significance of PSA testing for prostate cancer screening is controversial, in some clinical trial studies, PSA has proved to be a major limitation for identifying the true cases of prostate cancer, with false positive results recorded due to the test’s insensitivity.12,13 Other studies have specified that the PSA screening test decreased the mortality rate of prostate cancer by 20%, but was associated with over-diagnosis.14,15 The great discrepancy in the incidence rate between the current study and Rabah’s12 study (approximately 9 years difference) was mainly ascribed to sample selection which led to over diagnosis. Where men aged 70 years and over were included in the earlier study, among them, a significant percentage of cases had their PSA level above 4 ng/ml and many of them were diagnosed as prostate cancer, in addition, MRI-guided biopsy which was used in the current study resulted in a more precise diagnosis.
The United States Preventive Services Task Force (USPSTF) recommended against PSA screening in healthy men finding that the potential risks outweigh the potential benefits. Such recent recommendation concluded that “PSA-based screening results in small or no decrease in prostate cancer-specific mortality and it could result to harm, pertinent to subsequent evaluation and treatments, some of which may be needless.3,16
The cost of cancer treatment is higher than any other disease; however, it is unethical and unacceptable to let people die from prostate cancer without intervention. Not only because of the cost of treatment, but also due to the widespread use of PSA screening and its high cost, this might be the cause of controversies about prostate cancer screening and treatment.17 It is worth mentioning that the mean annual screening cost at the hospital referral region level ranged from $17 to $62 per recipient, without doubt the cost would be doubled for mass screening for outreach population,17 particularly if we put into consideration the false positive results and increased costs which might be incurred that increases the burden on the country’s resources. Such consideration about the widespread of prostate cancer screening, particularly in developing countries and/or where the incidence is significantly lower might lead to much more controversy about prostate cancer screening. As cost control becomes an important concern in health care systems; physicians should adopt whether the expenses of screening and treatment is worth the expenditure of the limited health care resources.18 The cost-effectiveness study of Heijnsdijk et al19 suggests that prostate cancer screening could be cost-effective when it is limited to 2 or 3 screenings between 55 to 59 years old and that screening above 63 years old is less cost-effective due to their loss in Quality-adjusted life years (QALYs) and over diagnosis. The early detection of prostate cancer is worthwhile only if it detects potentially life-threatening lesions among asymptomatic men at an early stage where lesions are treatable, and if the balance of evidence demonstrates that the prospect of benefit outweighs the potential for harm.20
Study limitation
The current study has certain limitations, first, it was not a population-base study, however, it was conducted in the main University Hospital of Riyadh City, a tertiary hospital which receives patients from different cities around Riyadh, which rendered our sample quite representative of the Saudi population. Approximately 17% were lost to follow-up, this moderately high percentage was mainly due to wrong contact information of some patients either in their records or deliberately given by them. At last DRE was not carried out for most of the patients as it causes embarrassment to such population and hence omitted for all of our cohorts.
In conclusion, the current study is addressing a controversial point about the mass screening of prostate and diagnosis of the disease in its early stages, putting into consideration the very low prevalence of prostate cancer, high cost of mass screening in addition to poor attitude towards screening and its results among men in our region. With such contemplations, we recommend not to adopt a national mass screening program but to encourage PSA testing for men before the age of 50 years and above. It can be carried out at primary health care clinics through shared decision making. This could be activated by enhancing the attitude of men and encouraging their families towards prostate cancer screening and its importance for the early identification of the disease. Such tests could be applied every 1-2 years before the age of 70 years, yet, such test might not be repeated if it remains constantly low for several times.
Acknowledgment
This study was financially supported by Vice Deanship of Research Chairs, King Saud University, Riyadh, Saudi Arabia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was financially supported by the Vice Deanship of Research Chairs, King Saud University, Riyadh, Saudi Arabia.
- Received February 1, 2017.
- Accepted April 11, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.