


Abstract
Objectives: To characterize the cutaneous leishmaniasis (CL) isolates of Syrian and Central Anatolia patients at species levels.
Methods: Skin scrapings of 3 patients (2 Syrian, 1 Turkish) were taken and examined by direct examination, culture in Novy-MacNeal-Nicole (NNN) medium, internal transcribed spacer polymerase chain reaction and sequence analysis (PCR).
Results: According to microscopic examination, culture and PCR methods, 3 samples were detected positive. The sequencing results of all isolates in the study were identified as Leishmania tropica. The same genotypes were detected in the 3 isolates and nucleotide sequence submitted into GenBank with the accession number: KP689599.
Conclusion: This finding could give information about the transmission of CL between Turkey and Syria. Because of the Syrian civil war, most of the Syrian citizens circulating in Turkey and different part of Europe, this can be increase the risk of spreading the disease. So, prevention measurements must be taken urgently.
Leishmaniasis is a vector-borne parasitic disease caused by Leishmania genus protozoa and transmitted to the vertebrate host by female Phlebotominea (Diptera: Psychodidae) sand flies. Leishmaniasis currently ranks second only to malaria in the World Health Organization (WHO) list of protozoan diseases that cause the highest human mortality. It was estimated that approximately 350 million people are under the risk of leishmaniasis infection and 12 million are infected.1 Leishmania is the main causative agent for cutaneous leishmaniasis in Old World with Leishmania tropica (L. tropica). Whereas Leishmania donovani (L. donovani) or Leishmania infantum (L. infantum) are reported as visceral leishmaniasis causative agents. However, some cutaneous leishmaniasis (CL) cases have been reported by L. donovani or L. infantum particularly in Tunis and Yemen.2 Self-healing zoonotic cutaneous leishmaniasis (ZCL) induced by Leishmania major (L. major) and anthroponotic cutaneous leishmaniasis (ACL) induced by L. tropica are 2 known types of CL.1 The CL can be both dry and wet and it is a growing public health problem in Turkey. Southeastern Anatolian and Mediterranean regions are endemic foci for CL caused by L. tropica. Also, in neighboring countries at the southern border of Turkey (Syria, Iraq and Iran), L. major and L. tropica are responsible for CL.3,4 Most (up to 90%) of the global CL cases are observed in few countries: Afghanistan, Algeria, Iran, Iraq, Saudi Arabia, and Syria in the Old World.1 Cutaneous leishmaniasis was observed in very early years and is endemic to Syrian Arab Republic. After 1950’s, the incidence decreased due to antimalarial sprays. But the number of CL cases sharply increased from the 1980s onwards; 4.734 were observed in 1987-1988, 27.739 (new cases) in 2008, 46.148 in 2009, and 58.156 in 2011.3-5 Syria is the most affected nation among Mediterranean countries with more than 25,000 cases per year.6 Due to civil war in Syria, thousands of civilians were forced to leave their country and migrate to safer countries such as Lebanon, Iraq, Jordan, and Turkey. A significant increase in the number of Syrian CL cases was reported in Sanlıurfa Hospitals, Turkey.7 Approximately 2 million refugees currently live in different border provinces in Turkey such as Gaziantep, Sanlıurfa, and Hatay and CL cases are expected to increase in these regions.
Clinical evaluation and microscopic demonstration of the parasite are not sufficient for a conclusive leishmaniasis diagnosis. Further, molecular techniques are crucial in detection of the pathogen species. Molecular biological tools are widely used to screen Leishmania spp. infections in samples obtained from patients and vector species. Also phylogenetic techniques are used to evaluate genetic distances between strains isolated from humans, canines, and vector sand fly species. Thus, we aimed to identify Syrian and Central Anatolian CL patient isolates at the species level using molecular techniques.
Methods
In this descriptive case study, 3 patients with CL suspicion were admitted to the National Reference Laboratories of Parasitology, Turkish Public Health Institution in 2014. Patients were all male and they were 3, 4, and 10 years old (Figure 1). Two patients were from Syria and one from Konya, Turkey. Two Syrian patients mentioned that lesions occurred before leaving Syria. Patients with skin lesions were included in the study.

Patient from Syria with cutaneous leishmaniasis.
The suspicious lesions were sterilized with 70% alcohol and allowed to dry. Skin was scraped with a sterile lancet and the smears were taken from the border of the lesion and divided into 2 parts. The first parts of the samples were fixed with methanol and stained with Giemsa. Then slides were examined under the microscope (100x) for the presence of the amastigote form of the parasite. The slides where amastigote was detected were declared positive after 15 minutes of examination.
The second part of the sample (preparation was the same with slide smears, a small amount of the scraped tissue) was inoculated on Biphasic Novy-MacNeal-Nicolle (NNN) medium. The NNN media included fresh, aseptically collected, defibrinated rabbit blood mixed with agar and penicillin G. And the liquid phase was supplemented with 0.85% saline. The cultures were produced at least in duplicates, incubated at 24°C and observed by microscopy every 72 hours for one month. Positive cultures were subcultured in RPMI-1640 media for 3 days, for further propagation of Leishmania promastigotes. The parasites (approximately 50 mL culture) were washed 3 times by centrifuge (500 x g for 5 min) in cold phosphate-buffered saline (PBS) and the final concentration was adjusted to 5x106 promastigotes/ml. The Leishmania promastigote pellets were suspended in 200 µl PBS and Proteinase K was added. Genomic DNA was isolated with QIAamp DNA Mini kit (Qiagen, Hiden, Germany), according to the manufacturer’s protocol.
Internal Transcribed Spacer 1 (ITS-1) gene was amplified to diagnose and identify the Leishmania species, using previously published primers (LITSR/L5.8S).8 Amplification reactions were performed with the final 50 µL volume containing 5 µL PCR buffer (0.2 ml, Fermentas), 2 mM MgCl2 (25 mM, Fermentas), 1 ml dNTP (10 mM; Fermentas), 20 pMol of each primer, 5 µL genomic DNA and 2 units Taq polymerase (5U/µL, Fermentas). The cycling was conducted at 95°C for 5 minutes followed by 35 amplification cycles, each consisting of 3 steps: denaturation at 95°C for 20 seconds, annealing at 53°C for 30 seconds and extension at 72°C for 1 minute, followed by a final extension at 72°C for 6 minutes. Finally, 8 µL PCR product was loaded in a 1.5% agarose gel electrophoresis and visualized by ultraviolet (UV) trans-illuminator using a 100 bp DNA marker. Positive PCR products were sequenced as noted elsewhere.8
Nucleotide sequences obtained in this study were aligned using ClustalW and the alignment was submitted to the GenBank. Basic Local Alignment Search Tool (BLAST®), used for search for similarities between the sequences, was applied to identify Leishmania species. Sixteen L. tropica sequences previously submitted to the GenBank from different countries were used to generate neighbor-joining (NJ) tree. Leishmania siamensis was used as an out-group in the NJ tree. Maximum parsinomy (MP) and bootstrapping method was conducted with 1000 replicates using Geneious R.8
Results
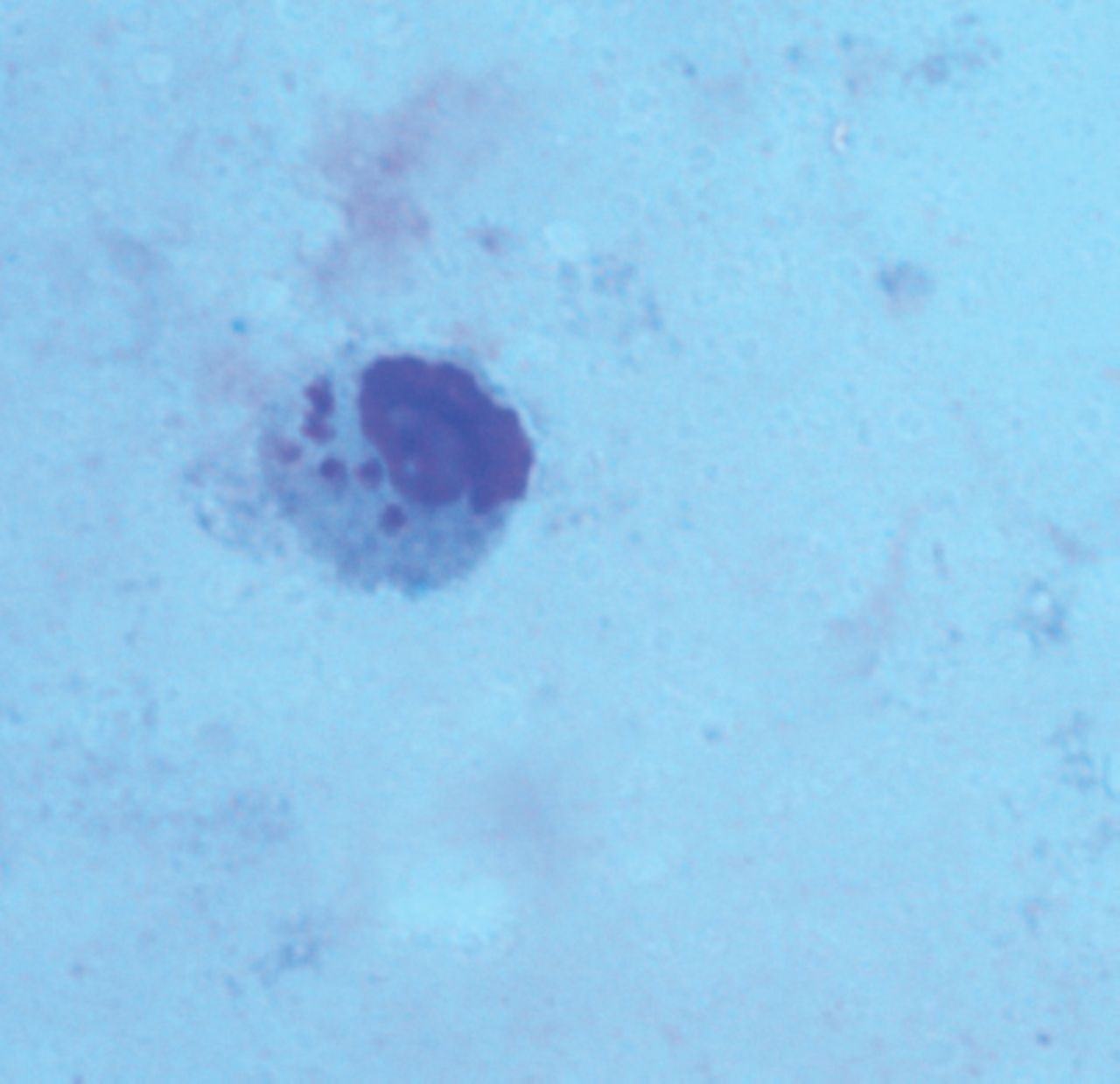
Microscopic examination demonstrated that 3 smears were positive for Leishmania spp. due to the observation of amastigotes in Giemsa stained slides (Figure 2). Also all tissue samples scraped from patients were successfully inoculated in the NNN media and promastigote forms were observed in all 3 samples approximately within 3 weeks. The PCR product of all 3 cultured specimens and one international control DNA demonstrated approximately 300-350 bp amplicon of expected size when visualized under UV trans-illuminator.

Amastigote form in Giemsa stained smears.
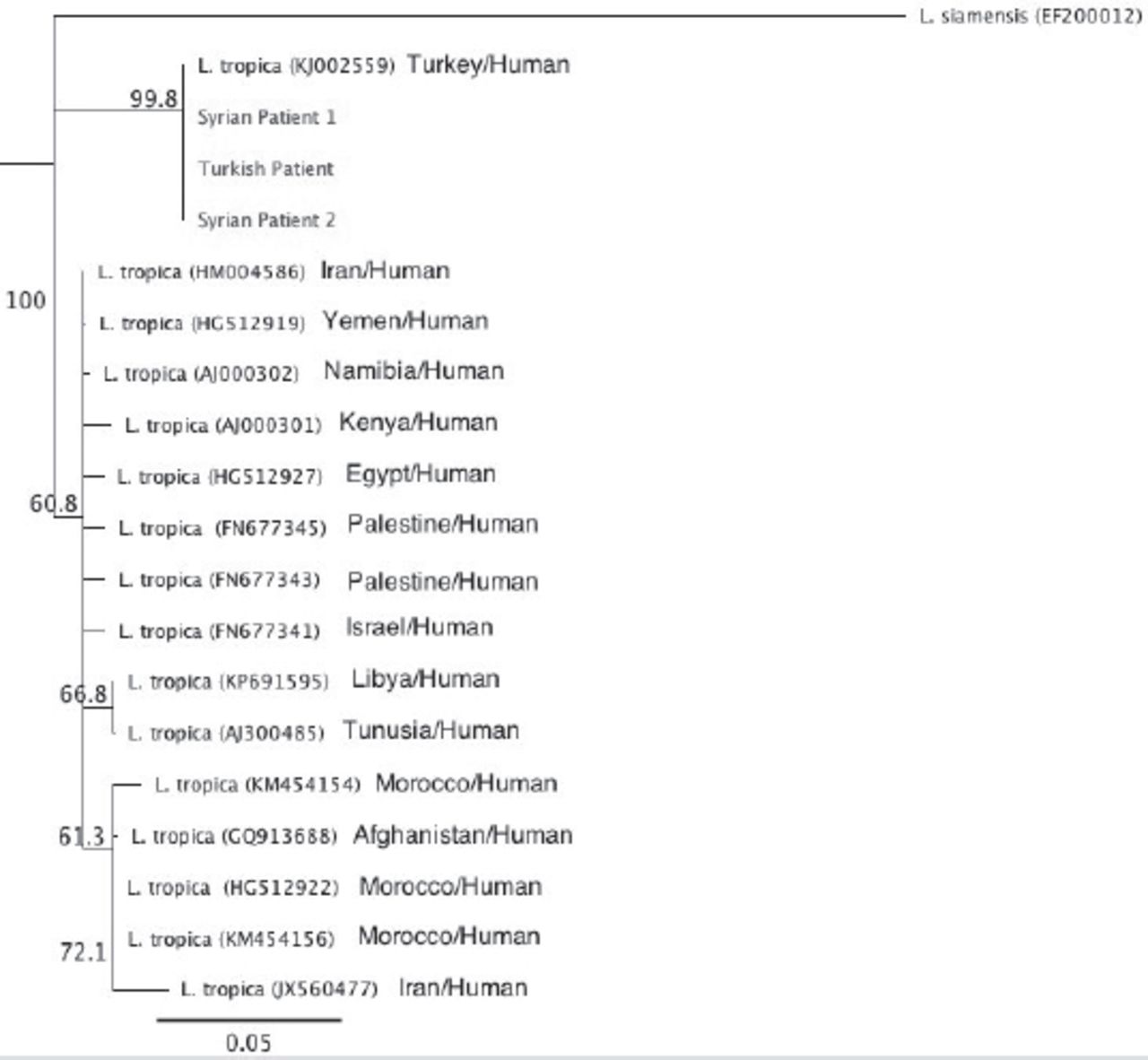
According to the BLAST® similarity search, the sequencing results for all isolates in the study identified L. tropica, the causative agent of ACL. The same genotypes were detected in 3 isolates and the nucleotide sequence submitted into GenBank with the accession number of KP689599. Neighbor-joining tree results demonstrated a slight diversion in these 3 isolates when compared with other isolates used in the tree except one (KJ002559), which was from Adana, Turkey (Figure 3).

Neighbor-Joining tree for the partial ITS1 rRNA sequences of the isolates.
Cutaneous leishmaniasis can be defined as a self-healing dermal disease and typically leaves depressed scars on the infection site. Three different pathogens that cause CL were reported in Turkey. Also L. donovani was identified in a CL patient in France who visited Yemen for 2 weeks.8 Zoonotic cutaneous leishmaniasis (ZCL) caused by L. major was generally defined as wet type, while ACL due to L. tropica was characterized as dry type. In Cukurova plain in Turkey, where CL is hyperendemic, L. infantum is found to be the pathogen.9 Accurate detection of the parasite is important for the diagnosis, prevention and adequate treatment of the disease and also for epidemiologic studies. Microscopy and culture methods have limitations in detecting the infection among patients admitted to hospitals.
Laboratory staff should be experienced or with adequate training for detecting the parasite in stained slides. Previous studies demonstrated that molecular tools were more sensitive compared to microscopy in detecting the infection.3,10 For infection screening among patients, culture method is time consuming and requires a sophisticated laboratory set up and increases the risk of contamination.10 Meanwhile, parasitological methods are not able to identify the species in Leishmania isolates.5,7 The consistency between the results obtained with microscopy, culture and molecular techniques may increase the reliability and quality of the results.
Anthroponotic cutaneous leishmaniasis represents approximately 90% of all CL cases in Syria induced by L. tropica.11 In 2008, 27.739 new ACL cases were identified due to L. tropica and 1.401 new ZCL cases were reported due to L. major.9 Al-Nahhas & Kaldas3 analyzed 32 positive samples using ITS1-PCR RFLP method and L. tropica was found as the pathogen in all isolates. Also in the present study, L. tropica was found in 2 isolates that originated in Syria . Latest government report on Syrian refugees in Turkey emphasized the high-risk of new imported CL cases from Syria.12 In the first 3 months of 2013, the number of Syrian CL patients rapidly increased in the town of Nizip in the city of Gaziantep. In this period, 67 CL patients were identified and 62 (92%) patients were from Syria.13 Konya is the seventh populous city in Turkey, located in Central Anatolia. The city is non-endemic for CL, but 72 cases (0.4%) were reported between 1994 and 2000.14 Also, Toz et al15 determined L. tropica in Central Anatolia, similar to the findings of the present study. Patient travel history was not available and the infection might be due to a visit to CL endemic region. Thus, it is not possible to conclude that CL agent was L. tropica in Central Anatolia.
In the present study, sequence analysis of Konya and Syrian isolates demonstrated 100% homology with each other and also with one isolate from Adana (KJ002559). There was no information on the source of the infection in Konya; therefore, it could be considered that the patient might have traveled to an endemic region, especially the cities on the border with Syria. Phylogenetic analyzes revealed that the sequence data obtained from patients slightly differed from the other sequences submitted previously to the GenBank. The present study demonstrated that utilizing molecular based assays on leishmaniasis provides specific identification of the species.
In this study, existence of L. tropica demonstrated the risk of anthroponotic CL in the study areas. Due to the Syrian civil war, several Syrian citizens travel in Turkey and also in different parts of Europe. This may increase the risk of spreading the disease, therefore prevention measures must be taken urgently.
Clinical Practice Guidelines
Clinical Practice Guidelines must include a short abstract. There should be an Introduction section addressing the objective in producing the guideline, what the guideline is about and who will benefit from the guideline. It should describe the population, conditions, health care setting and clinical management/diagnostic test. Authors should adequately describe the methods used to collect and analyze evidence, recommendations and validation. If it is adapted, authors should include the source, how, and why it is adapted? The guidelines should include not more than 50 references, 2-4 illustrations/tables, and an algorithm.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 11, 2017.
- Accepted August 2, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.