


Abstract
Objectives: To compare Anti-Mullerian hormone (AMH) concentrations between polycystic ovary syndrome (PCOS) patients and healthy women who have polycystic ovarian morphology (PCOM) with regular menstrual cycles, and to determine a diagnostic cutoff value for PCOS women during reproductive period.
Methods: This study was carried out between February 2013 and October 2017 at the Department of Obstetrics and Gynecology, İzmir Katip Çelebi University Atatürk Training and Research Hospital, Izmir, Turkey. Seventy PCOS patients and 70 PCOM women with normal menstrual cycles were included in the study. Blood samples of the subjects were obtained following an 8-hour fast for AMH and biochemical assessments, serum gonadotropin, and androgen measurements.
Results: The mean serum AMH levels of PCOS patients were found to be higher than PCOM women with normal menstrual cycles (p<0.01). The optimal serum AMH cutoff value for PCOS diagnosis was determined as 3.51 ng/ml (sensitivity 72.8%, specificity 75.7%).
Conclusion: Serum AMH concentrations are significantly higher in PCOS patients independent from the ovarian morphology and number of follicles per ovary. Positive and negative predictive values of AMH in PCOS diagnosis were found to be 75% and 73.6%, respectively, with a cutoff value of 3.51 ng/mL.
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder affecting 6-20% of women in reproductive age.1 The PCOS diagnosis is based on criteria adopted in 2004 and updated in 2012, consisting of either clinical or biochemical hyperandrogenism, oligo/anovulation and polycystic ovarian morphology (PCOM) on ultrasound which is defined as the presence of more than 12 follicles, 2-9 mm in diameter each, in an ovary or an ovarian volume greater than 10 cm3.2,3 The presence of at least 2 out of 3 aforementioned criteria is sufficient for PCOS diagnosis. However, since ultrasonographic imaging is user and device dependent, and current high resolution ultrasonography devices have increased the demonstrability of 2-9 mm follicles, the threshold value of follicles for PCOS diagnosis is controversial.4,5 Another controversy concerning the subject is whether the PCOM in women is a clinically non-significant variation, or a predisposing or mild clinical form of PCOS.6
Anti-Mullerian hormone (AMH)’s serum concentration is significantly correlated with the amount of pre-antral and small follicles.7 Thus, AMH is used as an effective marker of ovarian follicular reserve and ovarian senility.8,9 Although there are several studies reporting a strong correlation between AMH elevation and PCOS phenotype as well as ovulatory dysfunction, whether morphological alterations in the ovary or biochemical-hormonal interactions play a major role in the hormone level elevation is still controversial.10,11 Studies claiming that AMH is strongly correlated with standard diagnostic criteria and that serum AMH elevation is an objective predictor of PCOS diagnosis are abundant in the literature.12,13 Although different cutoff values for PCOS diagnosis have been defined by various studies, no AMH cutoff value is yet generally accepted for PCOS diagnosis.14,15
The aim of this study is to compare the AMH concentration and other biochemical parameters of otherwise healthy PCOM women with that of PCOS patients, and to determine an AMH cutoff value that can support PCOS diagnosis.
Methods
This cross-sectional study was carried out between February 2013 and October 2017 at the Department of Obstetrics & Gynecology, İzmir Katip Çelebi University Atatürk Training and Research Hospital, Izmir, Turkey. The study protocol was accepted by the Izmir Katip Celebi University local ethics committee (IRB 2013-111). The study was registered on Clinical Trials Gov. (NCT01878955). Ethical principles of Declaration of Helsinki for medical research involving human subject was applied in the study. Verbal or written informed consent confirmed by all participants. The power of the study was calculated using G-Power software (version 3.1).16 In order to determine the difference between the AMH values between 2 groups by using the mean effect size d = 0.05 suggested by Cohen (1988), with type 1 error = 0.05, and statistical power = 0.80, the sample size was determined at 64 patients.17
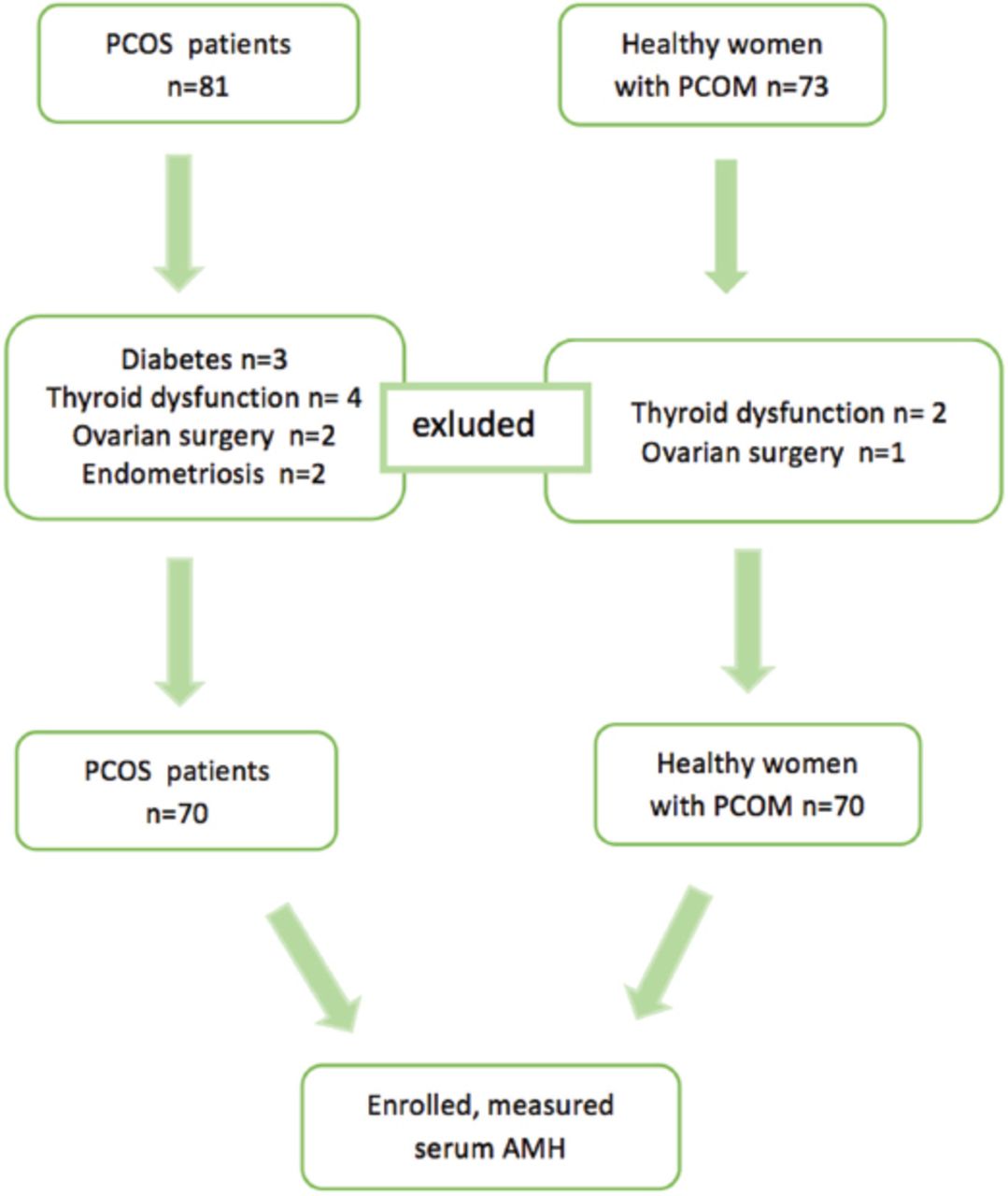
Seventy women aged between 15 and 45 years diagnosed as PCOS according to Rotterdam criteria, and 70 otherwise healthy, non-hirsute women in the same age group who had normal menstrual cycles and PCOM on ultrasonography were included in the study. Patients with diabetes, adrenal or thyroid dysfunction, previous history of ovarian surgery or endometriosis, and patients using drugs altering endocrine functions were excluded (Figure 1).
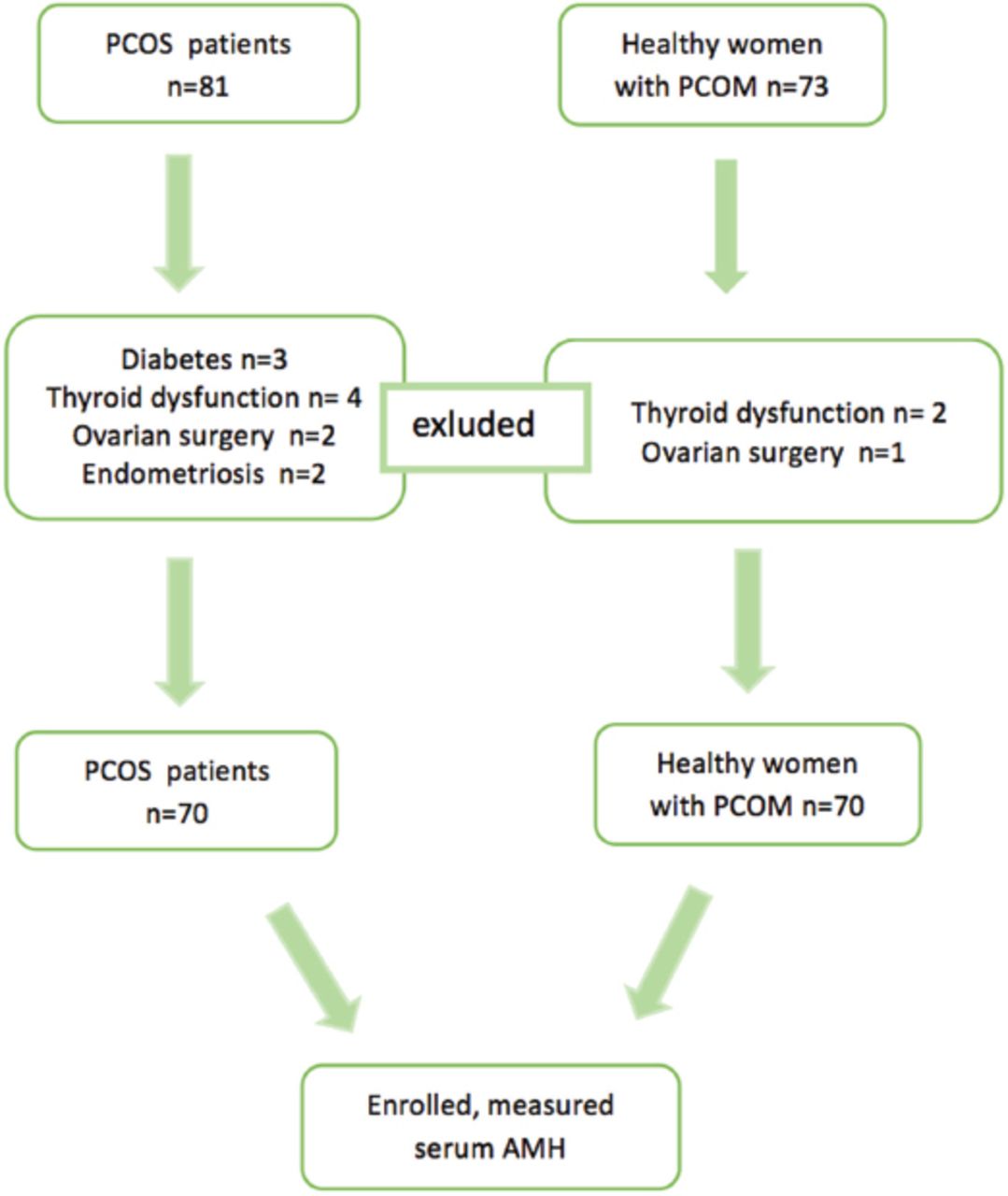
Flowchart of the study design. PCOS - Polycystic ovary syndrome, PCOM - polycystic ovarian morphology, AMH - Anti-Mullerian hormone
Physical and gynecological examinations of the subjects were performed as well as body mass index and modified Ferriman Gallwey (MFG) scores were calculated. Serum glucose, insulin, lipid and AMH levels of the patients were assessed in venous blood after an 8-hour fast. Follicle stimulating hormone (FSH), luteinizing hormone (LH) and total testosterone measurements were performed during the early follicular phase. Ultrasonographic examinations were performed either with a 7 MHz transvaginal probe or with a 5 MHz convex probe and a full bladder (The SonoAce X8 Ultrasound System Samsung Medison, S.Korea). The number of follicles per ovary (FNPO) was calculated by dividing the total number of follicles in both ovaries by 2.
Serum total testosterone levels were maesured by using ELISA technique (Beckman-Coulter, Villepinte, France). A total testosterone level ≥76 ng/dL was defined as biochemical hyperandrogenemia, whereas a MFG score ≥8 was defined as clinical hyperandrogenism. The homeostatic model assessment for insulin resistance (HOMA-IR) score was calculated to assess the glucose metabolism (fasting glucose x fasting insulin/450). Homeostatic model assessment for insulin resistance scores >2.5 were considered insulin resistant. Subjects with serum AMH <1 ng/mL and serum FSH >12 mU / mL were excluded from the study. Serum AMH levels were measured by ELISA using an appropriate commercial kit (Beckman Coulter, Chaska, MN, USA), mean inter- and intra-assay Coefficient of Variability (CVS) of 4.5% and 3.6%, respectively. Serum glucose, cholesterol and triglyceride measurements were performed with the appropriate kits suggested by the manufacturer (Cobas 8000, Roche Diagnostics, Mannheim, Germany). Serum insulin, FSH and LH levels were assessed by ELISA (DRG International, Inc., USA). The intra- and inter-assay coefficients of variation were below 10%. Data were evaluated in the statistical package program IBM SPSS Statistics 25.0 (IBM Corp., Armonk, New York, USA) Normal distributions of the numerical variables were evaluated by Shapiro Wilk normality test and Q-Q graphs. Comparison of the groups were performed by independent 2-sample t test and Mann-Whitney U test for normally distributed variables and non-normally distributed variables, respectively. Anti-Mullerian hormone comparison between the groups was performed by covariance analysis after correction for confounding factors. Receiver operating characteristic (ROC) analyses was used to determine cutoff, sensitivity, specificity, positive and negative predictive values. The relationships between numerical variables were evaluated by Pearson correlation coefficient or Spearman correlation analysis. Fisher Chi-square exact test was used for RXC tables to compare categoric variables. P<0.05 was regarded as statistically significant.
Results
Groups were similar in terms of fertility status, mean number of deliveries, fasting serum glucose, and FSH levels. The mean age of the PCOS group was found to be significantly lower than PCOM women. The mean serum AMH levels of patients with PCOS were found to be higher than PCOM women with normal menstrual cycles. The groups were significantly different from each other in terms of FNPO, BMI, modified Ferriman Gallwey score, HOMA-IR score, serum AMH, lipid and LH levels (Table 1). Evaluation of the groups in terms of fertility status revealed 12.9% (n=9) of healthy women with PCOM and 38.6% (n=27) of women with PCOS to be virgin and the number of patients diagnosed with infertility in both groups to be equal. Approximately 68.3% of healthy PCOM women and 39.3% of PCOS women were found to be fertile. Groups were found to be similar in terms of fertility after the exclusion of virgin cases.
Clinical and biochemical characteristics of the groups.
Assessment of the independent variables’ correlations according to the AMH dependent variable revealed that the variables age, BMI, insulin level, LH and FNPO are confounding factors among the groups. All variables with differences between the groups were modeled with group variables in general linear models to eliminate the effects of confounding factors. While AMH was negatively correlated with age and BMI, it was positively correlated with LH and fasting glucose level, and moderately positively correlated with FNPO. Evaluation of the intergroup correlations of independent variables showed that age and BMI in healthy PCOM women were correlated with AMH, whereas in PCOS women only age was correlated with AMH (Table 2).
Correlations between Anti-Mullerian hormone (AMH) and other variables.
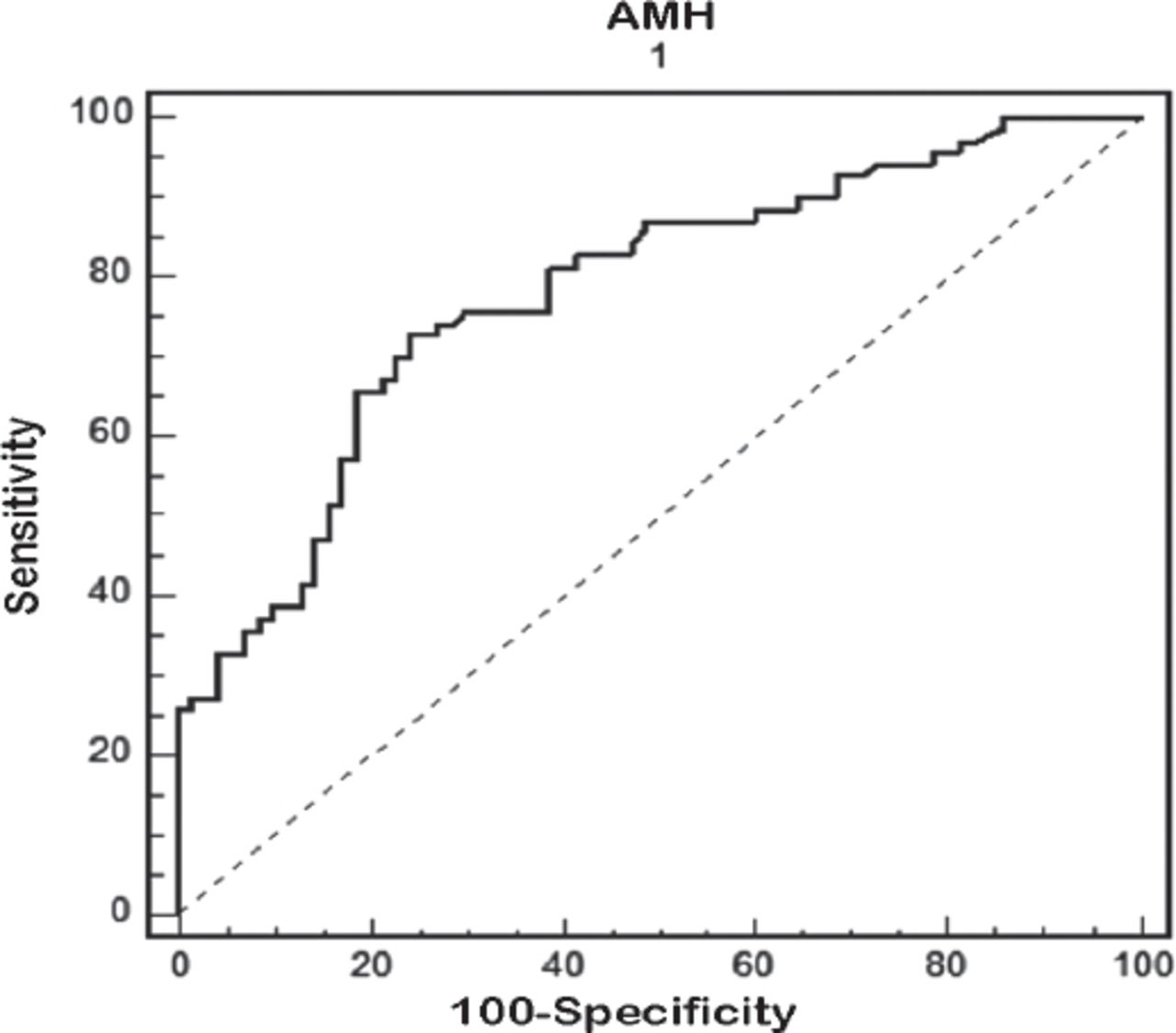
Groups were compared in terms of AMH with covariance analysis after correction for the confounding factors and serum AMH level was found to be significantly higher in PCOS patients. Positive and negative predictive values of AMH in PCOS diagnosis were found to be 75% and 73.6%, respectively, with a cutoff value of 3.51 ng/mL. In the ROC analysis performed for the optimal serum AMH level for PCOS diagnosis, the area under the curve was 0.781, sensitivity for cutoff value 3.51 was 72.8% (95% CI 60.9 - 82.8) and specificity was 75.7% (95% CI 64.0 - 85.2) (Figure 2).
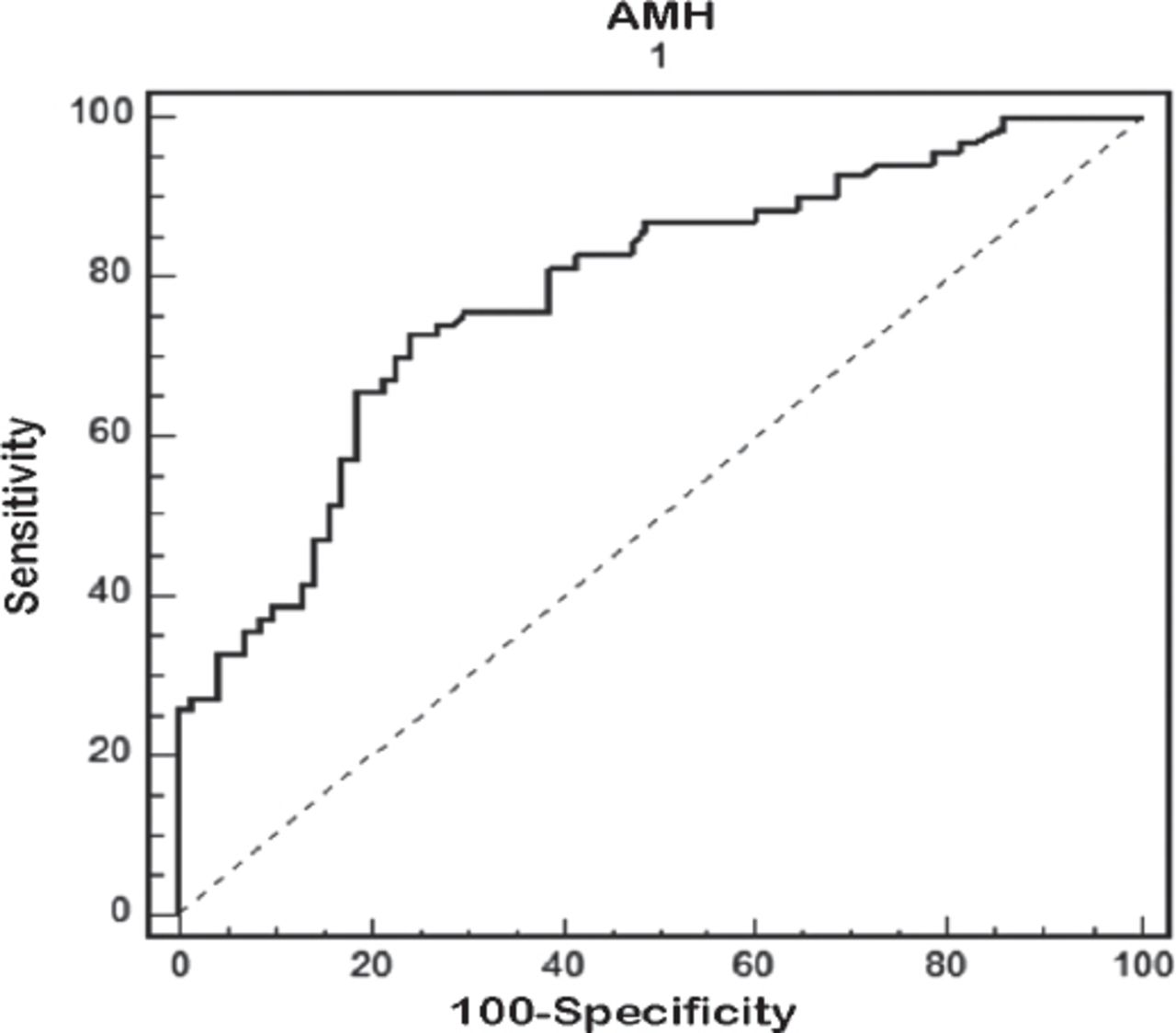
Receiver operating characteristic curve of the predictive value of AMH for polycystic ovary syndrome. AMH - Anti-Mullerian hormone
Discussion
In the current study, serum AMH concentrations of PCOS women were found to be significantly higher than healthy PCOM women after correction for confounding factors such as age, BMI, insulin level, LH, and FNPO. Comparison of PCOS patients and PCOM women with regular menstrual cycles revealed a significant difference among the groups in terms of hirsutism scores, BMI, FNPO, serum lipid concentrations, insulin resistance and LH levels, while no difference was detected in serum glucose levels and fertility status (p>0,05).
Anti-Mullerian hormone cutoff value that can be used to distinguish healthy PCOM women and PCOS cases is found to be 3.51 ng/mL. In the literature, AMH cutoff value results have been reported, such as 8 ng/mL for Chinese young adults (17-24 years), 8.4 ng/mL for European patients in the same age group and 3.8 ng/mL for young adults from northwestern Turkey.18-21 Despite being slightly lower than the threshold value determined for foreign populations, our result is quite close to the cutoff value reported from in Turkey.12,19,23 The difference of our results from the literature might be explained by racial differences as well as the age range (15-43 years) of our study group, which covers almost the entire fertile period unlike other studies composed merely of young adults.
Several studies have reported that AMH is strongly correlated with the baseline phenotypic characteristics of PCOS as well as the number of small antral follicles.19,20 Similarly, AMH level correlated significantly with age, fasting insulin, BMI, FNPO and LH in our study. Reduction in serum AMH levels with age has been shown and suggested as a marker for menopause prediction in several clinical trials.10,22 Concordant with the literature, we found that AMH is negatively correlated with age in both PCOS patients and healthy PCOM women.
Comparison of groups in terms of serum glucose, insulin levels and HOMA-IR scores revealed a significant difference among HOMA-IR and insulin levels. Different results have been obtained by various studies conducted in 2 different regions of our country. While Tokmak et al24 defined a significant correlation between AMH and insulin resistance (IR) among non-obese adolescents, Şahmay et al25 reported no correlation between AMH and IR. Although there was a weak positive correlation between insulin level and AMH in our study, no correlation between IR, serum fasting glucose and AMH was detected. The presence of hyperinsulinemia in PCOS cases has been proposed to be due to increased AMH release from granulosa cells via androgen uptake.26
A strong positive correlation between AMH levels, FNPO, LH levels and hyperandrogenism was detected in our study. Studies have reported a positive correlation between AMH and the number of small antral follicles in both healthy women and PCOS cases. Luteinizing hormone elevation is reported to increase AMH secretion from granulosa cells in PCOS cases.27,28 We detected a negative correlation between AMH and BMI. The results of other studies are controversial; however,29-31 despite the ambiguous relationship between obesity and AMH, the effect of obesity on AMH levels is suggested to be due to the inflammatory and oxidative stress that develops in the ovarian follicular microenvironment.32,33
The limitations of the study were the AMH measurement was carried out by different methods in different studies in the literature. Furthermore, the participants of the PCOM group consisted of women who had primary dysmenorrhea or healthy women whom were counseling requests. The heterogeneity of this group may have been a selection bias.
There was no significant difference in fertility between the groups in our study. Polycystic ovary syndrome is a major cause of infertility due to anovulation.34 The lack of difference in fertility between the groups in our study might be due to more than one third of PCOS cases being excluded from fertility status evaluation because they were virgins.
In conclusion, PCOM and PCOS differ in their clinical and metabolic characteristics. Anti-Mullerian hormone plays an important role in the pathophysiology of PCOS and can be used as an adjunct to other metabolic variables in PCOS diagnosis and differentiation. However, there is a need for multicenter studies to determine a cut-off value for AMH level.
Acknowledgment
We would like to thank American Manuscript Editors (www.americanmanuscripteditors.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 19, 2018.
- Accepted August 22, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.