


Abstract
Objectives: To assess the changes in parameters of thyroid carcinoma, particularly papillary type, in the era of widespread use of sensitive diagnostic methods. We aim to investigate whether the increased frequency of thyroid cancer is true or resulted from over diagnosis.
Methods: We conducted a retrospective study of 313 cases of thyroid carcinoma diagnosed at Jordan: University Hospital and King Hussein Cancer Center from 2007-2015. Papillary carcinoma accounted for 290 (92.7%) of all cases. Cases were sub classified according to demographic features, histological type, size, stage, and other variables. For comparison of data, cases were subdivided into 2 study periods: Group I included patients diagnosed in the period 2007-2010, and Group II in the period 2011-2015.
Results: The frequency of thyroid carcinoma has increased across the study period. Papillary carcinoma was the major type accounting for this increase. Papillary micro carcinomas ≤1cm accounted for 34.8% of cases of PTC. Most cases (52.4%) of papillary thyroid carcinoma (PTC) were localized stage tumors. Group II of the study witnessed a more than doubled number of cases of PTC compared to group I, with increased frequency of tumors of all sizes as well as tumors of both localized and regional stages.
Conclusions: Our observed trend cannot be totally explained by over diagnosis and increased diagnostic scrutiny. This increase could be of true nature and cannot be explained by single cause.
Thyroid carcinoma is becoming the most rapidly increasing cancer in the past few decades.1 It is the fifth most commonly encountered cancer among female patients, according to the most recent cancer statistics from the United States.1 Several population-based studies derived from large cancer registries worldwide have found that this increase is almost entirely from high incidence of papillary thyroid carcinoma.2-15 The rising incidence of thyroid cancer has long been a controversial issue among experts. Some authors believed that the apparent increase in incidence is most likely due to increased use of sensitive diagnostic measures and detection of small subclinical tumors and called this as over diagnosis.6 The increased use of sensitive diagnostic modalities such as neck ultrasound has permitted the detection of as small as 2 mm nodules in the thyroid.16 Subsequent fine-needle aspirations of these nodules have facilitated the detection of these small cancers on cytological backgrounds. At the same time, it is believed that a large reservoir of occult papillary thyroid cancers is detected in 10-36% of cadavers in classical autopsy studies, and those would most probably have remained silent unless more sensitive methods were used for their detection or discovered incidentally in thyroid glands.17 On the other hand, other experts argued that the increased incidence involved all sizes, including larger cancers and cancers with extra thyroid extension and lymph node metastasis as well.18 These authors claimed that the increased incidence is true and is related to exposure to unknown environmental carcinogens and hormonal factors that warrants further research for their identification. The aim of this study was to assess the changes in parameters of thyroid malignancy, discussing the reasons in a 9-year period in a retrospective 2 institutional study and to investigate whether the increased frequency of thyroid cancer is true or results from overdiagnosis of microcarcinomas. In other words, do we actually face an increase in the diagnosis of thyroid cancer? And if so, is it only the improved diagnostic measures that builds up this increase or it is due to unknown hormonal, dietary, genetic, or environmental unidentifiable risk factors?
Methods
A retrospective study was conducted between January 2007 and December 2015. All cases of thyroid cancer at Jordan University Hospital (JUH) and King Hussein Cancer Center (KHCC) in Amman, Jordan, were identified from the institutional database pathology records following approval from the institutional review boards. Research was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
A total of 313 cases were retrospectively identified and included in this review. Subsequently, all hematoxylin and eosin (H&E) stained slides and, if present, the immunohistochemical stains were retrieved, and each case was examined independently by at least 2 pathologists participating in the study. Thereafter, all cases were classified according to the histological classification of the World Health Organization (WHO) into papillary, follicular, Hurthle cell, medullary, poorly differentiated and anaplastic carcinomas.19 Major variants of papillary carcinoma according to the WHO were classic, follicular, and microcarcinoma (≤1 cm). Rare variants were also recorded, including tall cell, diffuse sclerosing, oncocytic, and others. Cases were staged in keeping with the most recent version of thyroid cancer classification Tumor, lymph nodes and metastasis staging (TNM) according to Union for International Cancer Control (UICC) (7th edition).
Cases were substratified with respect to demographic features, histologic type, variant, tumor size, extra thyroid extension, lymph node involvement, focality, pathologic T stage, and presence of associated chronic lymphocytic/Hashimoto’s thyroiditis. For comparison of data, the cases were subsequently subdivided into 2 almost equal study periods: Group I included patients diagnosed from 2007-2010, and Group II from 2011-2015.
We grouped the patients according to tumor size into 4 groups, microcarcinomas (≤1cm), small (1.1-2cm), intermediate (2.1-4 cm) and large tumors (>4 cm). These size criteria were selected because they correspond to the thyroid cancer TNM classification according to UICC.
Because micro carcinomas ≤1 cm are rarely palpable and usually asymptomatic, this size was assumed to be representative of subclinical disease in this study. Localized disease was defined as invasive cancer confined to the thyroid gland and was considered early stage. Regional disease was defined as invasive cancer with evidence of extra-thyroid extension and/or neck lymph node metastasis and was considered late-stage disease. Lymph nodes were sent for histological examination according to the surgeon’s decision based on clinical suspicion. Information regarding distant metastasis was not available in the pathology records.
Because stage is a better measure of outcome than size alone, we assumed that any increase in the frequency of late-stage disease suggests a real change in the frequency of thyroid cancer that is attributable to true etiological factors and not entirely related to increased detection of subclinical cases.
If the increased diagnosis of thyroid cancer was entirely related to the use of more sensitive diagnostic practices, we would expect greater increases in the detection of small, subclinical micro carcinomas, but we would not expect any change in the frequency of larger, clinically apparent tumors and tumors with advanced stage and adverse prognostic factors.
Inclusion and exclusion criteria
Cases were included in the study if the tumor was a primary thyroid carcinoma. We excluded noninvasive follicular thyroid neoplasm (NIFTP) with papillary-like nuclear features, lymphomas, and metastatic carcinomas from this study.
Statistical analysis
The data were managed and analyzed using the Statistical Package for the Social Science for Windows version 21.0 (IBM Corp., Armonk, NY, USA). A significance criterion of p-value <0.05 was used. The chi square test was used to compare distribution of all factors among the study periods. Trends analysis was applied showing the scatter plot and fitted line for the annual percent change out of regression model.
Results
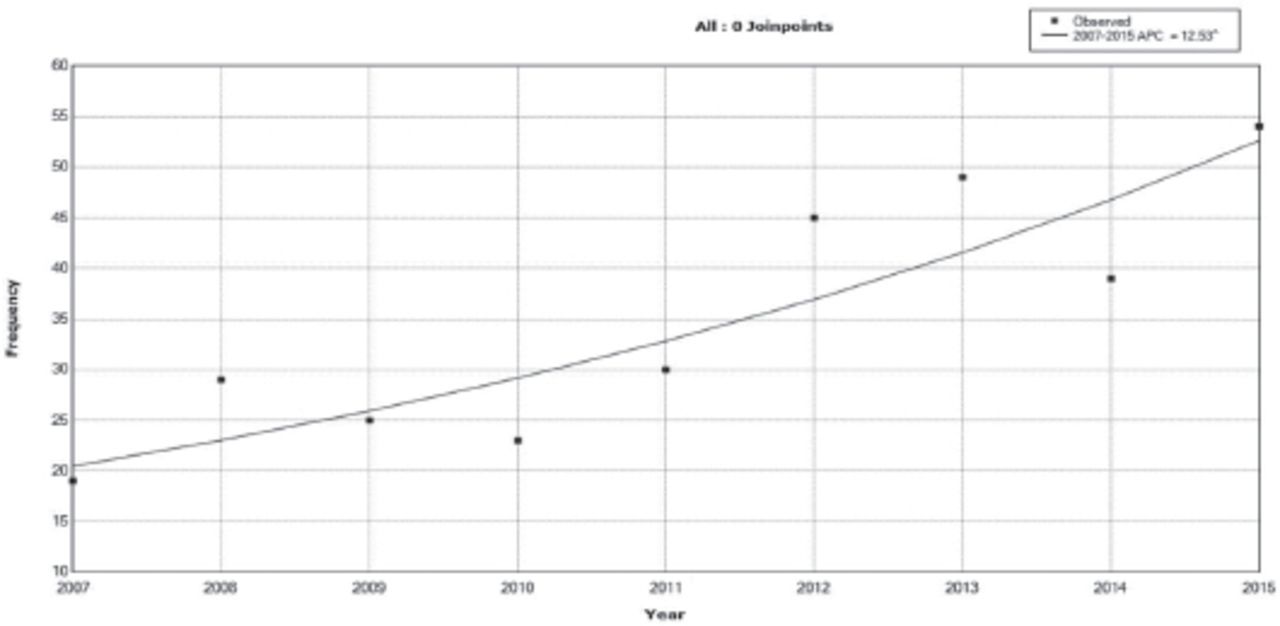
The analysis included 313 cases of thyroid carcinoma, out of which 290 cases (92.7%) were papillary thyroid carcinoma, followed by Hurthle cell carcinoma (11 cases, 3.5%). Follicular carcinoma constituted 0.6%, medullary carcinoma constituted 1.3%, poorly differentiated carcinoma constituted 1% and anaplastic carcinoma constituted 1%. The rising trend in thyroid carcinoma across all the years of our study is shown in Figure 1. The total number of cases increased from 19 cases diagnosed in 2007 to 54 cases diagnosed in 2015, which translates to an annual percent change of 12.53%.
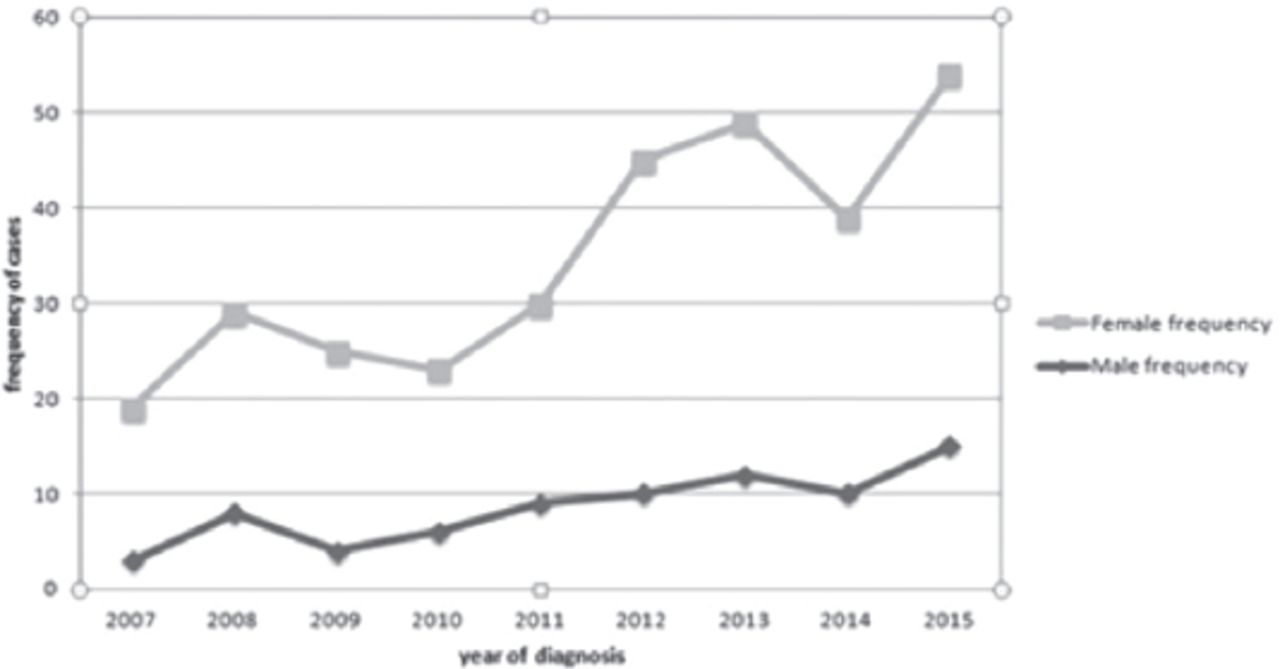
The majority of patients clustered in 2 age groups (20–39 years) constituting 41% (130) and (40–59 years) constituting 37.7% (118). The mean age at diagnosis was 42 years for males and 41.8 years for females. Overall, 236 cases were diagnosed in females (75.4%), whereas 77 cases were diagnosed in males (24.6%). Figure 2 shows the change in frequency of thyroid carcinoma in both genders across the study period.
Papillary thyroid carcinoma (PTC) was by far the most frequent cancer among all gender and age groups. Subsequently, we restricted our analysis to the PTC histological type.
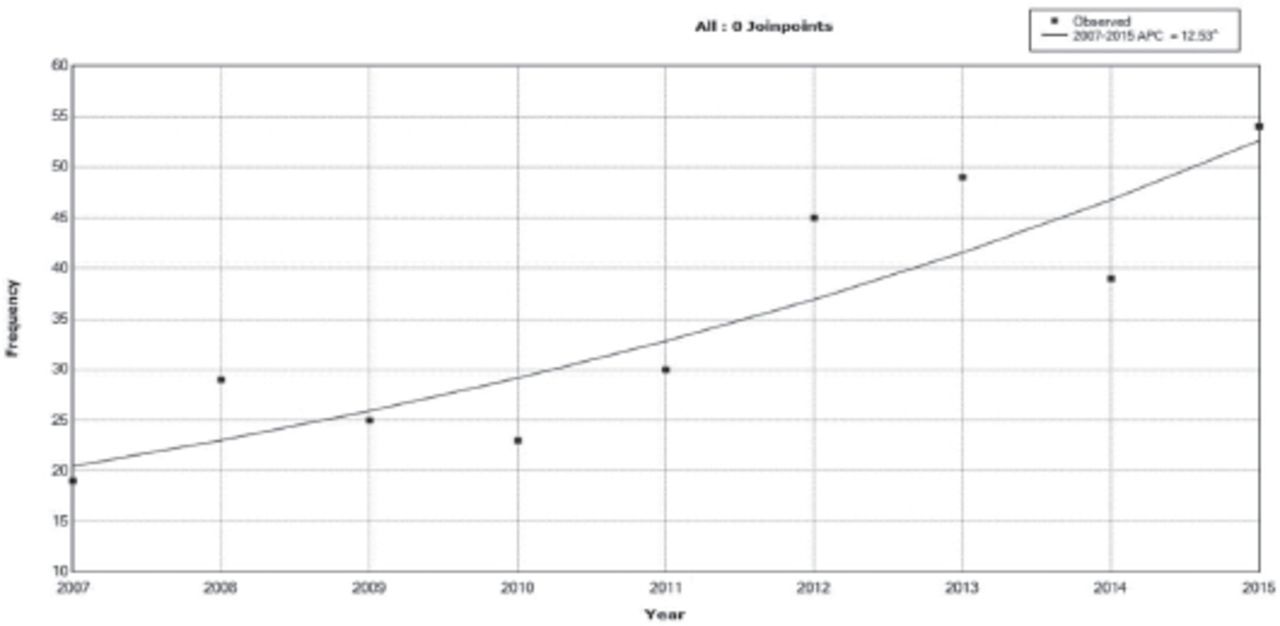
Overall frequency change in thyroid carcinoma across the study period from 2007 to 2015. X-axis: years of diagnosis, Y-axis: frequency of cases.
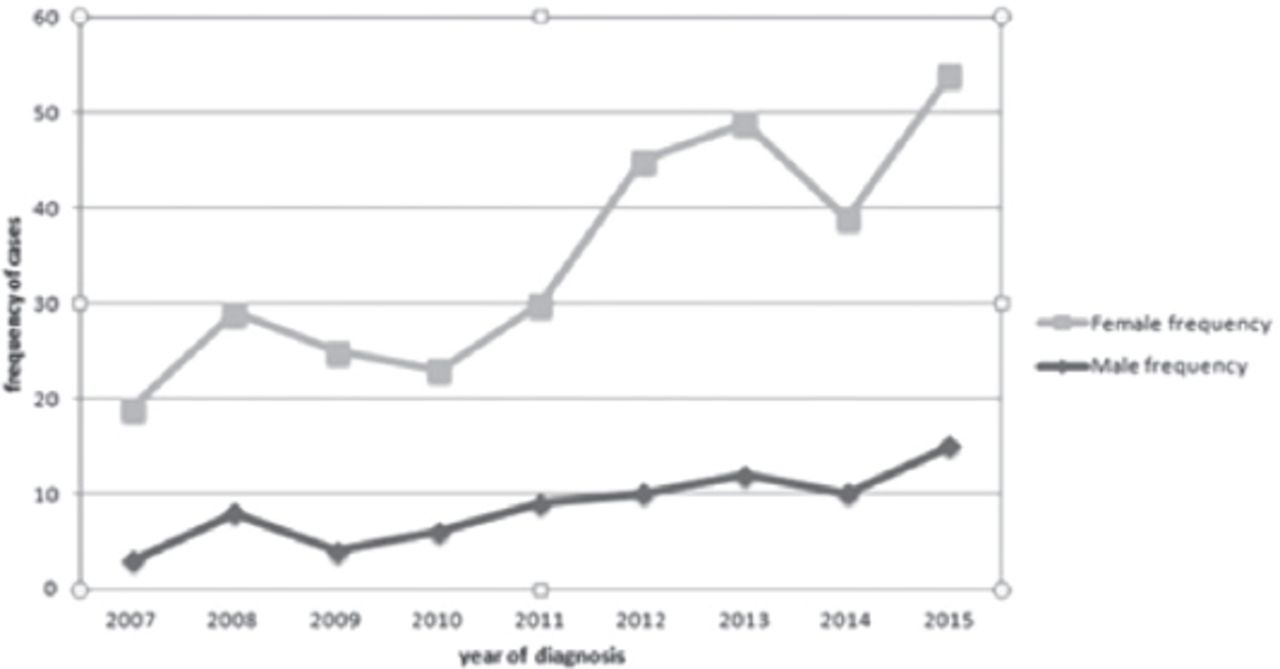
Frequency of thyroid carcinoma by gender across the study period 2007–2015, X-axis: year of diagnosis, Y-axis: frequency of cases.
The classical (conventional) variant of PTC dominated, accounting for 145 cases (50.0%). A substantial number of cases were papillary micro carcinoma variant (101, 34.8%). The distribution of other variants is shown in Table 1. Regarding size distribution, most of the PTC cases were microcarcinomas ≤1.0 cm, constituting 101/290 (34.8%), small cancers measuring 1.1-2 cm are the second most common, accounting for 94/290 (32.4%). Other sizes’ distributions are shown in Table 2. The majority of patients had small-size and low-stage tumors.
Distribution of variants of the 290 cases of papillary thyroid carcinoma (PTC) diagnosed from 2007 to 2015.
Overall characteristics of 290 cases of papillary thyroid carcinoma over the study period and comparison of cases in the 2 periods of the study with different parameters.
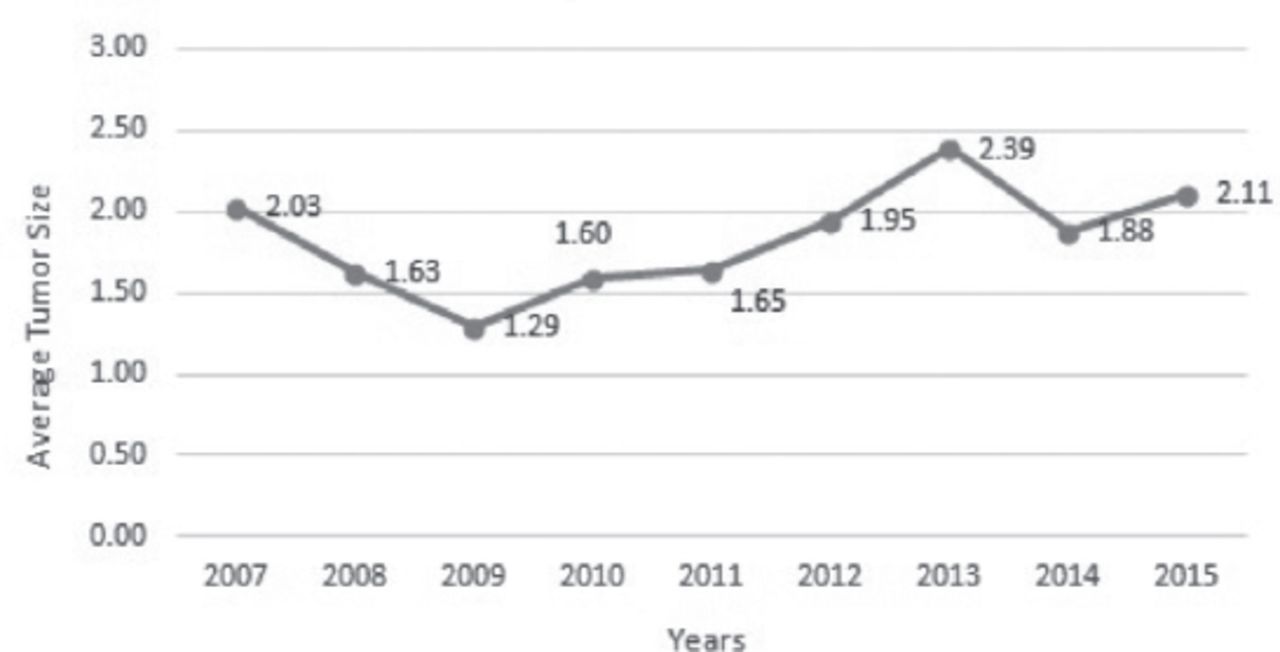
Figure 3 shows the change in average tumor size for the year of diagnosis over the study period from 2007 to 2015. Extra thyroid extension was found in only 72/290 (24.8% of cases). Lymph node metastatic deposits (pN1) were found in 117/290 (40.3%). However, the remaining cases were either negative for lymph node metastasis upon examination of surgically resected lymph nodes, pN0 (91/290, 31.4%) or lymph nodes were not sent for examination, pNx (82/290, 28.3%).

Average tumor size change per year of diagnosis across the study period 2007-2015. X-axis - Year of diagnosis, Y - axis - average tumor size in centimeters.
The majority of PTC were localized stage (152, 52.4%). T1 stage tumors accounted for the great majority of cases (153, 52.8%), followed by T3 tumors (70, 24.1%). On the other hand, T2 stage tumors accounted for 20.3% and T4 stage tumors accounted for 2.8%. Information regarding multifocality and coexisting Hashimoto/chronic lymphocytic thyroiditis are shown in Table 2.
Time trends: Age and gender time trends in papillary carcinomas
The mean age of the investigated patients was almost similar between both groups, with a clearly visible tendency toward an increasing risk of thyroid cancer in the population of females of a young age.
Histological type time trends
There was a substantial increase in the frequency of total thyroid carcinomas (96 versus 217) and papillary carcinomas in particular. The proportion of PTC increased from (86, 89.6%) in group I to (204, 94.0%) in group II. In both groups, PTC predominated.
An increased number of cases were observed in the 3 main variants of PTC in the second period of the study (2011–2015). Moreover, most of the increase was observed in the classic (conventional) variant (39, 45.3% to 106, 52%) followed by the microcarcinoma variant. However, the microcarcinoma variant constituted a lower percentage of the overall tumors in the second group (41.9% in group I and 31.9% in group II), but this percentage reduction was not statistically significant (p-value 0.123).
Tumor-size time trends in papillary thyroid carcinomas
Disease absolute frequency rates increased for tumors of all sizes. However, a shift toward microcarcinomas and small tumors in both groups is noted (66 cases in group I and 129 cases in group II) in Table 2.
In both groups, microcarcinomas (≤1cm) constituted the majority of cases (36, 41.9% in group I, and 65, 31.9% in group II), followed by the small-tumor category, measuring 1–2 cm. The reduction in the overall percentage of microcarcinomas and small tumors (which was observed in group II compared to group I) was not statistically significant (p-value 0.123). In addition, an increased number of PTC of the intermediate size category (2.1–4 cm) was also observed in group II.
Stage-specific time trends in papillary thyroid carcinomas
The second period of the study witnessed an increased absolute number of cases from all stages, except for the T4 stage. T1-stage tumors were predominant in both study groups. The absolute frequency of both localized and regional stage cancers increased over time. However, localized disease was predominant.
No statistically significant differences were observed between the study groups in the frequency of extra thyroid extension, lymph node metastasis, multifocality and the concomitant Hashimoto/chronic lymphocytic thyroiditis (Table 2).
Discussion
Our study shows that the frequency of thyroid cancer has increased in the study period from 2007 to 2015, and that papillary thyroid carcinoma was the only histological subtype accounting for this increase. These findings are congruent with findings from other countries worldwide.2,3 Similar increase was found in the United States, Australia, Poland, Turkey, England, Iran, and the Arab countries, including the kingdom of Saudi Arabia and the United Arab Emirates.1,4-6-14
We also found that the major burden of this increase fell on the female gender and struck patients of young age groups, as is already known.8,9-11,12
We focused on PTC, and our findings demonstrate that more than half of the cases of papillary thyroid carcinoma diagnosed from 2007 to 2015 were of small and very small size tumors (≤2 cm). Similarly, about 3-quarters are of early stages (T1 and T2) (Table 2).
Upon comparison between the 2 periods of the study, more papillary thyroid cancers were being diagnosed in the second period, from 2011 to 2015 (Table 2). The great majority of the increased cases in this period were also microcarcinomas (31.9%) and small cancers 1.1 to 2 cm (31.4%). However, the increased number has not been restricted to these groups. We also observed an increase in the number of all sizes of PTC, and the remaining cases were contributed by cancers of size >2 cm.
Regarding the stage of PTC, more than half of the overall increase in PTC was for localized stage tumors. However, we cannot ignore the almost similar increase in locally advanced regional stage tumors with minimal extra thyroid extension (T3) and/or lymph node metastasis. On the contrary, the more advanced T4 stage tumors constituted a very small percentage throughout our study and in both groups.
These results are similar to data from several studies that reported an increase in the diagnosis of small, early-stage, as well as larger regional stage tumors, as was found recently in a study from Iran and Canada.11,15 Recent studies from Poland and the Kingdom of Saudi Arabia reported an increase in both T1 stage tumors and tumors with regional lymph node metastasis.8,12
In addition, in keeping with our results, a study from USA spanning 8 decades, found a significant increase in the number of microcarcinomas (reaching 27%) and T1 tumors (reaching 49%) as well as larger tumors.20 Morris and Myssiorek also reported a significant increase in well-differentiated thyroid cancers >2 cm in size as well as larger tumors >4 cm in size.18
On the other hand, other published studies in the literature reported a higher percentage of papillary thyroid microcarcinomas, accounting for more than half of the cases in some studies.5,6,17,21,22 These reported that increased incidence of thyroid cancer is predominantly due to the increased detection of small papillary cancer and did not report increases in large thyroid cancers or late-stage cancers. They argued that the increased diagnosis of PTC is mostly an overdiagnosis of clinically silent, occult, and irrelevant microcarcinomas, which are considered in some studies as normal findings, placing the patient at risk of unnecessary surgical treatment and its harmful complications.23
Based on our results, we are facing an increase in small, subclinical, and early-stage tumors (constituting the great majority of cases) as well as larger and regional-stage tumors. Hence, there is no doubt that we have a problem of overdiagnosis due to the widespread use of improved disease detection methods such as imaging studies and fine-needle aspiration procedures, especially for tumors ≤10 mm. However, our observed trend cannot be totally explained by overdiagnosis. Apparently, this suggests that we are also facing a true increase in PTC. This increase cannot be explained by a single cause; it may be multifactorial.
The issue of overdiagnosis and over-detection of papillary thyroid carcinoma has long been a controversial subject in past years. Wider access to care and detection of occult tumors have been postulated as predominant influencing factors for this increase, especially in the concurrently unchanged mortality rates for this type of cancer and its favorable course.2,3-24-26
A claim of overdiagnosis has also been reported from follow-up and autopsy studies, which state a frequent finding of occult papillary thyroid carcinomas in at least one-third of adults with a variable frequency of 10–36% in thorough autopsy studies.17,26 Those would mostly not produce any harm or progression during adult life.21,27
Limitations of the study
Our study has some limitations. First, it only includes a subset of cases of thyroid cancer diagnosed in our country. However, both institutions from which cases were retrieved are considered 2 of the biggest institutions in our country; hence, they provide representative data on histological aspects of thyroid carcinoma. Second, it does not provide data about cases of papillary microcarcinoma that were diagnosed incidentally in thyroid glands removed for other benign causes; such data may have provided better insight into the overdiagnosis of occult, clinically irrelevant tumors.
In conclusion, our findings indicate that the current use of different diagnostic procedures, including ultrasound examination of the thyroid in addition to fine-needle aspiration of small tumors, cannot completely explain the observed increase in the frequency of papillary thyroid cancer.
Therefore, studies designed to investigate other risk factors for papillary thyroid cancer should be performed in the near future. Triage of patients with cancers needing surgical treatment is also suggested, not only to overcome unnecessary diagnosis but also unnecessary treatment in a fraction of patients.
Radiation exposure of the thyroid gland in children who are exposed to medical and dental radiation in the form of computed tomography scans, X-rays, and nuclear medicine examinations is suggested by some authors to be partly responsible for the development of thyroid cancer later in life, especially of microcarcinomas.4,28,29 The thyroid gland is highly sensitive to these types of medical radiation than any other body organ.29 We need studies to prove this association in the era of increased use of these radiologic modalities.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 10, 2017.
- Accepted December 18, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}