


Abstract
Objectives: To evaluate the surface roughness of 4 different bulk-fill resin-based composites cured using different irradiance levels.
Methods: This in vitro study was performed in February 2017 to August 2017 at the College of Dentistry, King Saud University. Twenty-four specimens were prepared from each of the bulk-fill materials [Tetric N-Ceram (TNC), SonicFill (SF), Smart Dentin Replacement (SDR), and Filtek Bulk-Fill (FB)] using a brass metal mold, resulting in a total of 96 specimens, cured using a Bluephase N light curing unit. Half of the total number of specimens (N=48) were cured using high-power irradiance (1200 mW/cm2) for 20 seconds, while the remaining half (N=48) were cured using low power irradiance (650 mW/cm2) for 40 seconds. After 24 hours, baseline surface roughness of each specimen was analyzed using a profilometer, then polished using Sof-lex abrasive disks, and the surface roughness of all groups was assessed.
Results: Post-polished SonicFill cured at high irradiance had the highest mean surface roughness (0.23±0.03), whereas pre-polished Smart Dentin Replacement (0.11±0.01) and SonicFill (0.11±0.02) cured at low irradiance had the lowest mean surface roughness.
Conclusion: High curing irradiance (1,200 mW/cm2) had no positive influence on the surface roughness of Filtek Bulk Fill and Tetric N-Ceram bulk-fill RBCs compared with lower curing irradiance (650 mW/cm2). However, the difference of curing irradiance significantly affected the surface roughness in SDR and sonic fill RBCs.
Improved esthetics and bonding to tooth structure and augmented mechanical properties have made the daily clinical use of resin-based composites (RBCs) more acceptable. Some drawbacks of these materials, such as polymerization shrinkage and water uptake on exposure to the oral environment, may weaken their mechanical properties.1 Failure of restorations may also be the result of a relatively poor wear resistance and curing procedures.2,3 Therefore an increase of surface wear may lead to an increase in surface roughness, resulting in plaque accumulation, gingival irritation, poor esthetics and recurrent caries.4,5 The surface smoothness and gloss of RBCs may also be negatively influenced by regular tooth brushing.6 Alternatively, inadequate irradiance (value) or insufficient time exposure of curing may lead to reduced degree of conversion (DC), hardness, strength, modulus of elasticity, wear resistance and increased cytotoxicity, marginal leakage and bond failure.7 Therefore, increasing the curing light irradiance may improve the degree of polymerization and curing depth and will require a shorter irradiation time.8 The emerging trend in using bulk-fill RBCs among dental practitioners has been reported due to its procedural simplicity. Many in vitro research has been conducted recently on the bulk-fill RBCs properties due to the deficiency of literature available on their clinical performance.9 A depth of cure in excess of 4 mm has been reported for bulk-fill composite materials, which may be due to enhanced light transmittance.10 The manufacturers claim that these restorative materials, which contain various modified resins and filler systems, have a clinical feel similar to that of amalgam in terms of condensability, hold shape, and occlusal and interproximal contours.11 Bulk-fill RBCs generally have increased filler size and decreased filler load, which enhances the depth of cure.12 The effects of irradiance time and the distance of the light tip on the micromechanical properties and the real-time increase of degree of cure of 2 bulk-fill RBCs (TetricEvo Ceram® Bulk Fill, Ivoclar-Vivadent and x-tra base, Voco) were assessed by Ilie et al.13 The authors concluded that both bulk-fill RBCs enabled at least 4-mm-thick increments to be cured in one step under clinically relevant curing conditions.14 Tarle et al15 assessed the influence of irradiation time on subsurface DC and microhardness of high viscosity bulk-fill RBCs (TetricEvo Ceram Bulk Fill, x-tra fil, QuixFil and SonicFill) and concluded that the tested bulk-fill RBCs could be safely used up to an incremental thickness of 4 mm considering the DC, but only x-tra fil and QuixFil achieved acceptable hardness at a 4-mm depth with 30 seconds of irradiation. A polywave light source with high irradiance (1,170 mW/cm2) was used in the study. The shape, type, size and inorganic filler distribution influences the surface roughness of RBCs.16,17 Increasing the filler content and decreasing the filler size decreases the surface roughness.18 Using a fine filler size causes a less interparticle spacing and filler plucking and provides protection of the softer resin matrix.16,19 At the interface during polishing, it is difficult to avoid irregularities between the resin and the filler particles due to their different levels of hardness.16 Another study found that the general effect of a finishing and polishing system on surface roughness is largely dependent on both the polishing system and the restorative material.20 Among the tested materials, Bulk Fill and nanohybrid resin composites exhibited the smoothest surfaces compared with nanoceramic and microhybrid resin composites after polishing.20 The present study was carried out to investigate the surface roughness of 4 different bulk-fill composite resin restorative materials cured using high-and low-power irradiance. The null hypothesis of this study is that there would be no significant difference in the surface roughness among the 4 bulk-fill RBCs using high- and low-power irradiance.
Methods
The present study was registered at and approved by the College of Dentistry Research Center (Registration number: FR 0379). The in vitro study commenced in February 2017 and finished in August 2017. The 4 bulk-fill RBC materials tested were Filtek Bulk Fill Posterior Restorative (3M ESPE, St. Paul, MN, USA), Tetric N-Ceram (Ivoclar Vivadent, Schaan/Liechtenstein), Smart Dental Replacement (Dentsply Caulk, Milford, USA) and SonicFill Nanohybrid Composite Restorative (Kerr Corporation, Orange, CA, USA). Twenty-four specimens were prepared from each of the bulk-fill RBC materials using a 2-part split brass metal mold with a diameter of 5 mm and a thickness of 4 mm, resulting in a total of 96 specimens. This design ensured a standard size and shape of each specimen. A clear Mylar strip (Mylar Uni-strip, Dentsply Caulk, Milford, USA) was placed on top of a clean glass slab, above which the split brass mold was placed, and a sufficient amount of RBC material was placed in a single increment into the mold using a plastic material and was then packed. Likewise, the upper surface of the RBC material was covered with a clear Mylar strip, and a 1-mm-thick glass slide was placed above and pressed gently to remove excess material in the mold. Mylar strips were placed on either side of the mold during the curing process to prevent formation of an oxygen-inhibited layer. All 96 specimens were cured using a Bluephase N light curing unit (Ivoclar Vivadent, Schaan/Liechtenstein). Half of the total number of each specimen (N=48) were cured using high irradiance (1200 mW/cm2) for 20 seconds, while the remaining half (N=48) were cured using low irradiance (650 mW/cm2) for 40 seconds. Irradiance values were measured using a Bluephase radiometer (Ivoclar-Vivadent, Schaan/Liechtenstein). The specimens were thereafter removed from the mold, and the bottom surface was marked with a permanent marker (Snowman, Japan) to facilitate identification.
Twelve specimens from each sub-group were subsequently placed in a lightproof container with distilled water and were stored in the incubator (Memmert Edestahl, Rostfrei, West Germany) at 37ºC and 100% relative humidity for 24 hours. After 24 hours, each specimen was mounted in an acrylic block to facilitate handling during polishing procedures, and the baseline surface roughness of each specimen, expressed as a µm Ra value, was analyzed using a profilometer (Contour GT-T, Bruker, Germany). After the initial reading was made, each specimen was polished using Sof-lex abrasive disks (ESPE Dental Products, St. Paul, MN, USA). Three grits, medium, fine and superfine, were used sequentially. All finishing and polishing procedures were accomplished with a low-speed handpiece (MF-Tectorque 9918, W&H Dentalwork GmbH, Austria) at 10,000 rpm for 10 seconds without water cooling, and each step was performed under mild uniform intermittent pressure in a circular pattern by one investigator. The specimens were thoroughly rinsed with distilled water and air-dried after use of each Sof-lex disk. The Sof-lex disks were discarded after use on each specimen. The final surface roughness was assessed using the profilometer.
The data obtained were analyzed using Statistical Package for the Social Science (SPSS) version 20 (IBM Corp., Armonk, NY, USA). The mean and standard deviation of surface roughness for each material before and after polishing were calculated and analyzed using one-way analysis of variance (ANOVA). Post hoc tests were performed for both multiple comparisons and independent specimens. The t-test was used for comparisons within each group. A p-value>0.05 was considered significant.
Results
The mean surface roughness of materials distributed according to curing irradiances and stages of polishing are given in Table 1. Post-polished SonicFill cured at high irradiance had the highest mean surface roughness (0.23±0.03), whereas pre-polished Smart Dentin Replacement (0.11±0.01) and SonicFill (0.11±0.02) cured at low irradiance had the lowest mean surface roughness. Furthermore, statistically significant differences in the mean surface roughness were observed for both high- and low-irradiance curing of Smart Dentin Replacement and SonicFill after polishing and then compared to those before polishing. However, these differences were not statistically significant for Filtek Bulk Fill and Tetric N-Ceram.
Mean surface roughness (µm) of materials distributed according to curing intensities and stages of polishing.
Considering the stage of polishing (post-polish/pre-polish) alone, a paired samples t-test revealed significant differences (p<0.001) in the mean surface roughness of Smart Dentin Replacement and SonicFill, whereas those of Filtek Bulk Fill (p=0.82) and Tetric N-Ceram (p=0.89) were not statistically significant. One-way ANOVA with a post hoc Turkey HSD (Honestly Significant Difference) test for multiple comparisons showed that, before polishing, the surface roughness of Tetric N-Ceram was significantly higher (p<0.05) than that of SonicFill. However, after polishing, the surface roughness of Smart Dentin Replacement (p<0.05) and SonicFill (p<0.001) were significantly higher than that of Filtek Bulk Fill.
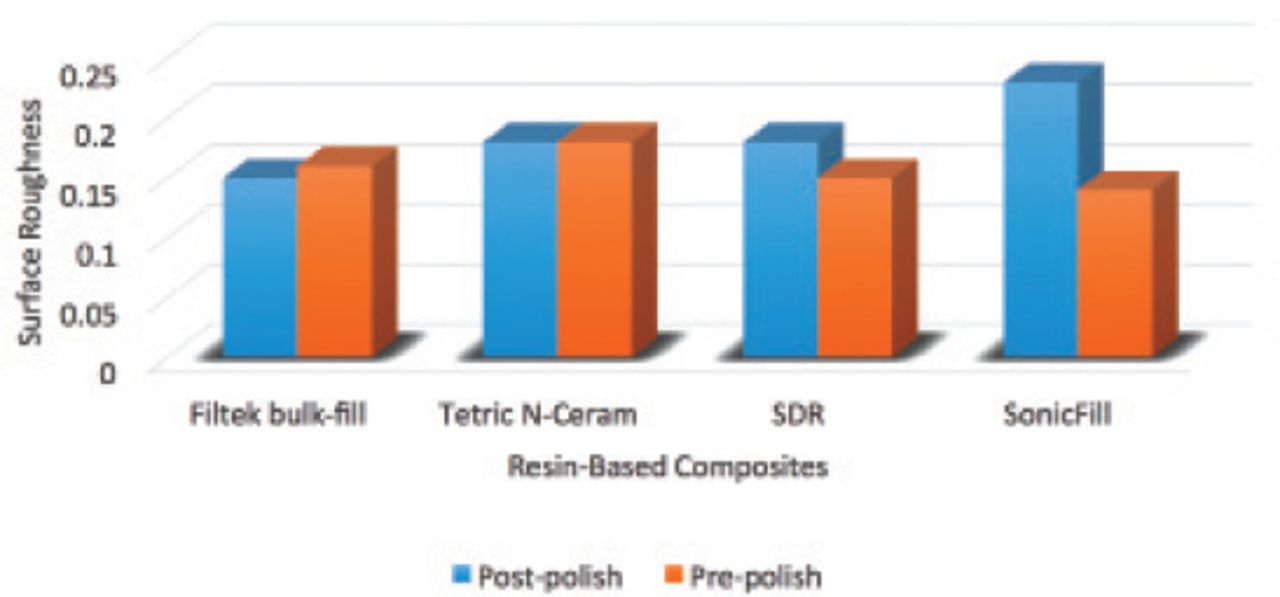
The results of one-way ANOVA with a post hoc Turkey HSD test for multiple significant differences in the surface roughness of materials cured using high irradiance after polishing were noted. The mean surface roughness of Smart Dentin Replacement was significantly higher than that of Filtek bulk-fill (p<0.05) and that of SonicFill was significantly higher those of Filtek bulk-fill (p<0.001), Tetric N-Ceram (p=0.001) and Smart Dentin Replacement (p=0.002) (Figure 1). However, materials cured using low irradiance showed no significant differences in the surface roughness either before or after polishing (Figure 2).
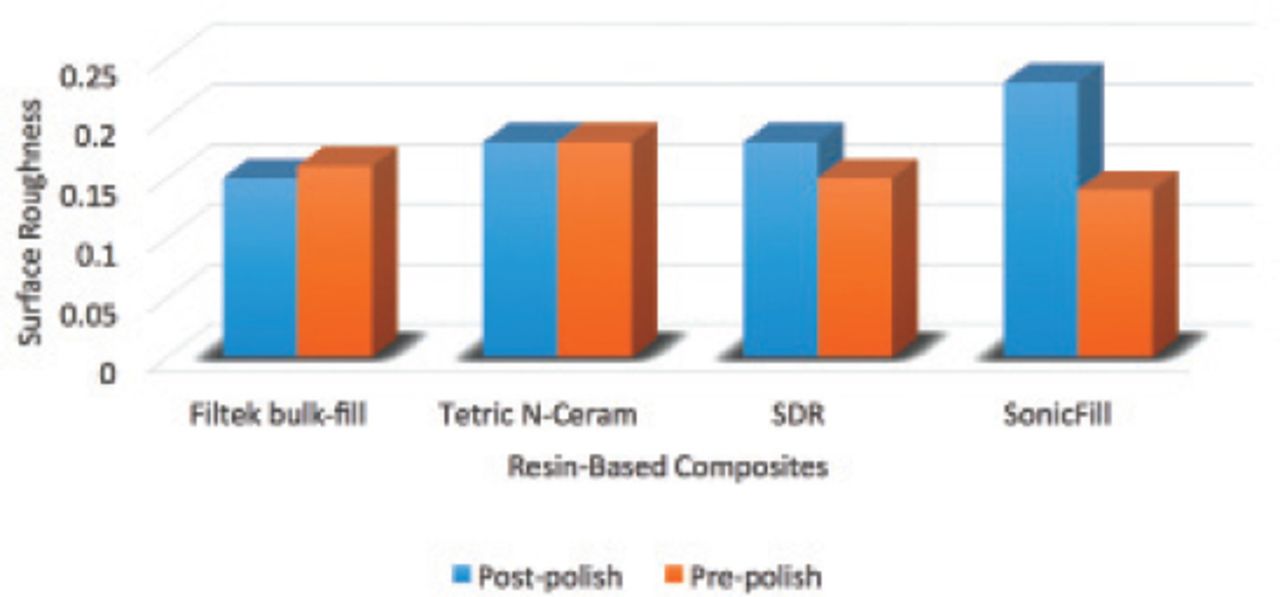
Graph showing the comparison of the materials using high light power irradiance.
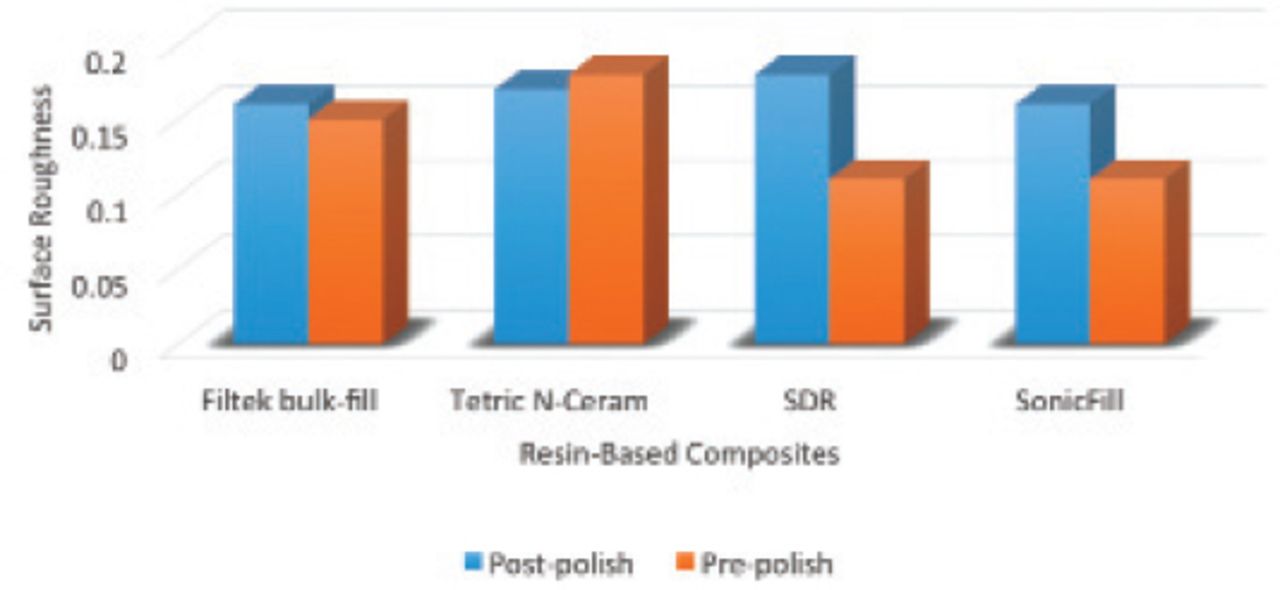
Graph showing the comparison of the materials using low light power irradiance.
Discussion
Bulk-fill RBCs may accomplish some significant requirements, such as low polymerization shrinkage, improved depth of cure, ease of use and enhanced physical properties.21 The physical properties of bulk-fill RBCs are particularly imperative since these materials may represent the majority of restorations.9 The surface roughness values of bulk-fill composite resin restorative materials, such as Filtek Bulk Fill, Tetric N-Ceram, Smart Dentin Replacement and SonicFill, were assessed in the present in vitro study.
A previous study was conducted to assess the wear resistance of the same 4 bulk-fill RBCs using high and low curing irradiances and found no positive influence between them.22 The study found that the most wear resistance material was SonicFill cured with low irradiance (650 mW/cm2) and the least wear resistant material tested was Tetric N-Ceram cured with high irradiance (1200 mW/cm2).
In another study on RBCs, Filtek Bulk Fill was found to be more resistant to wear and proved that there was a clear correlation between surface roughness and wear after simulated toothbrush abrasion of 50,000 cycles.23 The surface roughness may increase the coefficient of friction during mastication, oral habits or due to chemicals in the diet and the rate of wear.23 Rough surface can also predispose to accumulation of dental biofilms, residues, and stains leading to fading the gloss of the restoration, risk of secondary caries, gingival irritation and escalating discoloration and/or surface degradation.24
With regard to its mechanical properties, another study found that high curing irradiance (1200 mW/cm2) had a positive influence on the compressive and diametral tensile strength on the same bulk-fill RBCs and microhardness of the tested materials compared with low curing irradiance (650 mW/cm2).25 The highest compressive strength and microhardness was significantly found in SonicFill for high and low curing irradiances and greater diametral tensile strength with high curing irradiance but was not significant.25
The results of this in vitro study showed polished SonicFill cured at high irradiance had the highest mean surface roughness, whereas unpolished Smart Dentin Replacement and SonicFill cured at lower irradiance had the lowest mean surface roughness. Furthermore, high curing irradiance had a negative influence on the surface smoothness of Smart Dentin Replacement and SonicFill after polishing, whereas low curing irradiance had no significant influence on the surface roughness values of the tested materials either before or after polishing. The differences in the surface roughness among the materials tested may be due to the filler type, size, amount and type of resin; the surface roughness after polishing may also be due to the hardness of the abrasives used for polishing, the flexibility of the abrasive-embedded backing materials, the geometry of the polishing instruments and the type of instruments employed.26-28
The null hypothesis that there would be no significant difference in the surface roughness among the 4 bulk-fill RBCs using high- and low-power irradiance was accepted. Using higher curing irradiance (1200 mW/cm2) required lesser exposure time (20 seconds) while lower curing irradiance (650 mW/cm2) required longer exposure time (40 seconds). The curing irradiance and exposure time did not affect the quality of the bulk-fill RBCs in this study. Using high power irradiance offers convenience as it is less time consuming in the clinical practice. However, researchers have reported that lower curing irradiance produced restorations with better marginal integrity.29 It was also reported that a fixed amount of blue light energy can result in optimal clinical durability of RBCs rather than a high curing irradiance.30
Different methods were made to investigate how to increase the curing depth of RBCs. The curing depth may be increased by: 1) improving the absorption spectrum and the reactivity of the initiator, 2) optimizing the LED light source, or by 3) increasing the material’s translucency.31,32 Some intrinsic factors, such as ratio and co-monomer composition, size and content of the filler, and extrinsic factors, such as irradiance, irradiation time and light spectrum, should be considered while assessing the reactivities of photoinitiators.15 Third-generation LED curing units produce several wavelengths from a lone LED light, thereby attaining necessary peaks, acquire enough intensity and sufficient size and shape of the light probe. Furthermore, increasing the translucency of RBCs may lead to more photons that will penetrate the material’s deeper areas, thereby activating the initiator molecules.32 A reduced filler content combined with an increased filler size had a significant role in attaining the bulk-fill RBCs higher translucency.33 The values obtained from the present study were measured under ideal laboratory conditions, which may not be necessarily expected in clinical situations. The impact of each specific constituent of the bulk-fill RBCs on its properties is intricate to predict, as specific material compositions are mostly unknown.9
Periodontal and marginal integrity and wear of RBCs are influenced by finishing and polishing procedures, which contribute to the clinical longevity of restorations.34,35 Surface roughness of restorations may lead to plaque accumulation, surface discoloration and poor esthetics and is directly related to the restorative material and the polishing system used.36,37 Finishing procedures for restorations are mostly essential for contouring and removing excess, although they lead to increased surface roughness, which eventually necessitates polishing of the restoration.35 Borges et al who assessed the surface roughness of 4 packable RBCs and one microhybrid RBC after polishing with 4 different finishing and polishing systems, reported that the tested materials displayed variable surface roughness based on the polishing system used except for one material (Filtek P60), where comparable results were presented irrespective of the polishing system.37 Furthermore, Sof-Lex discs gave the smoothest polish for 4 out of 5 composites tested. A relatively smoother surface after polishing with Sof-lex discs may be due to the presence of aluminum oxide abrasive on a rigid matrix.38
In conclusions, within the limitations of this study, high curing irradiance (1,200 mW/cm2) had no positive influence on the surface roughness of Filtek Bulk Fill and Tetric N-Ceram bulk-fill RBCs compared with lower curing irradiance (650 mW/cm2). However, difference of curing irradiance significantly affected the surface roughness in SDR and Sonic materials. In addition, Sonic Fill cured at lower irradiance had the highest mean surface smoothness among the materials tested. High curing irradiance can be used to minimize curing time of composite restorative materials without jeopardizing the quality of the restoration
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research at King Saud University, Kingdom of Saudi Arabia, research project No. RGP-1438-028.
- Received October 9, 2017.
- Accepted January 17, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.