


Abstract
Objectives: To assess the effects of a technique of cup blocking screws combined with impaction bone grafting during total hip arthroplasty (THA) for patients with developmental dysplasia of the hip (DDH).
Methods: From August 2011 to July 2015, 53 patients (59 hips) with DDH in our hospital were treated with THA using the technique of cup blocking screws combined with impaction particulate bone grafting. These patients were prospectively followed, and the clinical and imaging results were collected.
Results: Harris hip score (HHS) was raised from 41.24 before surgery to 91.49 at the latest follow-up (p<0.001). Length discrepancy (LLD) was reduced from 28.97 mm before surgery to 6.08 mm after surgery (p<0.001). No loosening of the cup was detected at the last follow-up. The differences were insignificant in cup inclination and rate of cup coverage among the 3 groups of Crowe type II, type III, and type IV DDH (p>0.05).
Conclusion: The technique of cup blocking screws combined with impaction particulate bone grafting is simple and reliable, and it not only simplifies the attainment of initial stability, but also strengthens the mid-term to long-term stability during THA in DDH.
Bone defect on the superolateral border of the acetabulum is quite common in patients with developmental dysplasia of the hip (DDH).1 During total hip arthroplasty (THA), this defect often acts as the main challenge in obtaining the initial stability of the acetabular component.2 Additionally, without appropriate management, it may also undermine the mid-term to long-term stability of the cup. To resolve this problem, several methods have been developed, including shift-up of the rotational center, medialization of the rotational center, impaction particulate bone grafting, structural bone grafting, reinforcement rings and metal acetabular augments.3-9 The majority of the mild and moderate bone defects could be successfully treated by the first 2 methods. For severe defects, the other methods were often needed. Impaction particulate bone grafting is a frequently used method for the treatment of bone defects. However, it could only strengthen the mid-term to long-term stability and is of little help in the obtaining of initial stability. It still remains controversial regarding the application of structural bone grafting during THA in DDH, although it is helpful in the achievement of initial stability. Some studies reported satisfactory follow-up results, while others demonstrated that cup loosening was of high rate resulting from graft collapse or resorption.7,10,11 Several metal devices, such as reinforcement rings and acetabular augments, were reported to be helpful in facilitating the achievement of initial and mid-term to long-term stability; however, they could also increase the costs and complexity of the operation. To strengthen the initial stability, as well as the mid-term to long-term stability of the cup, the impaction particulate bone grafting was used in combination with a technique of cup blocking screws in our hospital. The main purpose of the present study was to introduce the clinical and imaging outcome of this technique during THA in DDH.
Methods
Study design and setting
In this prospective study, we followed 53 patients (59 hips) with DDH in our hospital who were treated with THA using the technique of cup blocking screws combined with impaction particulate bone grafting between August 2011 and July 2015. The average follow-up time of the patients was 4.62 years (2-6 years). Three patients (4 hips) were dead for reasons that were not related to operation. Another 9 cases (12 hips) were lost to follow-up. No signs of loosening was detected in these 12 patients until the latest follow-up. Therefore, there were 41 patients (43 hips) in all that were available for review. Patients’ demographic information is summarized in Table 1. Ethical approval was obtained from the review board in our hospital, and every patient had signed the informed consent. The research was carried out according to the Declaration of Helsinki.
Demographic data of 53 patients with developmental dysplasia of the hip treated with total hip arthroplasty using the technique of cup blocking screws combined with impaction particulate bone grafting.
Surgical procedure
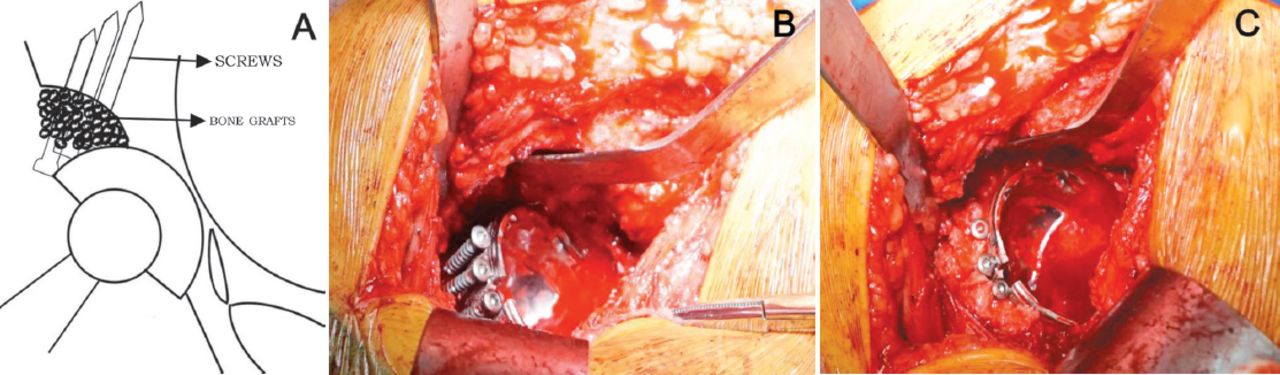
All operations were performed through posterolateral approach by the same Orthopedic Surgeon. The real acetabulum was firstly defined by the ischium, obturator, and pubis. To expose the acetabular medial wall and incisura acetabuli, soft tissue and bony layers had to be removed. The acetabulum was gradually prepared with acetabular reamer until the cartilage in the superior, anterior, posterior and medial walls of the acetabulum was removed. Remnants of cartilage in the inferior acetabular wall were allowed. Then, we evaluated the proportion of the bony coverage of the cup according to the last acetabular reamer. If the uncovered portion above the cup was more than 40%, the technique of cup blocking screws combined with impaction particulate bone grafting was used. Three to 4 screws were implanted in the area of bone defect close to the upper edge of the last reamer, which was kept in the acetabulum. Then, a cementless acetabular component was inserted, and the initial stability was assessed. The autogenous bone particles obtained from the patients’ femoral head were placed around the screws and impacted firmly (Figure 1). All of the femoral stems were also uncemented.

Technique of cup blocking screws combined with impaction particulate bone grafting: (A) Schematic diagram of the technique. (B) Three to four screws were implanted in the area of bone defect to strengthen the cup initial stability. (C) The autogenous bone particles harvested from femoral head were placed around the screws and impacted firmly to strengthen the midterm to long-term stability.
Perioperative management
Antibiotics were applied half an hour before skin incision and stopped 24 hours after operation. Enoxaparin was firstly administered 12 hours after operation for thromboembolic prophylaxis. All patients received the same procedure of perioperative pain management. With the help of crutches or walkers, we directed the patients to walk off the bed with touchdown weight-bearing from the second day postoperatively. The patients were allowed to walk with partial weight-bearing as tolerated until 4 weeks postoperatively, and then with full weight-bearing 8 weeks after operation.
Clinical and radiographic evaluation
Postoperatively, all patients were evaluated 6 weeks, 12 weeks, half a year, one year, and then annually thereafter. Length discrepancy (LLD) was recorded before and after the operation. Harris hip score (HHS) was recorded before surgery and at each follow-up postoperatively.12 A patient satisfaction scale was applied to assess patients’ satisfaction with the effect of THA.13 On the anteroposterior pelvic x-ray films, the inclination of the cup was determined by the interteardrop line and the face of the cup. The coverage rate of the cup was calculated with the methods introduced by Spangehl et al.11 Cup loosening was identified according to the standard introduced by Maruyama et al.14
Statistical analysis
Statistical analysis was performed with the Statistical Package for the Social Science (SPSS) version 23.0 (IBM Corp., Armonk, NY, USA). Preoperative and postoperative HHS and LLD were compared with paired-sample t-tests. Comparison of qualitative variables among groups was performed by one-way ANOVA with Bonferronni post-hoc test. Kruskal-Wallis test was performed to compare the cup coverage rate among the groups. p<0.05 was used to determine statistical significance.
Results
The mean HHS was raised from 41.24 (range, 21-60) preoperatively to 91.49 (range, 78-100) at the latest follow-up (p<0.001). The mean LLD was 28.97 mm (range, 0-50 mm) preoperatively, which was decreased to 6.08 mm (range, 0-11 mm) postoperatively (p<0.001). At the latest follow-up after surgery, no significant differences was detected in the aspect of HSS, LLD and satisfaction among patients with Crowe type II, type III, and type IV DDH(Table 2).
Comparison of clinical results among subgroups.
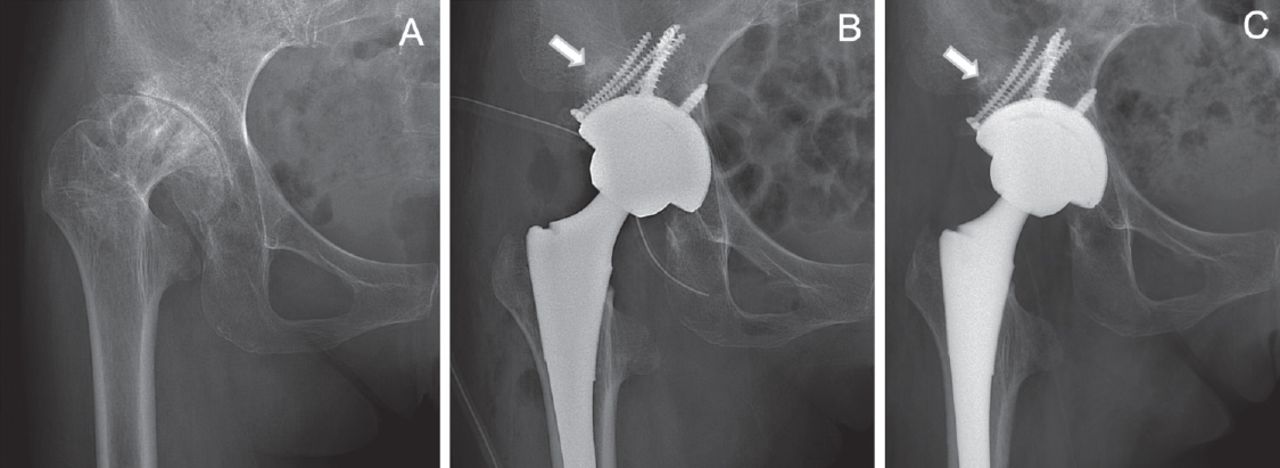
Posterior dislocation of the hip happened in one patient 2 months after operation when she tried to stand up from a low chair. We managed the dislocation by closed reduction under spinal anesthesia, and the hip abduction brace was applied for 1 month. The hip dislocation did not happen again. At last follow-up, no loosening of the cup was detected in any of the patients (Figure 2).

Radiographic evaluation: (A) Preoperative radiograph of a 53-year-old female patient with DDH. (B) Radiograph immediately after surgery. (C) Radiograph 3 years after operation. No signs of loosening was detected.
For patients with Crowe type II, type III, and type IV DDH, no significant differences were detected in the aspects of cup inclination, and rate of cup coverage (p>0.05). Patients in Crowe type IV group experienced more femoral head inferior shift (p<0.001) (Table 3).
Comparison of imaging results among subgroups.
Discussion
Owing to the bone defect often encountered, the most common difficulties often lie with acetabular reconstruction during THA for DDH, especially for patients with Crowe types III and IV DDH. Although it has been reported that most of the mild and moderate bone defects could be successfully treated by medialization of the rotational center, there has not been a consensus on the threshold of medial protrusion. Some reports proposed <45%, while others proposed <50% or even 60%.15-17 Excessive medialization will further undermine the bone stock of the acetabulum, which may worsen the complexity if a revision operation is needed in the future. In addition, there has also not been a consensus on the cup coverage rate of host bone to ensure the stability. The proposed uncovered portion of the cup ranged from ≤30% to ≤50%.18-21 Due to these uncertainties, it is often quite difficult for the surgeons to make sure if the initial stability of the cup is reliable enough and whether mid-term to long-term stability is guaranteed.
Bone grafting, including structural bone grafting and impaction bone grafting, is the most efficient method in improving the acetabular bone stock. Although structural bone grafting is helpful in obtaining the cup initial stability, it is reported that the effect of structural bone grafting on the mid-term to long-term stability is not always secured.22,23 We believe that structural bone grafting requires highly experienced surgeons who should be quite skillful in the grafts preparation and fixation.24 Additionally, the surface of the bone defect should also be carefully prepared by drilling and roughening to promote vascularization. In contrast to structural bone grafting, favorable mid-term to long-term effects of impaction bone grafting have been reported in the treatment of bone defects during THA for DDH.6,25 However, impaction bone grafting is not helpful in the achievement of the initial stability of the cup. To overcome this weakness, we tried to apply impaction bone grafting in combination with cup blocking screws. Under the help of cup blocking screws, we obtained the cup initial stability without significant difficulties in all the patients during this study. At the last follow-up, all of the cups demonstrated satisfactory coverage and inclination degrees. No loosening of the cup was detected.
We have summarized 3 recommendations regarding the technique of cup blocking screws combined with impaction bone grafting: 1) 3-4 screws are recommended to be implanted. Too many screws may further undermine the dome of the acetabulum, while too few screws may not provide enough support; 2) The screws should be implanted closely to the upper edge of the last reamer, and the reamer should be kept at the position of 40° of abduction and 10° of anteversion; 3) Before impaction bone grafting, the surface of the bone defect should be carefully prepared by drilling and roughening.
Study limitation
First, the sample size was small. Second, only one type of cup was used in the present research, and thus it may lead to certain bias. Third, patients included in this research were all Chinese with lower body weight in comparison with people in western countries, which may be one of the reasons why the screws could provide enough support for the cup.
In conclusion, the technique of cup blocking screws combined with impaction bone grafting is simple and reliable, which is not only helpful in obtaining initial cup stability but also in strengthening mid-term to long-term stability during THA for DDH. Nonetheless, further studies on this technique with larger sample sizes are needed.
Acknowledgment
The authors gratefully acknowledge the radiologists, Professor Jinxiong Zhang and Dr. Lilei Yi, for their assistance in reviewing the x-ray films.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 14, 2017.
- Accepted February 14, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.