


Abstract
Objectives: To observe the frequency of eosinophilic esophagitis (EoE), pattern of clinical presentation and diagnosis among Saudi children at 2 tertiary care hospitals in Riyadh, Saudi Arabia.
Methods: The database of children admitted or seen, and aged less than 18 years over 5 years period and diagnosed with EoE was collected and reviewed. Patients with esophagitis other than EoE were excluded. Patients who had eosinophils count more than 15/high power field (HPF) on esophageal biopsies were given the diagnosis of EoE. Demographic database, clinical parameters, and diagnostic modalities were analyzed by using the Statistical Package for Social Sciences version 22.
Results: A total of 37 children with the diagnosis of EoE were gathered from 398 upper gastrointestinal endoscopic procedures with the frequency of 9.3%. There were 22 (59.4%) males with a mean±SD age of 9.6±2.3 years and all were Saudi nationals. Dysphagia was the leading presentation in 21 (56.7%) children followed by vomiting in 18 (48.6%), impaction of food bolus in 8 (21.6%) and foreign body in 3 (8.1%). Allergic symptoms were present in 13 (35.1%) children in the form of asthma, 11 (29.7%) multiple food allergies and 5 (13.5%) eczema. Peripheral eosinophil count and immunoglobulin E were raised more than normal in 6 and 5 children respectively. The pH measurements were carried out in 16 (43.2%) and ruled out the reflux. Contrast studies with barium (n=6; 16.2%) and endoscopic findings were significant (n=27; 72.9%).
Conclusion: Eosinophilic esophagitis is an emerging disease and have a rising trend in Saudi children. Dysphagia, vomiting, and food impaction are the more common presenting features in older children and recurrent vomiting in younger children in addition to associated allergic conditions.
Eosinophilic esophagitis (EoE) is an inflammatory condition of esophagus with underlying immune mediated mechanism. Constant antigens exposure in a susceptible child will lead to induction of eosinophils in the esophageal mucosa and development of tissue damage and chronic inflammation along with fibrosis over time.1,2 Eosinophilic esophagitis is a clinico-pathological diagnosis with the presence of eosinophils more than 15/high power field (HPF) in esophageal biopsies taken from more than one locations.1 Eosinophilic esophagitis is on the rise and more children and adolescent are diagnosed due to heighten awareness or actual increase in the incidence still is uncertain.3 Eosinophilic esophagitis is less common in females without clear understanding.4,5
There are no specific clinical parameters which clearly pinpoint the diagnosis of EoE and thus many of these patients initially being treated as gastroesophageal reflux disease (GERD).6 Older children usually present with dysphagia, food impaction, and retrosternal pain whereas infants and toddlers usually present with feeding difficulty, vomiting, choking with meals and less commonly with failure to thrive.6,7 Physical examination is usually unremarkable except in younger children who can be failure to thrive because of feeding difficulties and vomiting. Gastroesophageal reflux disease and infective esophagitis are 2 major differentials of EoE which has almost same mode of presentation and earlier recognition deems necessary to avoid morbidities.3,6,7 Eosinophilic esophagitis has strong associations with allergic conditions such as food allergies, asthma, allergic rhinitis, eczema, and some other conditions like celiac disease, schatzki ring, and inflammatory bowel disease (IBD).6,8,9
Diagnosis of EoE mainly rest on clinical, endoscopic findings, and histopathology. Endoscopy should be considered after a trial of acid suppression therapy for at least 4-6 weeks. Endoscopic findings include ringed or circular appearance, linear furrows, white patches and stricture formation.9,10 Histopathology shows significant mucosal infiltration with eosinophils and is a hallmark of the disease, though eosinophils can be found in other conditions like GERD, but generally with a lower count <10/HPF. It is also important while taking the biopsies to include proximal, middle, and lower esophagus in addition to gastric and duodenal biopsies which should be normal as this is restricted to the esophagus only.11 Other supportive diagnostic modalities include barium contrast, total immunoglobulin E (IgE) level, and peripheral eosinophilia. Blood tests include total IgE level and presence of peripheral eosinophilia which is usually mild also supports EoE.6 Assessment by an allergist/immunologist is also suggested because of strong association with allergies.12
In the present study, we reported our experience from central region of Saudi Arabia (from 2 centers) about the rising trend of EoE, clinical presentation, and diagnostic modalities.
Methods
It was a retrospective, cross sectional study conducted at the Department of Pediatrics from 2 tertiary care hospitals, one public (King Khalid University Hospital) and other private setting (Dr. Suleman Alhabib Medical Center). The data base of children admitted or seen during the period from January 2010 to January 2015 from these hospitals and diagnosed as EoE was collected and reviewed. These were the absolute number of patients with the diagnosis of EoE over these years of data collection to know what could be the trend in Saudi children in hospital settings. The database was searched with the key words of eosinophilic esophagitis, dysphagia (description of dysphagia revealed difficulty swallowing solids and impaction of food in the center requiring some fluid to push it down and sometime feel comfortable by vomiting), vomiting, hematemesis, food impaction and esophageal strictures from the endoscopy procedure software, inpatient and out patient’s records. As the clinical presentation of GERD overlaps with EoE only those patients were enrolled in the study who underwent endoscopy and had eosinophils count more than 15/HPF on multiple esophageal biopsies. We included children below 18 years of age of both sexes and who had not responded to conventional course of proton pump inhibitor (PPI) previously for 4-6 weeks or negative pH studies (if done) and underwent endoscopic procedure. The children were divided into 3 age groups for data collection, younger than 5 years, 5-10 years and older than 10 years. Demographic database, clinical parameters (presentation and physical examination), blood tests and imaging studies, pH studies (if done) and endoscopic findings were recorded. Patients with esophagitis other than EoE were excluded such as reflux esophagitis, infectious esophagitis and structural causes other than eosinophilic stricture. Also excluded the associated conditions in these children were helicobacter pylori infection, celiac disease, and IBD.
Statistical analysis was carried out by using the Statistical Package for Social Sciences version 22 (SPSS Inc., Chicago, IL, USA). Categorical data were summarized as number and percentages whereas continuous data were summarized as mean, median, standard deviation (SD), and range. Comparison between groups for categorical variables was carried out using Chi-square test or Fisher’s exact test whereas for continuous data student t-test or Mann Whiteny U test were used. A p-value less than 0.05 was considered significant where applicable. This study was approved by the Hospital Internal Review Board and conducted according to the principles of the Helsinki Declaration.
Results
A total of 37 children met the inclusion criteria with confirmed EoE based on clinical parameters, endoscopic findings, and eosinophils count more than 15 /HPF on esophageal biopsies from different regions. These children were gathered out of 398 upper gastrointestinal endoscopic procedures with the frequency of 9.29% carried out for various indications such as dysphagia, food impaction, vomiting, hematemesis, feeding refusal, and chocking. There were 22 (59.4%) males with a mean±SD age of 9.6±2.3 years and all were Saudi nationals. There was a clear rising trend seen over these years (Figure 1). Dysphagia was the leading presentation in 21 (56.7%) children followed by vomiting in 18 (48.6%). Older children (>10 years age group) had dysphagia and recurrent vomiting in other groups as a presentation with a significant p-value of <0.001. Impaction of food bolus in 8 (21.6%) and foreign body in 3 (8.1%). Recurrent vomiting were more predominant symptoms among the infants and younger children with a p-value of <0.001. Allergic symptoms were present in children with asthma (n=13; 35.1%), multiple food allergies (n=11; 29.7%) and eczema (n=5; 13.5%). Physical examination was unremarkable in all the children except 4 (10.8%) who were growth retarded. Summary of demographic and clinical characteristics of EoE patients are summarized in Table 1.

The figure shows the rising trend of EoE patients over the years.
Summary of demographic, clinical and diagnostic characteristics of 37 pediatric patients with eosinophilic esophagitis (EoE) from Saudi Arabia.
Eleven children (29.7%) had raised than normal peripheral eosinophil counts (n=6) and immunoglobulins E (n=5). The pH measurements were carried out in 16 (43.2%) and ruled out the reflux. Contrast studies with barium was abnormal in 6 (16.2%) children and confirmed on endoscopy as stricture formation, one child was less than 5 years, 4 children were between 5-10 years, and one older than 10 years of age. Endoscopic findings were significant in the form of ringed appearance, linear furrows, sloughing with white exudates in 27 (72.9%) patients. Histopathology confirmed eosinophilic esophagitis in all children as reported eosinophils more than 20/HPF (Figures 2A & 2B). Summary of endoscopic and abnormal histopathology is given in Table 1 and detailed description is summarized in Table 2.
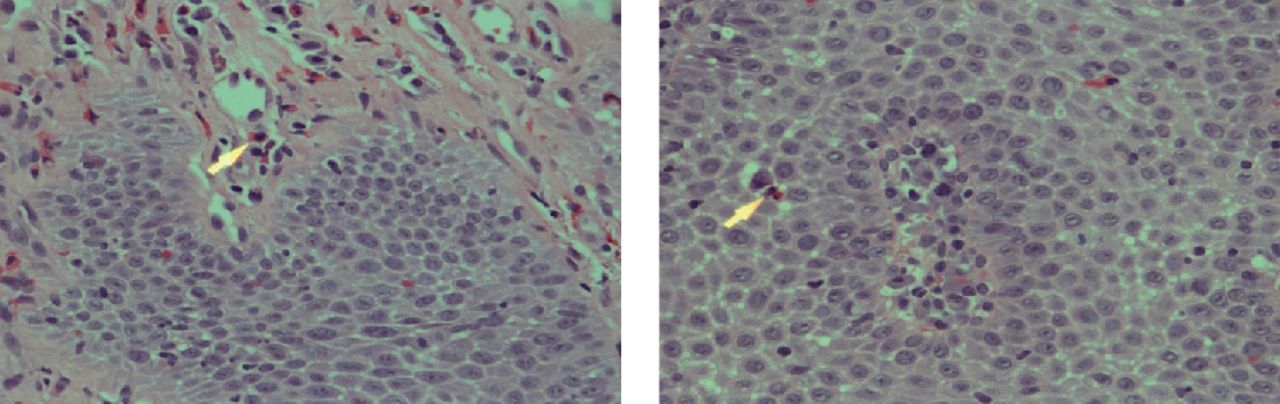
Esophageal squamous mucosa infiltrated by eosinophils (arrowhead) with the presence of significant intercellular edema. B) shows the presence of many eosinophils in the submucosal layer. Hematoxylin and Eosin (H/E) stained x 400.
Endoscopic and histopathology features of 37 pediatric patients with eosinophilic esophagitis (EoE) from Saudi Arabia.
Discussion
Eosinophilic esophagitis is not an uncommon entity in children and more recognition being made in the recent years because of rising trend. The exact prevalence is not known in Saudi Arabia, but literature showed it is not rare in this part of the world.6,13,14 The rising trend in EoE in Saudi children might be associated with more westernized food consumption as compared to conventional Saudi diet. With the consumption of more westernized food, there was an associated rise of allergic conditions like bronchial asthma in the urban areas of Saudi Arabia.13,14 In this study, the trend was observed during the study period (Figure 1). Eosinophilic esophagitis is more common in male gender without any clear reasons.15 Male out numbered female clearly in this study, which is consistent with the international literature though the p-value was not significant. Duration of illness before presentation is also an important prognostic indicator in these children. Commonly these children get antireflux and prokinetic medications before diagnosis of this important entity being treated as GERD.6,16 Our children also had history of PPI (67.5%) and few also had taken antacids/prokinetic medications, but without any good response. The clinical presentation of EoE is age dependent and all age groups are affected.17 Dysphagia, feeling of food stuck in the center of chest, and food impaction are the major clinical presentation in children and adolescent.18,19 Younger children and infants have recurrent vomiting or refusal to feed/ choking and failure to thrive may be the physical findings. Hematemesis is an unusual presentation but reported.20 In this study, older children and adolescent presented with dysphagia and food impaction while younger children had vomiting as prominent feature and few of our children also had failure to thrive on physical findings. Two of our children had hematemesis as clinical presentation. The major different of EoE were GERD and infective esophagitis. As symptoms of both EoE and GERD overlaps, high index of suspicion needs to be kept. The pH measurements and non-responders to acid suppression medication for reflux like symptoms may be considered to rule out EoE. For infective esophagitis, endoscopic assessment will be important modality in ruling out.20,21 The present study group was of those who had no response to conventional acid suppression therapy or had normal pH measurement and moreover all children underwent endoscopic assessment with biopsies and GERD and infective pathologies were ruled out.
Eosinophilic esophagitis has strong associations with other allergic disorders such as bronchial asthma, allergic rhinitis, atopic dermatitis, and food allergies. The most common associated condition is bronchial asthma (35%) followed by allergic rhinitis and skin conditions.3,22 Our children showed almost the same trend with bronchial asthma followed by multiple food allergies and skin condition but none of the children had allergic rhinitis. Due to overlapping symptomatology between GERD and EoE, response to trial of PPI for 4-6 weeks or pH measurement will provide clear direction to proceed to endoscopic examination.17,23 In this study, 25 children were given trial of PPI and 16 had additional pH measurements. Barium contrast studies helps in identifying any stricture formation in these children due to EoE.24 Blood tests include total IgE level which is usually elevated in 50-60% of patients with EoE. Presence of peripheral eosinophilia which is usually mild also supports EoE and evident in about 40-50% patients.3,22 Current study showed abnormal barium contrast study in 6 children and IgE/peripheral eosinophilia in 11. Endoscopy sometime gives classical picture like ringed appearance or linear furrows while white exudates needs to be differentiated from esophageal candidiasis. Other endoscopic findings include loss of vascular pattern, crepe paper appearance, and stricture formation. Normal endoscopic appearance does not rule out EoE.24-26 In this study, the most common endoscopic findings were loss of vascular pattern followed by white exudates, linear furrows and ringed appearance. In addition, 6 children had esophageal stricture. Endoscopic ultrasound may be helpful in measuring esophageal wall thickness, but not very popular in pediatric practice.25,27 The confirmed diagnosis of EoE is by histological examination of esophageal biopsies from different parts and documenting eosinophils >15/HPF in addition to the clinical manifestations and endoscopic appearance. Antral and small bowel biopsies should exclude other conditions such as celiac disease, IBD, and eosinophilic gastroenteritis.26,28 In the present study, all patients had eosinophil count more than 15/HPF and associated conditions were also excluded by antral and small bowel biopsies. Additional histopathological findings favoring EoE include basal cell hyperplasia, lamina propria fibrosis with elongation, eosinophil microabscesses, eosinophil degranulation, ulceration, and intercellular edema similar to our study.10,28,29
Study limitations
This study includes its retrospective nature so the potential of missing the data could not be ruled out. The sample size was small as it was collected from 2 tertiary care centers and result may not be standardized for all the settings. More prospective studies with larger sample size are required to depict the frequency of this emerging and important disease for better management and outcome.
In conclusion, EoE is not an uncommon entity in Saudi children and trend is on the rise. The recurrent vomiting, refusal to feed, and failure to thrive in younger children and dysphagia and food impaction in older children and adolescents needs consideration for eosinophilic esophagitis to be ruled out. Frequently associated allergic conditions should also point to investigate for this important and rising entity for possible earlier management to avoid long term morbidity.
Acknowledgment
This study was supported by the Prince Abdullah Bin Khalid Celiac Disease Research Chair, Vice Deanship of Research Chairs, King Saud University, Riyadh, Kingdom of Saudi Arabia. Authors would like to thank Editage, Cactus professional English editing company for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This study was supported by the Prince Abdullah Bin Khalid Celiac Disease Research Chair, Vice Deanship of Research Chairs, King Saud University, Riyadh, Kingdom of Saudi Arabia. (Grant # AB-89754).
- Received May 25, 2018.
- Accepted June 11, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.