


Abstract
Objectives: To study auditory temporal resolution skills using adaptive auditory tasks designed with a computer-based experimental program, and to provide normative values for gap detection thresholds (GDTs) of young listeners in 3 listening conditions.
Methods: The GDTs were established under 3 stimulus conditions: 1) broadband noise (BBN), 2) narrowband noise within-channel (NBN WC) using similar leading and trailing markers centered at 1.0 KHz, and 3) narrowband noise across-channel (NBN AC) with the leading marker centered at 2.0 KHz and the trailing marker centered at 1.0 KHz. In within-subjects design, the GDTs were obtained from 27 normal hearing young Saudi adults at Speech and Hearing Laboratories, Department of Rehabilitation Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia between April 2017 and April 2018.
Results: The mean GDTs for the BBN condition was 3.19 millisecsond (msec), NBN WC was 14.53 msec, and NBN AC was 29.71 msec. Our findings for the GDTs measured in the 3 conditions were consistent with those of earlier investigations that used different instrumentations. Also, no correlations among the GDTs of the 3 stimulus conditions were found.
Conclusion: The present study showed that experimental program is a reliable tool with clinical potential to estimate GDTs across different conditions. Also, the findings of no correlations in the GDTs across stimulus conditions suggest that different processes were involved in the perception of the temporal gap for different stimulus conditions.
For a listener, a clear understanding of speech requires many intact auditory processes. Study has shown that temporal processing skills, the regulation and monitoring of changes in sound energy over time, are essential to this understanding. Auditory temporal processing is classified into different categories or abilities, such as temporal integration (summation of energy over time), temporal discrimination (differentiating 2 acoustic events solely by duration), temporal masking (the effect of the decreased audibility of a sound due to a preceding or following sound), temporal ordering (perception fluctuations in intensity and frequency over time), and temporal resolution/acuity (recognition of temporal cues in acoustic energy as the means to differentiate acoustic signals).1 With regard to measuring temporal resolution/acuity, extensive studies have reported on temporal gap detection, duration discrimination, temporal integration, and temporal modulation transfer functions.2 Scholars have used different procedures to investigate these abilities, such as adaptive tests of temporal resolution,3 gap-in-noise (GIN) test,4 random gap detection test,5 and gap detection testing using MATLAB, MathWorks, Inc. (The Math Works, Natick, MA, USA). Perceptual deficits in temporal resolution skills or other central auditory processing skills such as sound localization, lateralization, and discrimination may cause central auditory processing disorder (CAPD).1 Temporal gap test is one of the clinical test battery for diagnosing CAPD. The present study reports Saudi data on gap detection thresholds (GDTs) by using a Windows-based psychoacoustic experiment program named Psycon developed by Kwon.6
The GDT is a temporal gap detection test involves determining the minimum silence duration embedded in a signal that can be detected by a listener. Extensive study was conducted to identify the GDT for broadband noise (BBN) and narrowband noise (NBN). Measurements of the GDT using NBN sounds are commonly carried out using within-channel (WC) gap detection (similar markers before and after the gap) or across-channel (AC) gap detection (dissimilar leading and trailing markers before and after the gap). Studies on gap detection with normal hearing adult listeners have shown that the lowest gap duration that has been detected for BBN sound was in the range of 2 to 5 millisecond (msec).7-10 High GDTs have been reported using NBN sounds in the range of 3 to 7 msec for the WC paradigm.8,10,11 Also, the gap detection performance for WC testing varies as a function of frequency. For example, Florentine et al12 have found psychometric functions for gap detection using band pass noises with center frequencies between 0.25 KHz to 8.0 KHz. Their results suggest that the GDT varied between 4.6 msec for 8.0 KHz band pass noise to 88.1 msec for 0.25 KHz band pass noise. Furthermore, the study consistently reported a higher GDT when using an AC gap detection paradigm.10,11,13-17 For example, Florentine et al16 reported a GDT of approximately 40-42.6 msec for AC NBN 2-1 KHz msec for young adults with normal hearing.
Lister et al3 have proposed a gap detection test that uses a computerized software application named adaptive tests of temporal resolution (ATTR). The experimental procedures of ATTR were applied into more clinically used procedures for determining the GDT.8,10,11 The ATTR software requires a computer with a sound card. It uses sets of stimuli that are stored offline as a waveform audio file format with fixed silence intervals.10 In addition, the experimental procedures are pre-determined in the ATTR platform with limited flexibility to investigate the cause and effect relation of stimulus-related parameters. As an alternative to ATTR, Kwon6 has described an independent scripting language device called auditory syntax (AUX) that was developed to generate and process audio signals using relatively simple codes and could be used as experimental platform for temporal gap detection tasks. The scripting application software package includes details for writing scripts to create psycho-perceptual tasks. In addition, Kwon6 designed a Windows-based psychoacoustic experiment program named Psycon that uses these AUX scripting syntax to create and process auditory signals. There is a need to explore such computer applications for their feasibility and reliability for assessing gap detection abilities, and for their clinical utility.
The aim the study is to describe the procedures for determining temporal resolution tasks using a Windows-based psychoacoustic experiment program named Psycon as described by Kwon.6 Psycon (Version 2.18) manipulates complex signal parameters in a relatively easy manner, and to systematically observe cause and effect relations in a consistent manner. The present study has used the clinical potential of Psycon to establish the normative values for the GDTs of normal hearing listeners both within and across a channel paradigm.
Methods
Twenty-seven native Arabic male speakers with normal hearing sensitivity volunteered to participate in the study. We used within-subject study experimental design in which all participants performed all experimental conditions. We screened all participants for normal hearing abilities based on an inclusion criteria of air conduction pure tone thresholds less than or equal to 15 dB (for octave frequencies between 0.25 to 8.0 KHz). All participants had normal findings on an otoscopic examination, and A/As tympanograms with acoustics reflex present at 90 dB HL. All participants were undergraduate students from the College of Applied Medical Sciences, King Saud University, Riydah, KSA and they were blinded to the procedure used in the study. The ages of the participants ranged from 21.08 to 24.44 years (22.21+0.73). The case histories of all the participants included in the study-regarding their history of middle ear infection, cognitive illness, head trauma, or noise exposure-were unremarkable. All the experimental procedures were carried out at the speech and hearing laboratories, Department of Rehabilitation Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, KSA between April 2017 to April 2018. All the study procedures followed the ethical guidelines of the Research Ethics Committee of the College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia.
A 2 channel diagnostic audiometer (Grason Stadler GSI-61TM (GSI-61TM, Eden Prairie, Minnesota, USA) for hearing assessment and to route the stimuli in the experimental procedures were used. Supra-aural headphones TDH-50P with a mod 51 ear cushion were used to deliver the stimuli for the study. A clinical otoscope and calibrated GSI-Tympstar were used to assess the participants’ middle ear functions prior to their participation in the experiment. All the procedures were carried out in the subject room of an audiometric test booth (model: RS142 acoustic systems). Psycon (Version 2.18) was used to generate the desired experimental stimulus and to collect the participants’ responses.6 Psycon is a Windows-based psychoacoustic experimental program available under Academic Free License 3.0. The program was operated by using commands scripted with the auditory syntax (AUX) detailed in the program manual. We installed and ran the program distributed under the Academic Free License (Version 3.0) on a Hawlett-Packard Compaq nx7300 laptop with a standard built-in sound card (Intel).
All the gap detection measures required the participant to listen to 2 stimuli presented successively; a standard (no-gap) stimulus and an adjustable (gap-in) stimulus. A sampling frequency of 44.1 KHz and an amplitude factor of -5dB (to avoid distortion at peak level) was used to generate all the stimuli. We presented the stimuli monaurally and at a constant level of 60 dB HL (volume unit meter was set to 0). The desired stimulus under 3 categories: BBN GDT, NBN WC GDT, and NBN AC GDT were generated.
To measure the GDT using BBN, the Gaussian noise was used without any edge filters. Both the standard and adjustable stimuli under BBN GDT were 500 msec with a 10-msec rise time at the start of the signal and a 10-msec fall time at the end of the signal. The gap (silence) duration around the center of the signal (silence inserted around 250 msec) were symmetrically inserted and maintained the total signal duration as 500 msec. Spectrograms of the no-gap stimulus and the gap-in stimulus with a 30 msec silence interval are represented in Figure 1. The adjustable stimulus depicted in Figure 1 illustrate that the gap duration was from 235 msec to 265 msec (symmetrical around 250 msec). Figure 2 depicts the long-term average spectrum of the signals generated for BBN GDT. All the spectrograms and long-term average spectrum measures were obtained through Praat Version 6.0.14.18
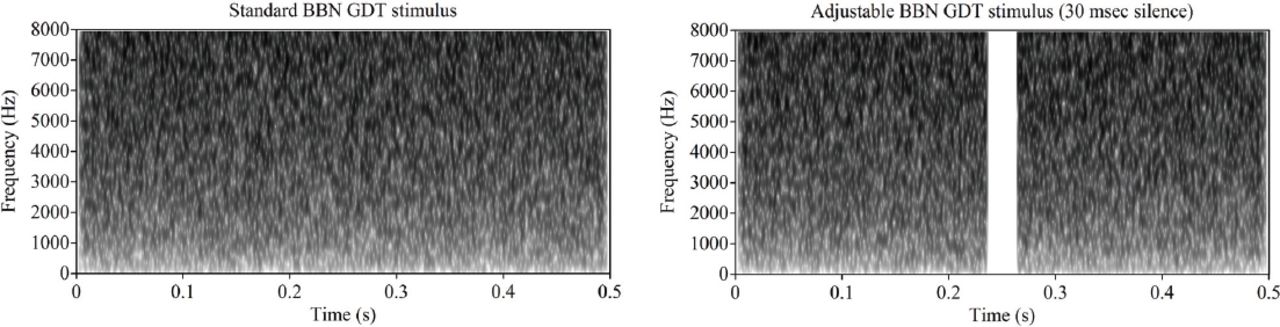
Spectrograms for no-gap stimulus (left side) and the gap-in stimulus. As an example a 30 msec silence interval was illustrated in gap-in stimulus (right side). BBN - broadband noise, GDT - gap detection thresholds
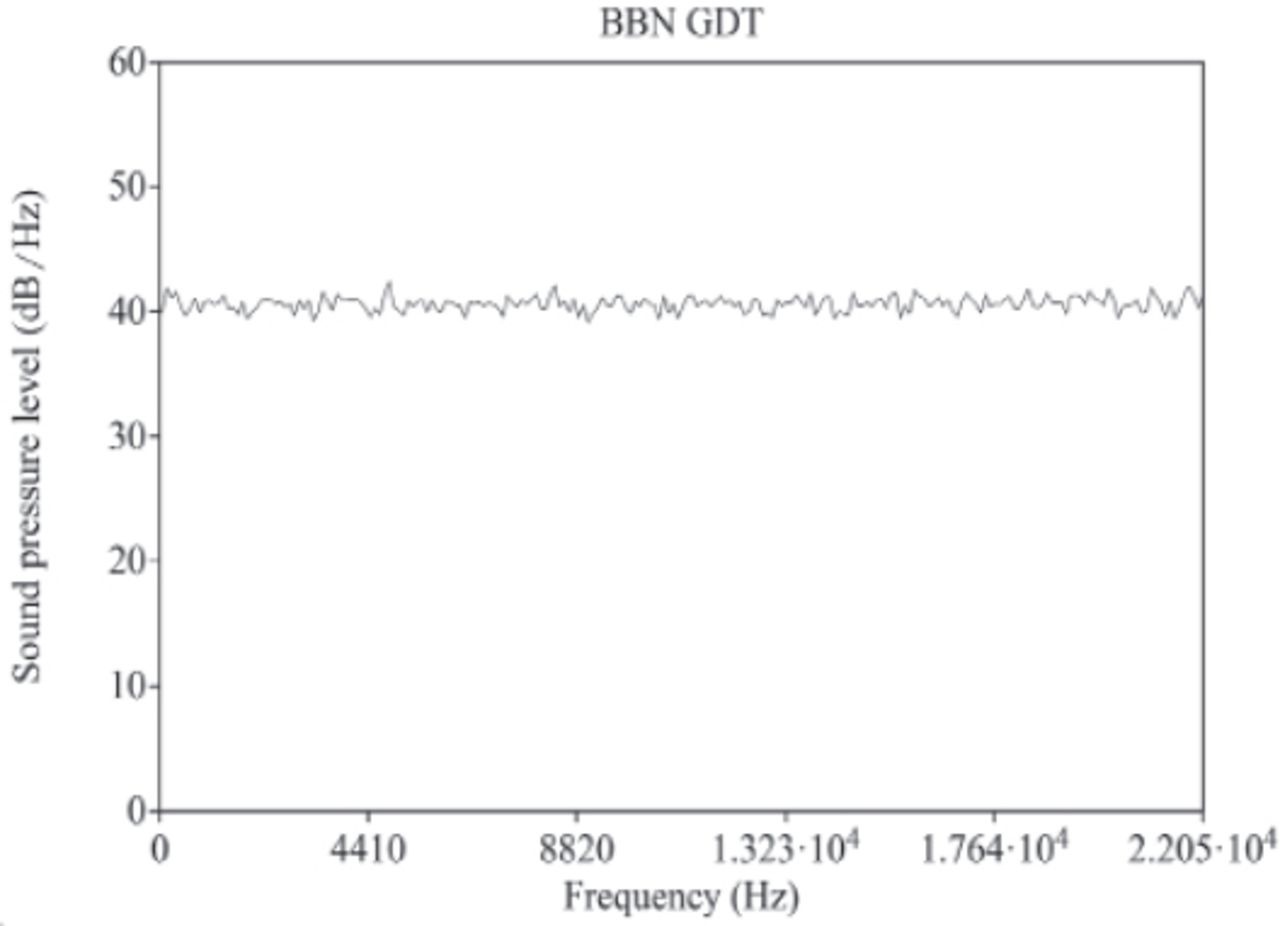
Long-term average spectrum of the broad band noise used for estimation of gap detection threshold (BBN GDT) stimulus. Hz = hertz and dB = decibels.
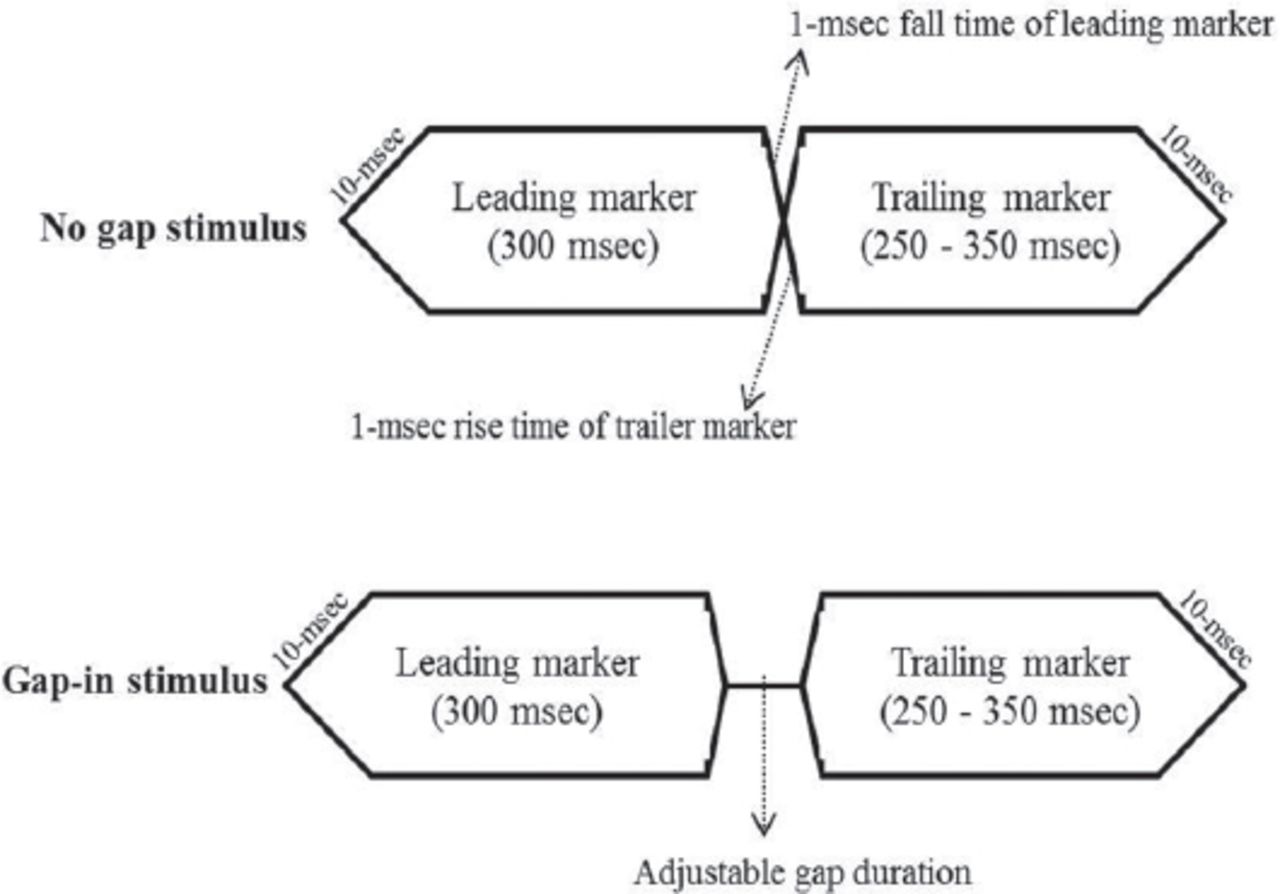
The NBN WC GDT and NBN AC GDT gap detection measures, narrow band noises were instantly generated from Gaussian noise with each 1/4th octave bandwidth and frequency geometrically centered at 1.0 KHz or 2.0 KHz with an 8th order Butterworth filter (pass band ripple as 0.5dB and stop band attenuation -40dB). Both the leading (before the gap) and trailer (after the gap) markers were 1.0 KHz centered NBN in all stimuli of the NBN WC GDT, and for NBN AC GDT, the leading marker was always 2.0 KHz centered NBN, and trailer marker was 1.0 KHz centered NBN. The duration of the leading marker was always constant at 300 msec, and the duration of the and the duration of the trailing marker varied randomly between 250 to 350 msec per each trial in each experimental run. The trailer maker duration was randomized to avoid the detrimental effects of constant overall stimulus duration.10,19,20 The rise time of the leading marker and the fall time of the trailer maker were ramped with 10 msec. However, the offset of the leading marker and the onset of the trailer marker were one msec. These one msec transients ensured similar gating properties in both the standard and test intervals.9,14 These transients are illustrated in Figure 3.
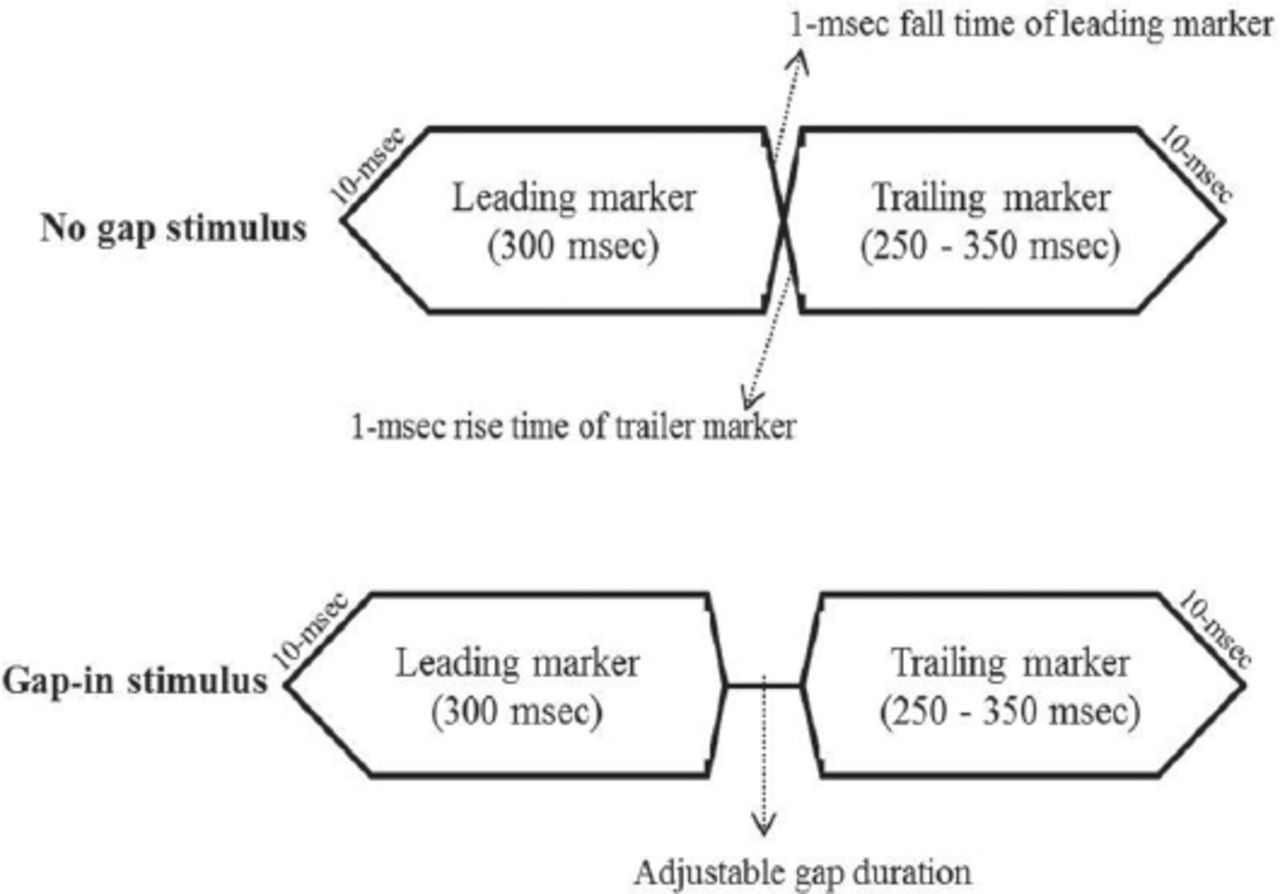
Schematic representation of the transient durations in the no-gap and gap-in stimulus conditions.
Each participants seated in the subject room of the audiometric booth facing a laptop monitor and provided them with TDH-50P Supra-aural headphones with a mod 51 ear cushion that were connected to a GSI-61™ 2 channel clinical audiometer. Before beginning the experiment, all the participants were provided with detailed instructions along with a visual depiction of the screen shots of the experiment. The listeners were asked to select one sound that had a longer silence in it from the 2 sounds heard one after the other. A corresponding block was highlighted on the screen with each sound presentation. A wireless keyboard was connected to the laptop and handed to the participant to select the desired interval by pressing a numerical key (1 or 2) after listening to both the standard and adjustable stimuli. Visual feedback on the correctness of their selection was displayed after each desired selection for each trial. A trail test condition was used involving 15 trials to check all the participants’ understanding of the instructions and their familiarization with the task.
Throughout the experimental procedures, an inter-stimulus interval of 500 msec14,21 and a minimum 1000 msec interval were used after each subject response before presenting the next set of stimuli. We randomly assigned the stimulus conditions, and adoptively changed the imposed gap duration of the adjustable stimulus, based on the participants’ response. If the stimulus condition was BBN, the gap for the adjustable stimulus started at 15-msec, and if the stimulus condition was NBN WC or NBN AC, the gap duration for the adjustable stimulus started at 50-msec. The classic Levitt’s adaptive 2-down 1-up procedure was utilized using a 2 interval alternative force choice method to target the 70.7% correct gap detection threshold.22 To ensure fine measurements for the first 5 reversals of each experimental run or trial, the step size was 1.2 factors, and for the next 6 reversals, the step size was 1.05 factors.
An average of the last 4 reversals out of 11 reversals were used to compute the GDTs so to reduce the variation in the considered GDT.14 We computed an individual standard deviation for each experimental run from the last 4 reversal points to determine whether the GDT measure with that condition needed to be repeated (when the SD was greater than 5 msec). Each participant’s response for all stimuli trials were saved, along with the mean and standard deviation values in a text file, which was saved on the hard drive of the computer for further analysis. The computed GDT for each task was the duration apart from the transients present in the standard stimulus. The Statistical Package for Social Sciences for Windows (Version 24.0, IBM Corp, Armonk, NY, USA) was used to analyze the data. A One-way repeated measure of Analysis of Variance (ANOVA), paired-samples t-test, and Pearson’s correlation coefficient were performed.
Results
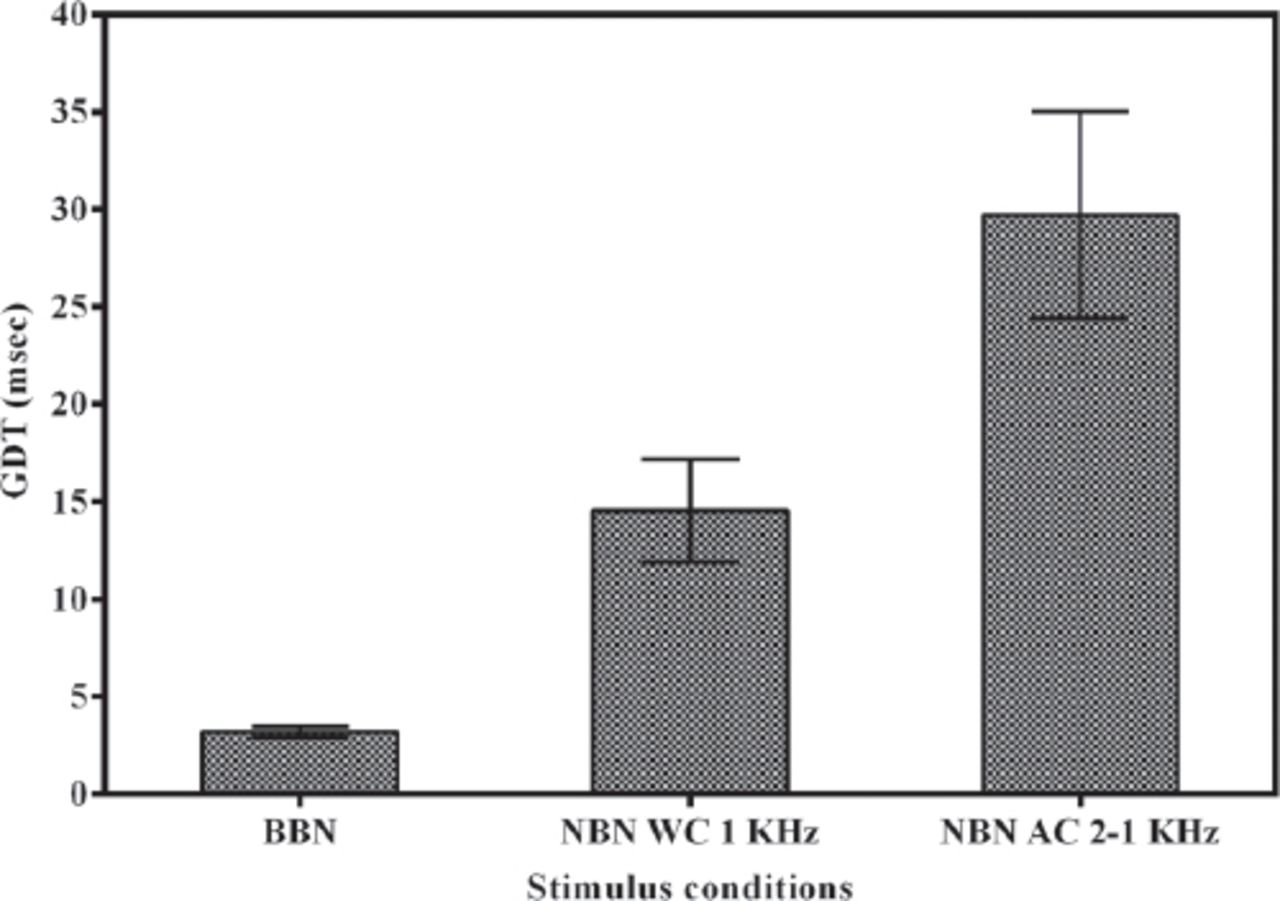
The computed GDT data from the last 4 reversals of each participant’s responses under each stimulus condition across all subjects were averaged. The mean and SDs of the GDT for the BBN, NBN WC, and NBN AC conditions are provided in Figure 4 and Table 1.

Average gap detection thresholds (GDTs) along with standard errors (in msec) across stimuli conditions. Note: AC Stimulus condition is depicted as narrowband noise (NBN), leading marker frequency–trailing marker frequency in KHz.
Average gap detection thresholds in different stimulus conditions and corresponding standard deviations measured across subjects.
Furthermore, individual GDTs for each participant in each condition are shown in Table 2. Mauchly’s test indicated that the assumption of sphericity had been violated for the main effects of stimulus condition on GDTs -χ2(2)=14.918, p<0.001. As a result, degrees of freedom were corrected using Greenhouse-Geisser estimates of sphericity (0.69) for the main effect. A one-way repeated measure of ANOVA indicated that the GDTs obtained differed significantly across the stimulus conditions (F [1.38, 35.88]=70.191, p<.0001, eta2=0.73). The Pairwise comparisons (t tests) that was conducted, revealed significant differences among the GDTs obtained in different conditions. The analysis showed that the GDTs obtained with the NBN AC condition was significantly higher than those GDTs obtained with the NBN WC condition (t[26] = - 6.012, p<0.0001]) and also higher than the GDTs obtained with the BBN condition (t[26] = - 9.973, p<0.0001]). Further, the analysis also showed that the GDTs obtained with the NBN WC condition was significantly higher than the GDTs obtained with the BBN condition (t[26]= -8.73, p<0.0001]). Moreover, the Pearson correlation among the GDTs of the 3 stimulus conditions did not show any significant positive correlations among any pairs.
Individual gap detection thresholds (in msec) for the BBN, NBN WC and NBN AC stimulus conditions.
Discussion
The aim of the study was to explore the clinical utility of the Windows-based psychoacoustic experimental software Psycon (Version 2.18) and to estimate GDTs and to provide normative values for young listeners in the BBN, NBN WC, and NBN AC conditions. The overall results obtained with the above detailed parameters were consistent with those of previous study that used a similar methodology.7-9,11,14,21,23-25
In the study, the temporal acuity abilities measured with GDT using BBN revealed an average of 3.19 msec silence detected by the young listeners. Similar findings obtained with ATTR have been reported by Lister et al10 for 30 adult listeners with normal hearing. They also reported an average GDT of 3.2 msec (SD: 1.9 msec) with BBN. In addition, our findings were consistent with Hoover et al7 who found an average of 4.53 msec of silence obtained using the GIN test with 19 young normal hearing adults. In line with these findings, using the GIN test, Shinn et al26 have reported an average temporal gap of 4.87 msec (SD=1.25 msec) and 5 msec (SD=1.16 msec) for right and left ears, respectively for 22 normal hearing listeners aged between 12 to 18 years. Similarly, using the GIN test, Samelli and Schochat27 have reported an average of 4.19 msec temporal gap for BBN. Overall, our findings on GDTs show that Psycon (Version 2.18), along with appropriate AUX codes, could reliably provide accurate GDTs using BBN.
In contrast to the above findings based on the BBN stimulus, the average GDT using the NBN WC stimulus with a marker frequency of 1.0 KHz revealed that the studied listeners detected an average silence of 14.53 msec. These findings were consistent with the outcome of Florentine’s et al12 study. The midpoint of the psychometric function curve of 1.0 KHz was 12.7 msec (SD: 1.28 msec). Similarly, Formby et al28 have found an average GDT of 15.65 msec for the leading 0.9 KHz (bandwidth: 190 Hz) marker and trailer marker of 0.99 KHz (bandwidth: 100 Hz), with a varying leading marker duration of 50-90 msec and a trailer marker duration of 100-140 msec. However, in the present study, the results (average GDT of 14.53 msec) obtained with the NBN WC stimulus were comparatively higher than the average 8.43 msec reported by Phillips and Smith29 and the average 6.7 msec reported by Elangovan and Stuart30 for similar NBN makers of 1.0 KHz. Also, the mean GDT (14.53 msec) from the present study is higher than the mean GDT of 3.2 msec with different markers centered at 2 KHz in Lister et al.10 These differences among studies could be due to the bandwidth of the signal considered, and the slope of the digital filters used for designing the stimulus. Furthermore, these differences also could be due to the procedure differences involved in the experiments.
In this study, the temporal resolution abilities assessed with respect to the AC paradigm revealed that an average of 29.71 msec (sd: 13.8 msec) silence duration was detected by the listeners. These findings were comparative with previous studies that involved similar marker frequencies of 2.0 KHz as leading marker and 1.0 KHz as trailer marker.14,21,23 For example, Lister et al21 have reported GDTs of 27 msec in an anechoic listening environment and reported GDTs of 29.9 msec in a reverberant listening environment. However, the obtained GDTs for the AC condition were lower than other investigations. For example, the obtained mean for GDTs was lower than the mean GDTs found by Hess et al,11 which was 35.71 msec at 50 dB sensation level, and by Lister et al,10 which was 42.6 msec obtained for dissimilar markers centered at 2 KHz before the gap and one KHz (both of these studies used the ATTR instrument). Moreover, such variations between our findings and other study findings may be due to instrumentation and procedure differences.
In addition, the finding from the study of no correlation among the 3 conditions suggests that a separate auditory process may be involved WC and AC gap processing. The study of Phillips and Smith29 measured temporal gap processing in 95 normal hearing adults. They obtained gap detection thresholds for 2 NBN WC conditions with markers centered at 1.0 KHz and 4.0 KHz, and for one NBN AC condition with markers centered at 4.0 KHz and 1.0 KHz. They reported evidence for a weaker correlation between the WC and AC conditions compared to a higher correlation between the 2 WC conditions, which suggests a separate process is involved in the identification of the gaps in WC and AC.29 According to Phillips and Smith,29,31 the temporal processing of WC gap detection task of same marker frequencies (spectrally overlapping) involves an activation of the same neuron regions in the peripheral auditory system. The silent gap is identified due to the detection of a lack of neural activity (a discontinuity detection process). In contrast, the temporal processing of the AC gap detection task of dissimilar makers (spectrally non-overlapping) involves an activation of different neuron regions in the peripheral auditory system. The silent gap is identified due to the monitoring of the time between the offset of the leading marker and the onset of the trailing marker (a relative timing process). The complexity of the relative timing process due to frequency disparity induces more time to identify the temporal gap, and hence larger GDTs. Thus, the SD obtained by the present study also supports the complexity effects of AC gap processing in which higher variations exist in AC temporal acuity compared to WC among normal hearing listeners, which is consistent with the previous studies.14,21,23
The overall findings of the study indicate that temporal resolution abilities using gap detection could be reliably and easily assessed using computer applications with appropriate stimulus and experimental parameters. However, the findings from the study were limited to 1 KHz for WC and 2-1 KHz AC gap investigations. Further, the variability in the GDTs of the WC and AC conditions across studies suggest a need exists for more studies on standardized procedures to obtain normative data on GDTs, and also to create clinically reliable tools to assess the temporal resolution of speech and to diagnose CAPD.
Acknowledgment
The authors appreciate the support from the Research Center, College of Applied Medical Sciences and the Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Aarabia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 30, 2018.
- Accepted December 5, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.