


Abstract
Objectives: To figure out the burden of chronic non-communicable diseases in Iraq on the health system through measuring the incidence and trend of these diseases.
Methods: This descriptive study that was conducted between January 2016 and 2017, involved treatment data of chronic non-communicable diseases (hypertension, diabetes mellitus, ischemic heart disease, stroke, asthma and epilepsy). The data was collected from the registry of the Department of Health and Vital Statistics in the Ministry of Health, Babylon, Iraq, between 2000 and 2016.
Results: The prevalence of diabetes mellitus had significantly increased from 19.58/1000 in the year 2000 to 42.27 in 2015 (p=0.0002). The prevalence of hypertension also increased from 31.33 to 45.82 (p=0.003) in the same period. The prevalence of cerebrovascular accidents showed a significant increase especially after 2008 (p=0.007), while ischemic heart diseases increased from 6.3/1000 in the year 2000 to 8.2/1000 in 2014 with no significant change.
Conclusion: Non-communicable diseases in Iraq continue to show as a new developing burden after the 2003 war. Hypertension and diabetes mellitus demonstrate rapidly rising trends which may, in turn, enhance the occurrence of ischemic heart diseases and cerebrovascular accidents.
Epidemiological transition in industrialized countries started around 1900, with increase of the chronic and degenerative diseases that peaked around 1950 accompanied by marked fall in infectious diseases mortality and morbidity.1 This was not shared equally by all nations of the globe; in the developing countries, the prevalence of old, emerging and re-emerging communicable diseases have been constant or increasingly occurring.2 The burden of non-communicable diseases defines the national health challenges that constrain the economic and social progress all over the world.3 This group of diseases causes 40 million deaths annually, approximately one third of these are premature deaths mostly in the low and middle income countries (80%), furthermore these diseases have a ingrained effect on disability trends, in which they are estimated to be responsible for approximately two third of years lived with disability in those countries.4-6 The burden categorization of a disease can range from the incidence and prevalence to its effect on the longevity, morbidity, state of health, quality of life and the monetary aspects that include direct and indirect loss arising from premature death, disability or injury due to the disease or its complications.7
Since 2010, the Eastern Mediterranean region (EMR) entered in a whirl of unrest.8 War and other armed conflicts usually result in severe morbidity and mortality. Many social and health problems occurred during and following the conflicts manifested by destruction of the health system infrastructures, lack of food and safe water, poor sanitation, lack of medical care and health services.9 The global burden of disease (GBD) 2015 study showed that the leading cause of death in the EMR last years was ischemic heart diseases with a rate of 90.3/100000, which rose by 17.2% since 1990, while high blood pressure increased by 83.3% since 1990.4 The first gulf war in 1991 caused vast destruction to the Iraqi major infrastructures essential for healthy life.10 The economic sanction came to aggravate the condition of deterioration with health care budget almost cut by 90%.11 Approximately 12% of the hospitals were damaged during the United States of America (US) invasion or thereafter.12 Understaffed and weakly resourced hospitals have struggled to overcome the raised load of sick and injured attendants and to provide them with the required essential care.13
Rationale of the study
The duple burden of diseases (old and new) makes it difficult for policy makers to address the variable population health needs. The current study was a trial to portray the trend of chronic non-communicable diseases in the form of incidence and prevalence, in order to assess the burden of these disease over around a decade and a half to highlight the problems that are facing our health system.
Methods
This descriptive study that was conducted during the period between January 2016 and 2017, involved treatment and processing of data related to chronic non-communicable diseases.
The data encompass the most prevalent chronic health problems including hypertension, diabetes mellitus, ischemic heart disease, stroke, asthma and epilepsy. Data was collected from the registry of the specialized Department of Health and Vital Statistics in the Ministry of Health, and supported by data from the Division of Non-Communicable Diseases Control and Prevention Center and some survey data. Data was formed from hospital discharge registries and outpatient visits to the hospitals and primary health care centers. All registries of non-communicable diseases during the period from 2000-2016 were included; however, incomplete registries were excluded to enhance accuracy.
The total sample was 40,927,512, of which, 12,025,843 were diabetes mellitus, 14,516,532 hypertension, 2,823,290 ischemic heart diseases, 570,021 cerebrovascular accident, 10,107,239 were asthma and 884,587 were cases of epilepsy.
Data was gathered on monthly basis, triple checked and confirmed by data from other official sources to fill the gaps caused by missing data and to increase reliability.
To measure the rate of occurrence; the total population for each governorate, and for Iraq, was obtained from the central statistical organization to be used as denominators; these rates were then plotted against time to define the trend.
In respect with age, data was categorized into: under 15 years, 15-45 years, and more than 45 years in accordance with the original categorization of noncommunicable diseases (NCD) center of the Ministry of Health. The number of cases of the 3 age groups also plotted against time to get the trend of each disease by age and to detect changes in age of predilection.
Ethical approvals were granted by the Ethical Committee in the College of Medicine, Mustansiriyah University and the Iraqi Ministry of Health in Iraq. As this is a surveillance study that deals only with numbers, and with no intervention, so indication according to the principles of Helsinki Declaration was not applicable.
The Statistical Package for Social Sciences (SPSS) Version 23 (IBM Corp., Armonk, NY, USA) was used to estimate the rates. Linear regression was calculated to estimate the trends of the disease. The outcome depended on the picture of the slop whether going downward, upward, flat, or unpredictable, to assess the trend. A p=0.05 was considered significant.
The percentage change was calculated for the whole and mid time periods as a measure of difference in the trend for each disease, using the following formula:
Where as: PC stands for percent change, R2 stands for new rate, and R1 for old rate.
Results
Diabetes mellitus
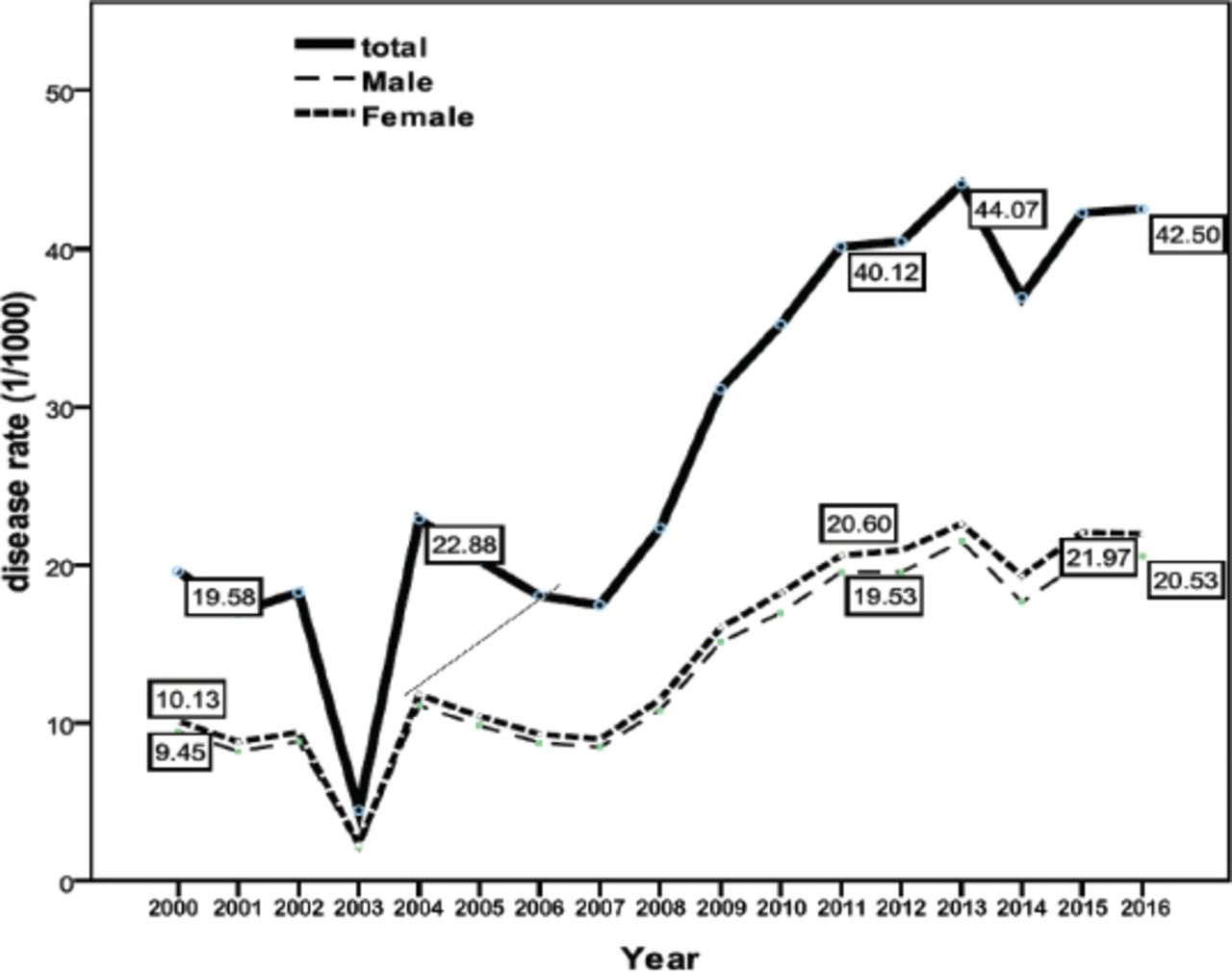
The prevalence of diabetes mellitus had significantly raised from 19.58/1000 in the year 2000 to 42.27/1000 in 2016 with a percent change of 38.25 (p=0.0002). Males and females were affected almost equally. The majority of cases aged more than 45 years are shown in Figure 1, never the less, there was a small proportion (5%) aged less than 15 years.
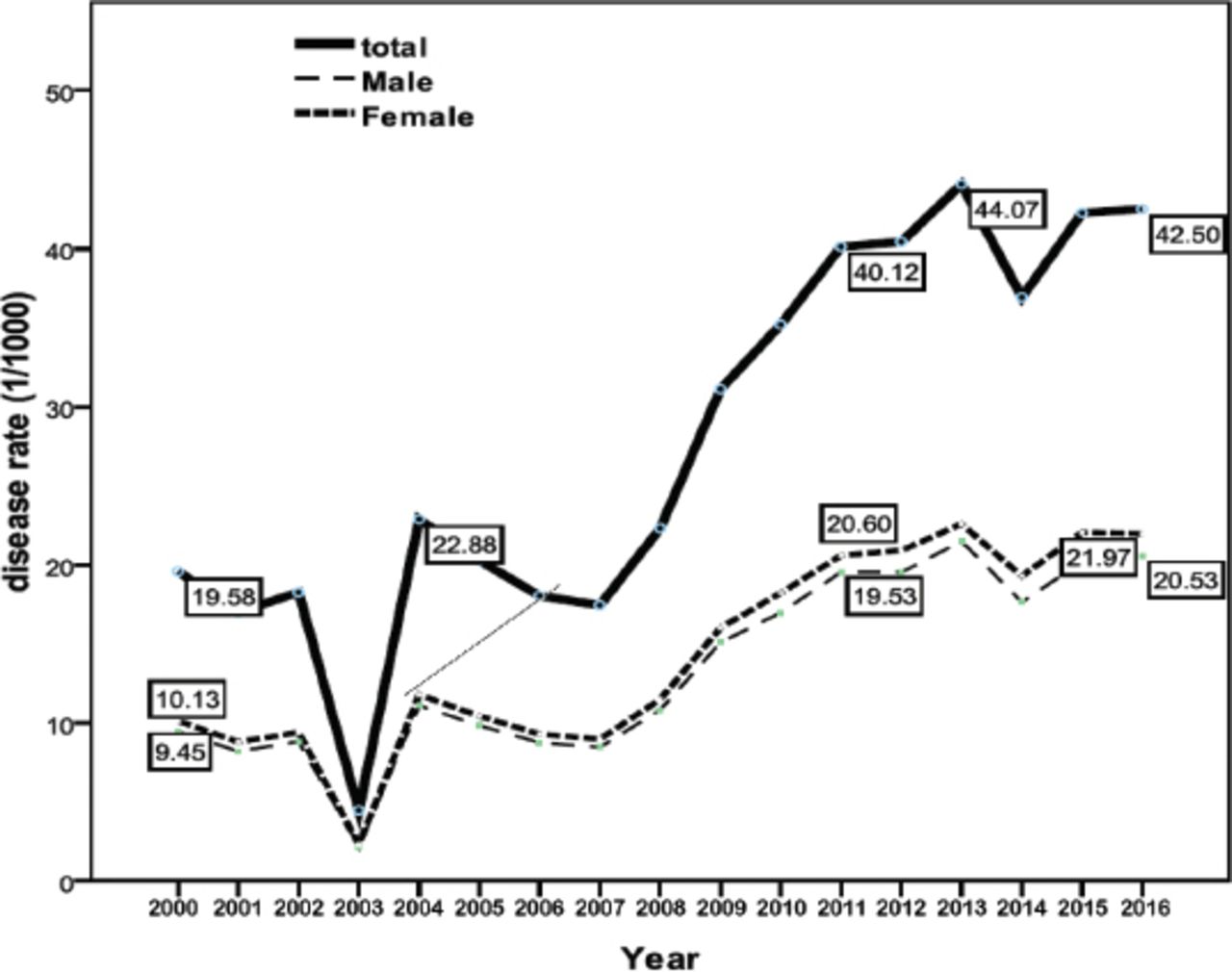
Trend of diabetes mellitus distributed by gender (2000-2016), p=0.0002.
Hypertension
The prevalence of hypertension in Iraq showed a significant change during the last 17 years from 31.33/1000 in the year 2000 to 45.82/1000 in 2015 (p=0.003), mostly among adults more than 45 years (Figure 2). Both genders were almost equally affected.
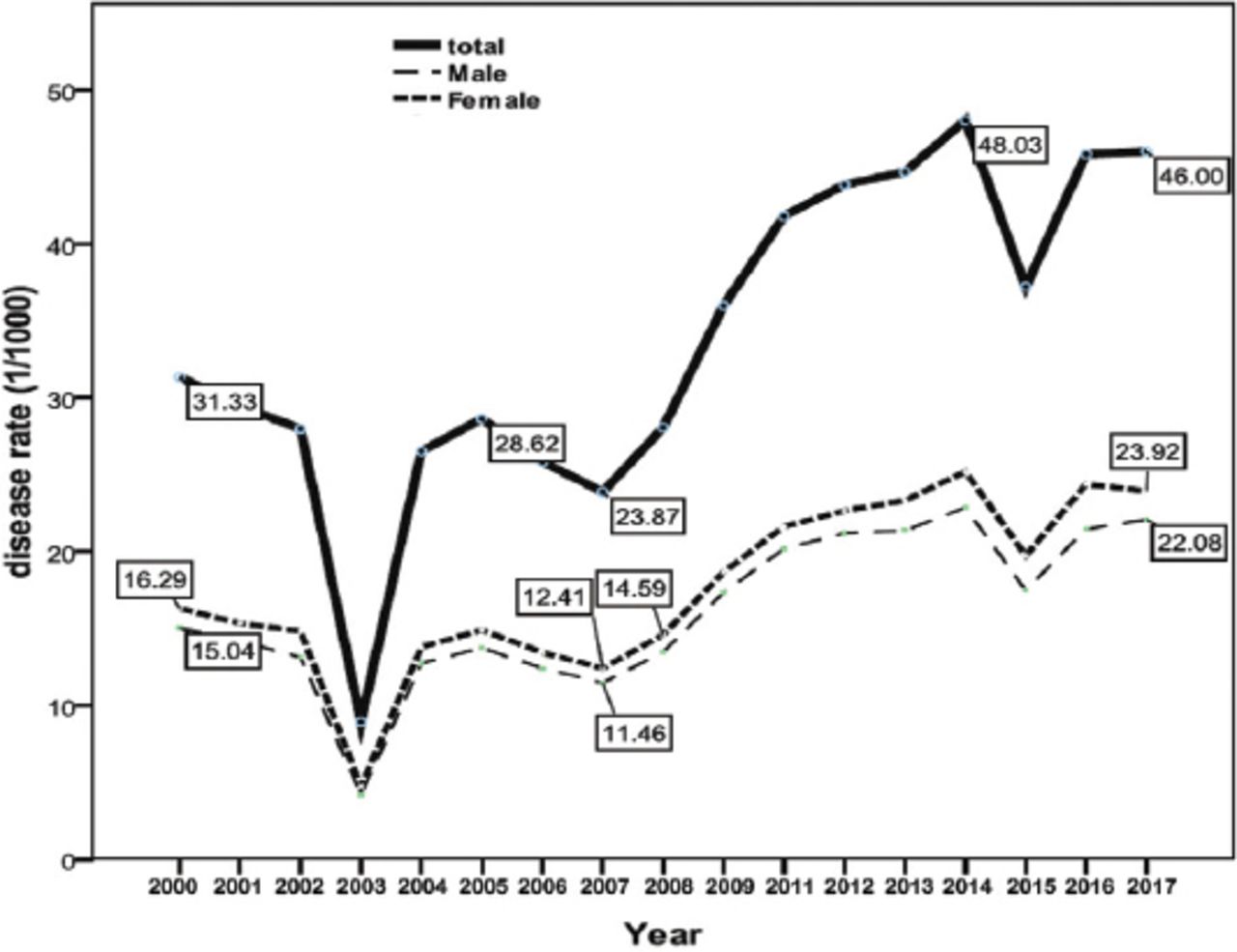
Trend of hypertension distributed by gender (2000-2016), p=0.003.
Ischemic heart disease
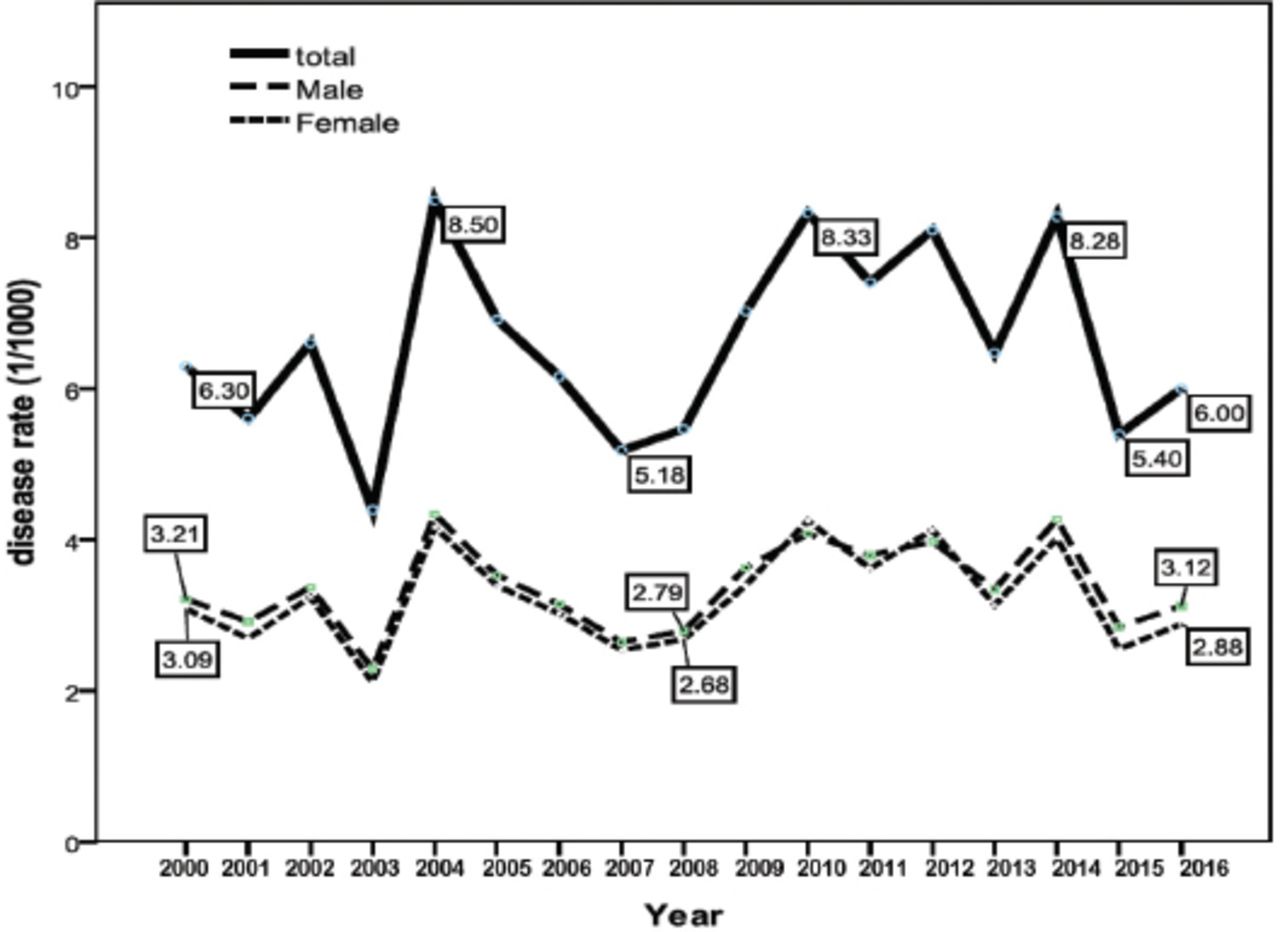
The trend of ischemic heart diseases increased from 6.3/1000 in the year 2000 to 8.2/1000 in 2014; however, this increase in the trend could not reach a significant level. Both genders were affected almost equally and mostly after the age of 45 years (Figure 3).

Ischemic heart diseases by gender (2000-2016), p=0.814.
Cerebrovascular accidents
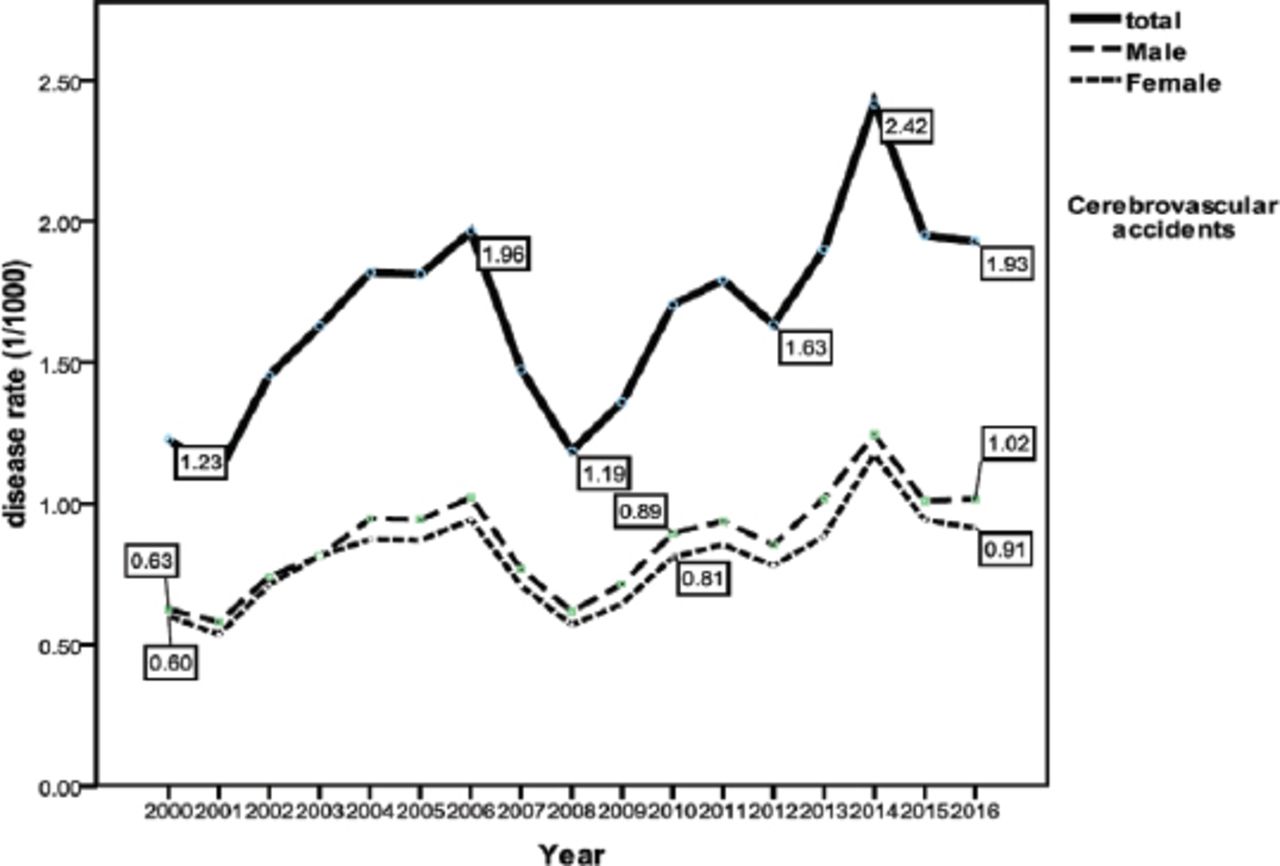
The prevalence of cerebrovascular accidents (CVA) in Iraq showed a significant increase especially after 2008 with a percent change of 56.91 (p=0.007). Both genders were similarly affected, mostly above the age of 45 years (Figure 4).

Cerebro-vascular accidents by gender (2000-2016), p=0.007.
Asthma
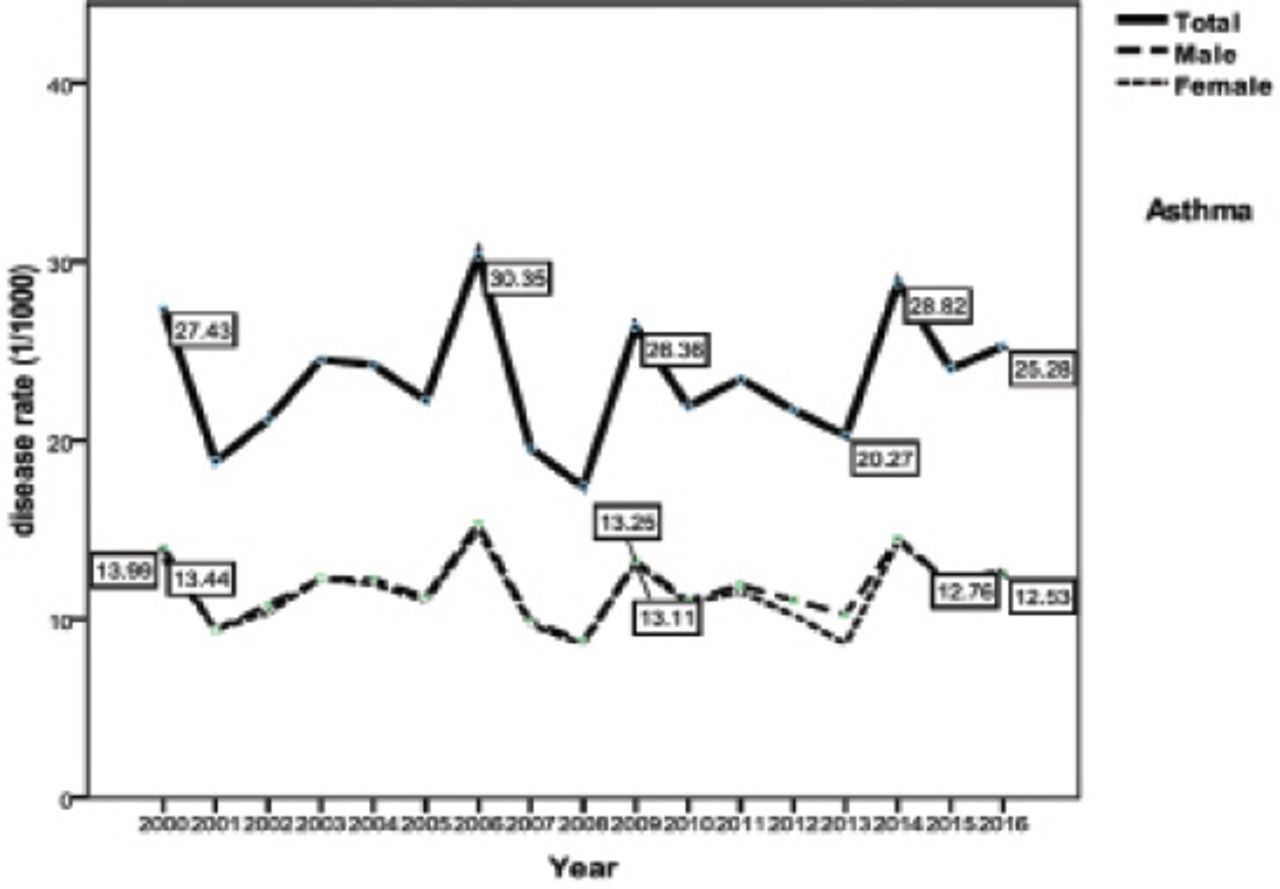
The occurrence of asthma showed no significant changes in its trend (Figure 5). Both genders were almost equally affected, more than 40% of the cases aged less than 15 years, and 40% aged 45 years or more.

Trend of asthma by gender (2000-2016), p=0.285.
Epilepsy
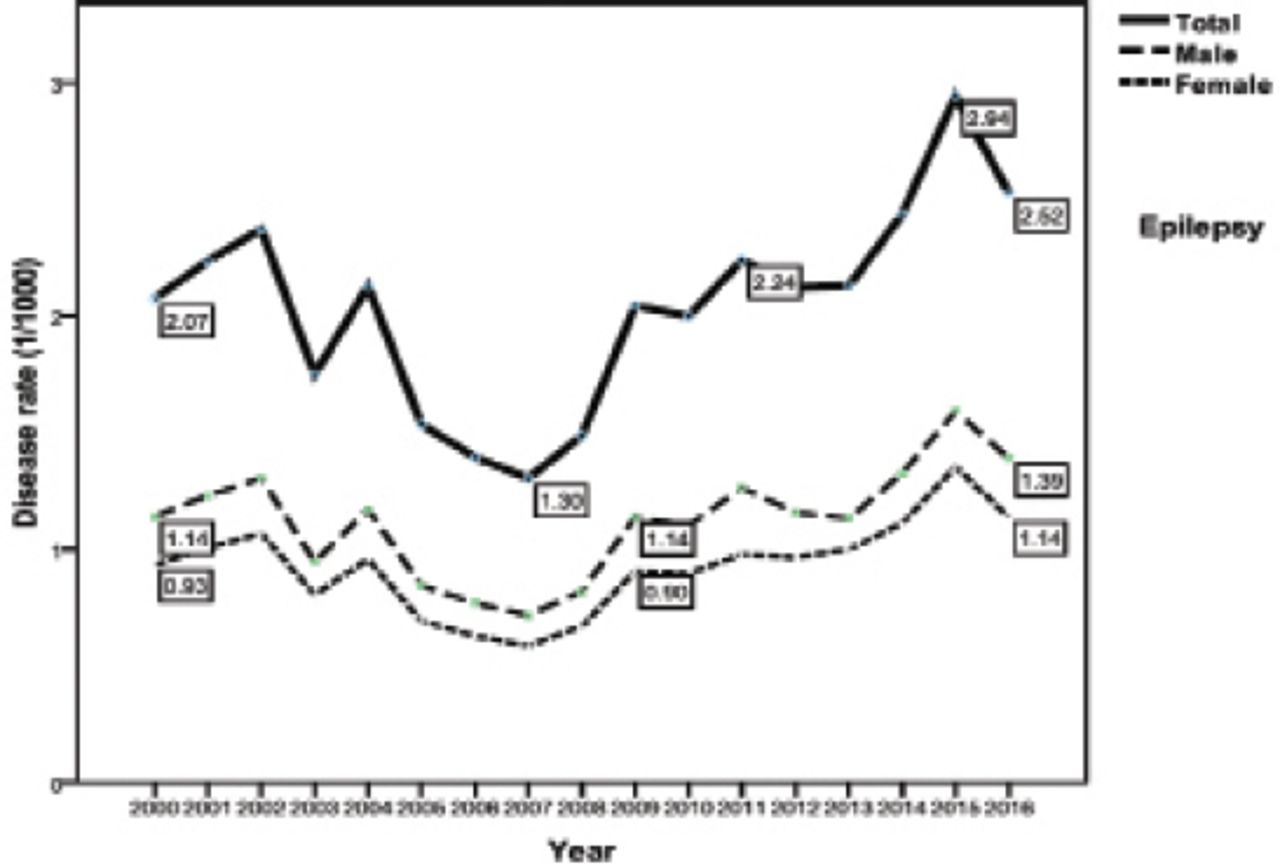
The trend of epilepsy had a step rise in its occurrence as shown in Figure 6. It had been raised since 2008, affected both genders with a similar rate, the number of cases was more in the age group more than 45 years.

Trend of epilepsy by gender (2000-2016), p=0.09.
Table 1 shows the percent change in incidence rate of chronic non-communicable diseases for the period 2000-2016.
Percent change in prevalence rate (1/1000) of studied non communicable diseases (2000-2016).
Discussion
Non-communicable diseases are responsible for 2 of every 3 years lived with disability.14 The burden of chronic non-communicable diseases is immense as it forms 75% of the global mortality15 and 75% of the global GDP (approximately 63 trillion US dollars), or per capita cost of approximately 139 US dollars.16 As the portrayed trend in the current study represents the rate of patients attending the health facilities rather than the real prevalence, so this may only reflect the utilization of such services giving an obvious unavoidable underestimation.
Our findings revealed that diabetes mellitus increased significantly from 19.5/1000 in the year 2000 up to 42.1/1000 in 2015 with a percent change of 115%. World Health Organization (WHO) reported a collateral raised age standardized prevalence rate of diabetes among Iraqi populations from 12.5-17.5% during 2000-2014.17 This trend goes with what is happening in the regional countries such as Kingdom of Saudi Arabia, Lebanon and Iran and the whole world.18-21 The number of diabetic almost quadrupled since the year 1980, it is estimated that the number in 2015 reached 422 million 22 with a prevalence rate of 8.8% or one of every 11 persons.23 This ascending prevalence is more in the middle and low income countries and mirrors the high prevalence of overweight and obesity and the widespread lack of physical activity.24 Diabetes is the 6th leading cause of disability and the third global risk factor following hypertension and smoking.25 The burden of diabetes comes from its expenditure that accounts 12% of the total health expenditure reaching 673 billion US dollars according to the International Diabetes Federation (IDF) estimation. A study in Singapore estimated the total financial burden from type 2 diabetes at approximately 5000 US dollars per patient.26 This is superadded by the wide range of serious complications such as ischemic heart disease, nephropathy, retinopathy and amputations that disturb the patients’ life.27 Diabetes is a leading cause of death, where in 2012 it caused the death of 1.5 million people directly and 2.2 million through an increased risk of cardiovascular and other diseases. Forty three percent of these deaths occur at the productive age before 70 years and is higher in middle and low income countries. The estimated prevalence of diabetes/hyperglycemia in Iraq according to WHO country profile is 13.2%, and three fourth of them are on Insulin.17,21 Hypertension also showed a progressively raising rate from 31.33/1000 in 2000 to 45.8/1000 in 2015 with a drop in 2003 that was associated with the USA invasion of Iraq and the disrupted health surveillance system at that year. According to STEPwise approach to Surveillance (STEPS) surveys; the prevalence of hypertension declined from 40.4% in 2006 to 35.5% in 2015.28 Turkey reported a stable rate within 30% in the period 2003-2012, Iran showed a mild rise between 2007-2011.29,30 Hypertension is thought to be responsible for more than half of the death cases caused by strokes or ischemic heart diseases.31 From financial point of view the presence of hypertension was estimated to double the health expenditure of an individual, which is further redoubled by co-presence of diabetes.32 The prevalence of hypertension in the Eastern Mediterranean region is near the highest (41%) with high income countries have lower prevalence of hypertension (35%) than the low and middle income ones (40%).33 According to STEP survey (2015), the prevalence of hypertension was 35.6%, being higher among men with a very low control rate (7.9%). Hypertension formed approximately 19% of the total disability-adjusted life year (DALY) loss in 2015. It also accounts for 9.4 million deaths worldwide annually, and responsible for at least 45% of deaths due to heart diseases and 51% of those due to stroke.34 Ischemic heart disease showed a fluctuant trend ranging between 4.5 and 8.5/1000. It witnessed a decrease in its rate in 2015-2016 down to 4.01/1000. Ischemic heart diseases are the main cause of death worldwide and account for 16% of all death causes in the region.4
Globally; there were approximately 17.7 million deaths from cardiovascular diseases in 2015 representing nearly 30% of the global total deaths, 7.4 million caused by ischemic heart diseases and 6.7 million were due to stroke.35 Both occupied the first 2 causes of premature deaths and high years of life lost (YLLs) globally.4 This picture differs among different world regions where the last 25 years witnessed a decrease in cardiovascular deaths (mainly coronary diseases) by more than 50% in high income countries while low and middle income countries showed a flat or even increasing trend.36 Even within the developed societies, the lower socioeconomic groups have higher incidence and mortality of cardiovascular diseases due to poorer risk factor profile.37 In Iraq, ischemic heart diseases occupied the second cause of premature deaths after war and violent deaths with stroke been the fourth of the main 10.4 In the current study, an interesting finding was that although diabetes mellitus showed a significantly increased trend, yet, the prevalence of ischemic heart diseases has not been increased in the same rate, this could be explained by that this spike in the trend of diabetes mellitus in Iraq is recent and so, its effect (as a risk factor) on ischemic heart diseases did not get enough time to appear, probably, the coming years may make this effect more clear. Cerebrovascular accidents almost doubled between 2000-2013 from 1.23-2.42/100000. The most prominent burden of stroke is its high case fatality rate which is approximately 12.7% globally, while in Iraq; a hospital based study estimated it to be 22.7%.38 Stroke is the third main cause of mortality in Iraq and accounts for 9.3% of all deaths, survivors often get an associated long term disability.39
Asthma remained within the same range of 20-30/1000. The National estimation of the prevalence of asthma in Iraq by Iraq Family Health Survey (IFHS) in 2006 provided a rate of 8.3 per 1000 which is comparable to the rates in the neighboring countries such as Iran, while in 2015 it jumped to 22 per 1000 (2.2%).40,41,28 The prevalence of asthma was more in young people, probably due to the registration method as many of the cases of asthma in adults are included within the category of chronic obstructive lung diseases.
Asthma is one of the major non-communicable diseases affects approximately 240 million people in 2016 worldwide, mostly children.42 It affects all countries regardless the level of development but mortality been higher in low and middle income countries reaching approximately 80% of all Asthma related deaths.43
The trend of epilepsy had a mild rise with a percent change of 21%. STEPwise approach to Surveillance Survey 2015 reported a prevalence rate of epilepsy of 0.4% which was much lower than that of Egypt (5.1/1000) and Kingdom of Saudi Arabia (6.5%).44
Limitations of the study
There is an underestimation for most of the rates of the studied diseases as data was collected from the registries of hospitals and primary health care centers and not population based. Many of our patients prefer to attend the private clinics for a better care, those patients are not registered in the statistics of the Ministry of Health as the private sector is not included in the surveillance system.
In conclusion, it can be interpreted from this study that non-communicable diseases in Iraq continue to show as a new developing burden with a raised trend for all. Hypertension and diabetes mellitus demonstrated rapidly rising trends which may, in turn, enhance the occurrence of ischemic heart diseases and CVA.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 18, 2018.
- Accepted December 5, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.