


Abstract
Objectives: To investigate the potency and speed of action of 2% lidocaine and 3% prilocaine for upper teeth extractions.
Methods: This prospective clinical study was conducted from November 2016 to May 2017. Ninety-six patients, aged between 16 to 70 years old were recruited in this study. Two regimens were randomly administered over one visit. Patients, treatment group I, received 2% lidocaine with 1:00.000 adrenaline. Patients treatment group II received prilocaine 3% and felypressin 0.03 I.U. per ml. The efficacy of pulp anesthesia was determined by electronic pulp testing. At any point of trial (10 minutes), the anesthetized tooth becomes unresponsive for maximal pulp stimulation (64 reading), the extraction was carried out.
Results: There were no significant differences in the mean onset time of pulpal anesthesia and extraction between the prilocaine and lidocaine buccal infiltration groups (p=0.28). However, clinically, the patients in prilocaine group recorded faster onset time of anesthesia and teeth extraction than those in lidocaine group.
Conclusion: Prilocaine has a better clinical performance in terms of providing rapid dental anesthesia and earlier teeth extraction than lidocaine but the differences were not significant. Prilocaine with felypressin could be a good choice for patients who have contraindication to the use of lidocaine with adrenaline.
There are continuous efforts in the field of dental local anesthetic research for finding the optimal local anesthetic which can be used safely for normal and medically compromised patients.1-4 Lidocaine and prilocaine are amide local anesthetic agents but prilocaine is less toxic and vasodilator than lidocaine.5 So, prilocaine can be a good choice for patients for whom vasoconstrictor is contraindicated.6 Adding a vasoconstrictor agent to the local anesthetic solution prolongs the length of action and increase the depth of anesthesia.7 However, in high risk such as unstable angina, uncontrolled severe hypertension, uncontrolled congestive heart failure and uncontrolled hyperthyroidism, patient adrenaline may cause acute hypertensive crisis, angina, arrhythmia or myocardial infraction.6-8 Effects of adrenaline are exaggerated in medically compromised patients even with small dosages.6 Felypressin is a non-catecholamine vasoconstrictor and chemically is related to vasopressin, the posterior pituitary hormone.1,5 Felypressin constricts venous outflow.7 So, it is less vaso-constrictive than adrenaline. Felypressin added to prilocaine in a concentration of 0.03 IU/ml. In light of these facts, prilocaine with felypressin could be of value to be used in medically compromised patients because it has less vasodilation, toxicity and fewer hemodynamic effects than lidocaine with adrenaline.5-8
The aim of this study was to compare the effectiveness of 2% lidocaine with epinephrine (1:100,000) and 3% prilocaine with felypressin (0.03 I.U. per ml) and the possibility of using them in the oral surgery of medically compromised patients.
Methods
This randomized, clinical study was conducted according to the principles of Helsinki Declaration from November 2016 to May 2017 in the Oral and Maxillofacial Department, Taibah Dental College, Saudi Arabia after obtaining the approval from Taibah Dental School Research Ethics Committee.
Recruitment of patients for this study took place in the Oral Surgery Department, Taibah University College of Dentistry, Saudi Arabia. Ninety-six patients were included in this study who were scheduled for extraction ≤2 simple teeth under local anesthesia, healthy or with mild systemic diseases (class I or II according to American Society of Anesthesiology) and capable to understand and cooperate with the requirements of the protocol. However, patients with allergy to local anesthetic agents, need multiple teeth, or surgical extraction were excluded.
Randomized process began before starting the study, researcher printed a certain number of slips of paper with 3% prilocaine or 2% lidocaine regimen and asked the department’s secretary to mix them up and placed them in a sequential number of opaque envelops. Once the patient was allocated to the study, a numbered envelope was attached to the patient’s dental hospital treatment record. On dental chair, the patient was asked to sign the consent form after opening the envelop by a dental assistant who was completely independent of the whole process. If the patient was in lidocaine or prilocaine regimen, buccal infiltration injection was administrated by inserting a short needle at the depth of the sulcus and advanced 4-7mm in order to deposit the anesthetic solution (1.4ml lidocaine 2% with epinephrine 1:100,000 or prilocaine 3% felypressin [0.03 I.U. per ml]) around the apex of extracted tooth. The remaining 0.4ml of the anesthetic cartilage was given in the palatal side of the extracted tooth 5mm far from gingival margin. A dental surgeon was not associated with the study.
The efficacy of pulp anesthesia was determined objectively by electronic pulp testing. This will be performed with an Analytic Technology Pulp Tester (Analytic Technology Redmond, Washington, USA). Testing performed at a rate of 2 minutes. In order to validate the pulp tester readings, a control unanesthetized tooth on the contra-lateral side of the upper jaw was also tested at base line and at intervals in the study.
Anesthetic success is defined when 2 or more consecutive episodes of maximal pulp stimulation (64 reading) without sensation are recorded. The efficacy of pulp anesthesia was evaluated for maxillary upper tooth listed for extraction or its adjacent teeth (if intended tooth for extraction was not vital), before injection (baseline) and at intervals of 2 minutes until 10 minutes. At any point of trial (10 minutes), the anesthetized tooth becomes unresponsive for maximal pulp stimulation (64 reading), the extraction was carried out. After 10 minutes of injection of local anesthesia, if the anesthetized tooth was still positively responsive to electrical pulp tester, the second cartridge of LA was administered.
Both patients and the researcher testing anesthetic effectiveness were not aware to which local anesthetic BI. regimen was administered. All injections were given by the same operator. Standard aspirating dental cartridge syringes (ATI, A. Titan Instruments, Inc., Orchard Park, New York, USA) fitted with 27-gauge, 21mm short needles (C-K Ject [27 gauge] 0.4 mm × 21 mm, Korea) were used for buccal and palatal infiltrations.
Statistical analysis
Sample size calculation was made for this study based on a study by Mittal et al.9 A sample size of 90 would have 90% power to detect a difference in success rate of 21% in a continuous outcome measure assuming a significance level of 5% and a correlation of 0.5 between responses from the same subject. A total of 96 patients were recruited in this study. Data were entered and analyzed using the Statistical Package for Social Sciences Version 20 (SPSS, Inc., Chicago, IL, USA). These statistical tests were descriptive analysis, cross tabs analysis and independent sample t-test.
Results
Ninety-six adult patients were recruited. Four patients were excluded due to faint following local anesthetic injection (2 patients from lidocaine regimen and 2 from prilocaine regimen) and were excluded consequently according to study protocol and official clearances. The final sample size included 92 patients aged between 16 to 70 years old (36+12.50).
Seventy-nine patients in this study secured anesthetic success for upper teeth following pulp testing after lidocaine and prilocaine regimens within 10 minutes and they had successful extraction. However, there were 13 patients with failure dental extraction who did not achieve the anesthetic success within the study duration time (10 minutes) and an additional local anesthetic was administered. There were 5 patients in prilocaine group and 8 patients in lidocaine group. It was considered appropriate to use non-parametric tests to quantify the number of episodes with no responses to maximal pulp stimulation (64 reading), termed anesthetic success. Cross tabs analysis was carried out to obtain the numbers and percentages of patients in both groups. Table 1 summarizes the overall outcome of the anesthetic success for the pulp of upper teeth of the 92 patients who participated in the study. In this table, the anesthetic success represents “no response to maximal electronic pulp stimulation (64 reading)”, and the anesthetic failure represents “positive response to electronic pulp stimulation”.
Number and percentages of anaesthetic successes at time interval for upper teeth pulp anaesthesia following prilocaine and lidocaine buccal infiltration in 90 adult patients.
The range onset of pulpal anesthesia and extraction of upper teeth in this study was from 2 to 14 minutes. Table 2 reveals that the mean onset time of anesthesia and extraction of upper teeth using pulp testing after prilocaine buccal infiltration (prilocaine regimen: 3.91+3.27) was clinically faster than after lidocaine buccal infiltration (lidocaine regimen: 4.70+3.68). The application of t-test revealed that there were no significant differences in the mean onset time of pulpal anesthesia and extraction between the prilocaine and lidocaine buccal infiltration groups (p=0.28, Table 2, Figure 1). It was found that patients in the prilocaine buccal infiltration group recorded faster onset time of action regarding anesthesia and teeth extraction than patients in lidocaine buccal infiltration group but statistically non-significant.
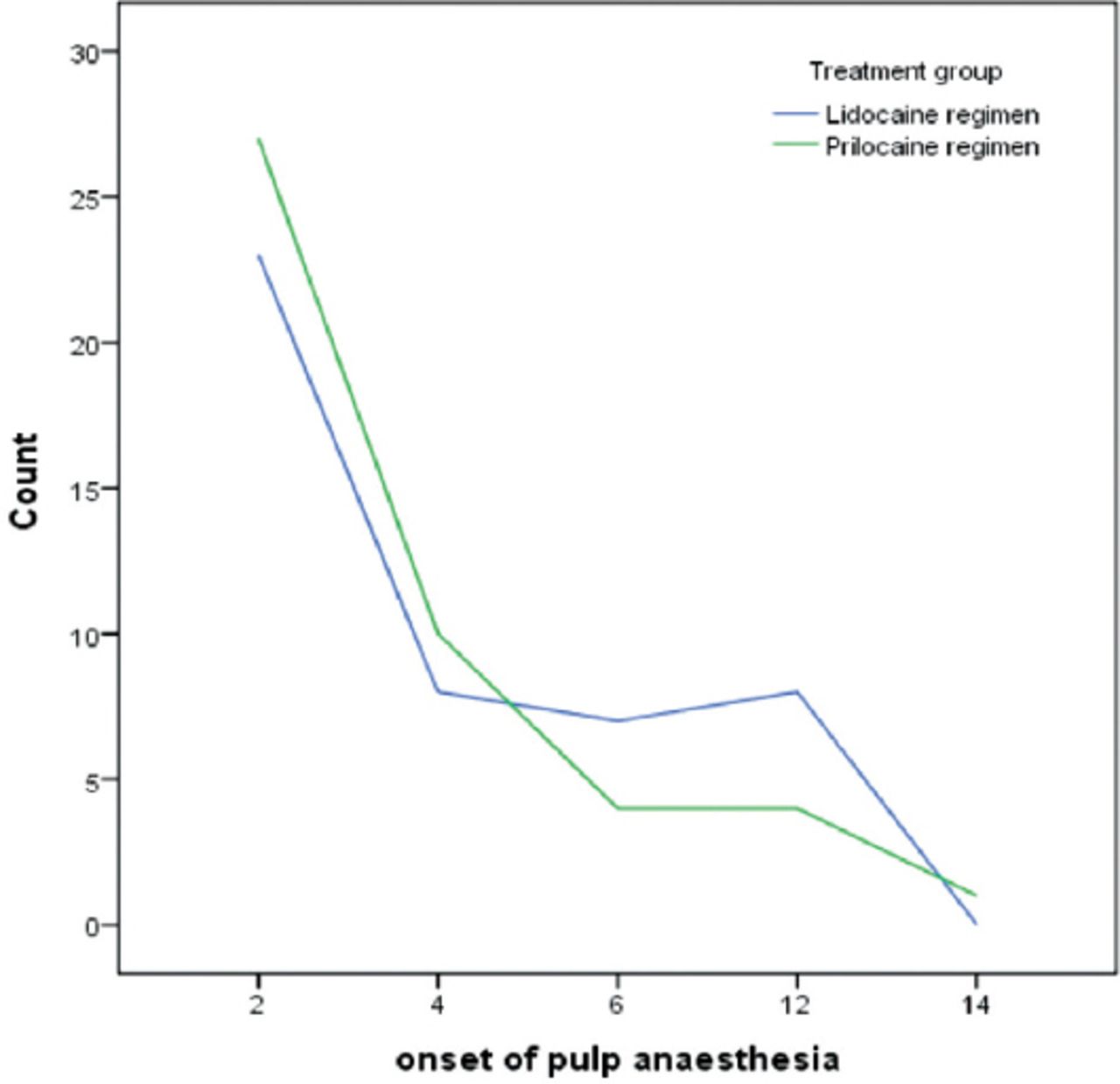
Number of patients recording upper tooth pulp anaesthesia (1 x 64 stimulation without sensation) with time after lidocaine and prilocaine buccal infiltration.
Comparisons between mean onset time of pulpal anaesthesia and extraction of the patients for lidocaine and prilocaine infiltration groups.
Discussion
Lidocaine and prilocaine have the best ranking by the US Food and Drug Administration to be used as local anesthetic agents for special patient populations.8 Although the findings of St. George et al10 reported that 2% lidocaine with 1:100,000 epinephrine was superior to 3% prilocaine with 0.03 IU felypressin when surgical procedures were performed, the outcome of this study revealed that both prilocaine and lidocaine possess a similar potency and onset time of action.
Adrenaline is considered as strong vasoconstrictor when it is compared with felypressin.5,11 The advantage of using the adrenaline in the local anesthetic agents is to minimize blood flow in the injection site, holding the local anesthetic in place, and reducing the rate of plasma uptake and potential toxicity.5,11,12 Therefore, addition of adrenaline to lidocaine will cause longer duration of action than felypressin with prilocaine. However, prilocaine is lesser vasodilator than lidocaine.11 This merit will overcome the weakness of felypressin as vasoconstrictor and it will prolong length of action and increase depth of anesthesia for prilocaine.5,11 Plain prilocaine have a milder vasodilatory effect than most other amides. It can be a good choice for patients for whom vasoconstrictor is contraindicated.6,12,13 Moreover, prilocaine is less toxic than lidocaine. Since prilocaine is also metabolized in the lungs and kidneys, it is metabolized more easily by the liver than lidocaine or mepivacaine. In addition, it clears the kidneys more rapidly than other amides.5,13
The discussion is consistent with the results from a previous study conducted by Abu-Mustafa et al.12 Their study investigated the effects of lidocaine 2% with epinephrine 1: 80,000, prilocaine 3% with Felypressin 0.03 IU/ml, and mepivacaine 3% plain on hypertensive patients during dental extraction. The results showed that prilocaine 3% with felypressin 0.03 IU/ml is safe to use in patients with stage I hypertension.
Action of adrenaline on heart includes increased systolic and diastolic pressures, increased cardiac output, increased heart rate, increased strength of contraction and increased myocardial oxygen consumption.5 Moreover, there is evidence that epinephrine injected during dental local anesthesia increases blood glucose levels and reduces plasma potassium levels.8,11 Potassium level is very important in patients on diuretic therapy who may be potassium depleted. Use of epinephrine-free solutions will avoid these problems.7,11
In high risk patient, adrenaline may cause acute hypertensive crisis, angina, arrhythmia or MI and uncontrolled diabetes.5,8 Accordingly, prilocaine is considered as a least vasodilator and can be a good choice for patients whom vasoconstrictor is contraindicated. Felypressin is less vasoconstrictive than adrenaline and constricts venous outflow.8,12 Felypressin is considered to have fewer hemodynamic effects than adrenaline.8-14
This study provided strong evidences for using prilocaine with felypressin as a substitute local anesthetic for patients who have contraindication to the use of local anesthesia with adrenaline.
Prilocaine has a better clinical performance in terms of providing rapid dental anesthesia and earlier teeth extraction than lidocaine but the differences were not significant. Prilocaine with felypressin could be a good choice for patients who have contraindication to the use of lidocaine with adrenaline.
This study has no female participants. Therefore further study with male and female participants might have more solid results.
Acknowledgement
We would like to acknowledge all the dentists, dental assistants, receptionists, oral and maxillofacial unit staff involved with local anesthetic extraction service in College of Dentistry, Taibah University, Al Madinah Al Munawwarah, Kingdom of Saudi Arabia for their help and advice.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 13, 2018.
- Accepted November 6, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.