


Abstract
Objectives: To compare the efficacy of ShotBlocker and cold spray in reducing intramuscular (IM) injection-related pain in adults.
Methos: A prospective, randomized, controlled study carried out between January 2018 and March 2018 at the Department of Emergency Medicine, Acibadem Mehmet Ali Aydinlar University, School of Medicine, Istanbul, Turkey. Adult patients receiving IM injection of diclofenac sodium (75 mg/3 ml) were included. The patients were randomized into 3 groups: ShotBlocker, cold spray, and control. Each group comprised 40 patients. Patients were instructed to rate the intensity of IM injection-related pain using a 100-mm visual analog scale (VAS). Visual analog scale scores of the patients were statistically analyzed.
Results: Visual analog scale scores were lower in the ShotBlocker (11 mm) and cold spray (10 mm) groups than in the control group (31 mm) (p=0.001). There were no significant differences in VAS scores between the ShotBlocker and cold spray groups. The operators’ responses revealed that ShotBlocker was more difficult to administer than cold spray.
Conclusion: ShotBlocker is an effective non-pharmacological method that reduces IM injection-related pain and is similar in efficacy, to cold spray.
Intramuscular (IM) injection is an invasive hospital intervention that causes substantial pain.1 Intramuscular may impair adherence of patients to treatment.2 Intramuscular injection-related pain results from mechanical trauma and a sudden increase in pressure, owing to the introduction of the needle and administration of the substance directly into the muscle. Previous studies have investigated the pharmacological and non-pharmacological methods that reduce or prevent this type of pain.3 The major pharmacological methods for reducing IM injection-related pain include the administration of topical anesthetic agents and application of cold spray. The use of topical anesthetics is limited in the emergency department (ED) due to low and slow analgesic effects, risk of systemic toxicity, and local side effects.4,5 Cold sprays effectively reduce pain, are safe for both healthcare providers and patients, and do not cause local tissue injuries. ShotBlocker is a plastic device with several short and blunt contact points on its surface that contact the patient’s skin. Non-pharmacological methods such as cold spray and ShotBlocker (Bionix, Toledo, Ohio) reduce pain via gate control theory during the administration of IM injections. The use of the ShotBlocker device has no reported side effects.6-9
Cold sprays are a well-established method used to reduce IM injection pain. We thus aimed to evaluate the efficacy of ShotBlocker and cold spray in reducing IM injection-related pain in adult patients. The primary endpoint of the study was the pain scores obtained after injection in ShotBlocker, cold spray, and non-interventional groups. We aimed to evaluate whether the ShotBlocker was user friendly, and we thus considered the secondary endpoint as the operators’ perceptions on the use of ShotBlocker and cold spray.
Methods
This study was conducted on 120 patients between January 2018 and March 2018 in the Department of Emergency Medicine, Acibadem Mehmet Ali Aydinlar University, School of Medicine, Istan bul, Turkey. Ethics committee approval has been received from the institution (decision number 2017-11/2). The study was guided by the Declaration of Helsinki and its latest amendments. The center was a tertiary care hospital with 60,000 emergency admissions annually.
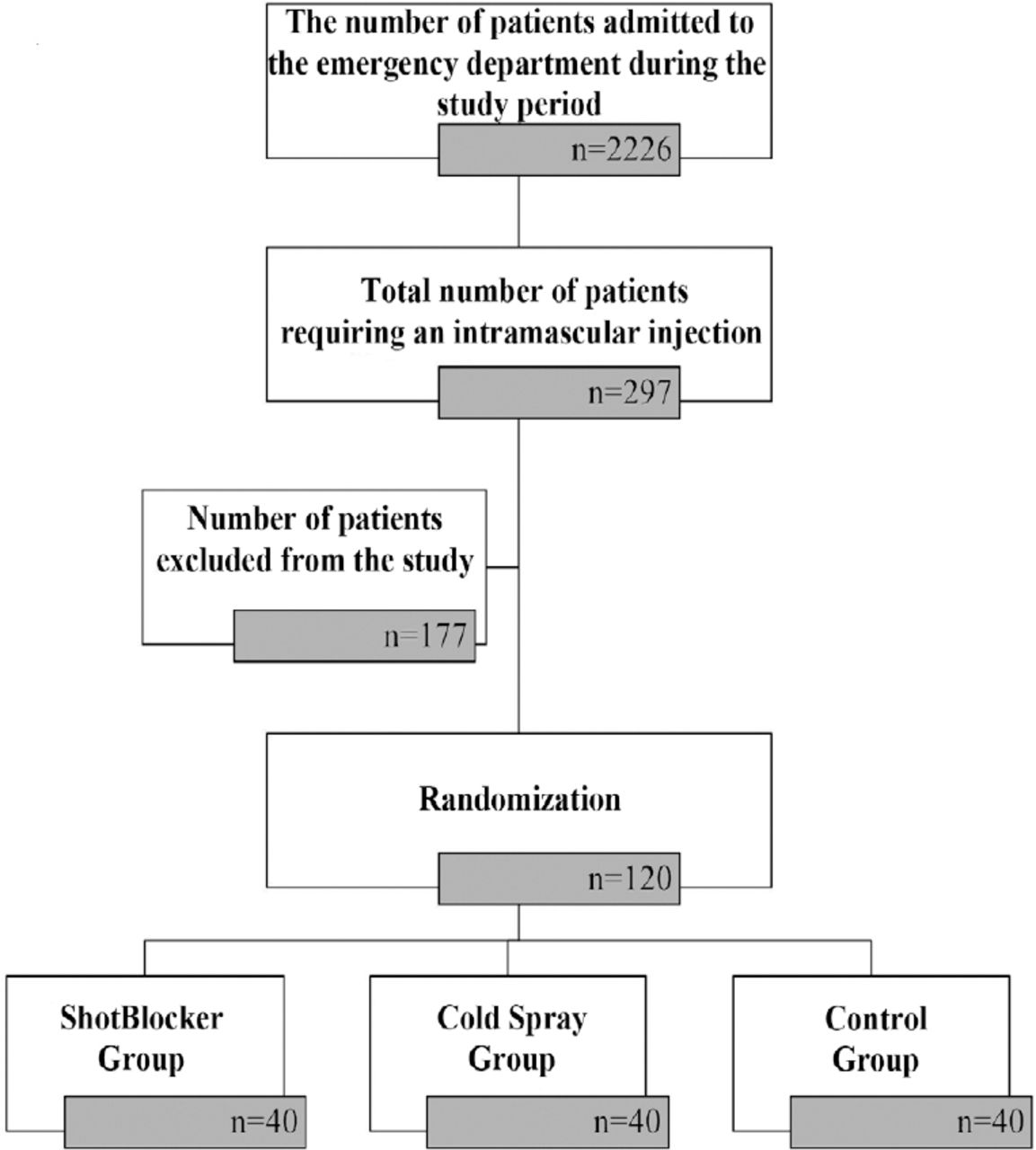
Adult patients who were admitted to the ED due to either the administration of already prescribed medications (diclofenac sodium, 75 mg/3 ml) or those who were to receive an IM injection as ordered by the ED physician, participated in the study. They were randomized into 3 study groups, each consisting of 40 patients. The flowchart of the study is presented in Figure 1.

Flow diagram of the study.
The inclusion criteria were patients aged 18 years or more who signed the informed consent form and were admitted to the ED for administration of prescribed medications or who were scheduled to receive an IM injection as ordered by the ED physician.
The exclusion criteria of the study were pregnant women, those with mental retardation and hearing or vision problems, those presenting to the ED with complaints of anxiety or trauma (soft tissue traumas, multiple traumas, or bone fractures due to traffic accidents or falls), those who experienced alterations in consciousness, those with clinical conditions requiring emergency interventions, secondary injuries, and infections at the site of injection, those who received a previous injection in the same area within the last 24 hours (h), those who experienced failure in the injection procedure at the first attempt, and those who declined to provide informed consent for the study.
The database on ShotBlocker was searched on PubMed and Google Scholar Academic. There were 7 studies that have been conducted on Shotblocker. We reviewed these studies to obtain efficacy and safety data on ShotBlocker.
Prior to the study, the investigators conducted a 2-h theoretical and practical training on 2 separate groups of emergency service nurses (n=14) regarding the study protocol and instructions on the use of ShotBlocker (Bionix, Toledo, Ohio) and cold spray (Anticare Cold Spray, BSN Medical Limited, the UK).
Adult patients who approved the informed consent form were randomized into 3 groups: the ShotBlocker group, cold spray group, and control group. The randomization list was generated via block randomization.10
When 90% power and 0.05 2-sided margin of error were assumed, 27 patients were included in each group based on a difference in 16-mm visual analog scale (VAS) score and 18-mm standard deviation, as reported in previous studies. The study has been conducted on 120 patients and 3 groups each comprising 40 patients.11
Standard IM injection procedure
As the gluteal region is confined to the limits defined by the iliac crest, coccyx, and gluteal folds, it was arbitrarily divided into 4 equal-sized areas, among which the upper outer quadrant was considered the site of IM injection. The patient was placed in a prone position and instructed to rotate their feet inward, with the big toes of either foot opposing each other. The injection area was undressed appropriately, and muscle relaxation was examined via palpation. The area of intervention was sterilized with 2% chlorhexidine solution as preparation for the procedure. All injections were standardized and were performed by emergency department nurses. The medication was administered within 15 second (sec), at a rate of one ml/5 sec. Intramuscular injections were performed using a standardized method in which a green catheter (21 gauge, 1.5 inches) and a 5-ml syringe were used to administer the medication at a 90° angle at the injection site.
Control group
The standard IM injection procedure was applied to this group.
ShotBlocker group
In this group, the device was placed just below the intervention site prior to injection with its opening facing upward. The injection was immediately performed with the dominant hand after the device was pressed firmly against the skin of the patient with the non-dominant hand of the operator (Figure 2).

Intramuscular injection with the use of ShotBlocker.
Cold spray group
In this group, injection was performed after administering the cold spray (Anticare, BSN Medical Ltd., East Yorkshire, UK) to the site of injection with a distance of approximately 15 cm perpendicularly. No waiting time was required for cold spray use. Operators performed the injection immediately after using cold spray.
The demographic data of the patients, including gender, age, weight, and fear of injection were recorded.
After successfully completing the procedure, the patients were instructed to label the intensity of injection-related pain using a 100-mm-long VAS for pain. A score of 0 in the VAS indicated the absence of pain, whereas a score of 100 indicated the highest level of pain intensity. The patient’s skin properties (thin/not thin) were recorded. In addition, whether the patient moved their leg during the procedure (moved/kept stable) was recorded by the operator. The user evaluated the difficulty of administering either the ShotBlocker or cold spray using a 5-point Likert scale.
Statistical analysis
All statistical tests were performed using IBM SPSS Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL., USA). Descriptive statistics are presented as numbers and percentages for categorical variables. Numerical variables are presented as mean, standard deviation, median, minimum, maximum, 25th percentile, and 75th percentile. The conformity of the variables to normal distribution was examined with the Kolmogorov–Smirnov test. For categorical variables, Chi-square test was used in multiple comparisons when Chi-square condition was met, whereas Fisher’s exact test when Chi-square condition was not met. Spearman correlation analysis was performed to determine the relationship among normally distributed numerical variables. Multiple group comparisons were performed with analysis of variance (ANOVA) if the data were distributed normally. Kruskal–Wallis test was used for analyzing non-normally distributed data. Post hoc analyses were performed with the Mann-Whitney U test using the Bonferroni correction. The effects of independent risk factors on VAS scores were analyzed using linear regression analysis. The initial candidate risk factors for regression model were selected according to the expert authors’ opinion. The VAS scores were evaluated for normal distribution extensively using Shapiro-Wilk test, QQ-detrended plot, histogram graph, skewness-kurtosis, and coefficient of variation being below 30%. The linearity between VAS scores and risk factors were evaluated visually using scatterplots and quantitatively using the Pearson correlation analyses for numerical variables or student t-tests for dichotomous dummy variables, where appropriate. The model fit was analyzed using residual analyses and goodness-of-fit statistics. The residuals were evaluated for normal distribution and homoscedasticity. The results of the linear regression analyses were summarized using parameter coefficients and statistical significance level. The upper limit of type-I error level for statistical significance (p-value) was regarded as 5% (p<0.05).
Results
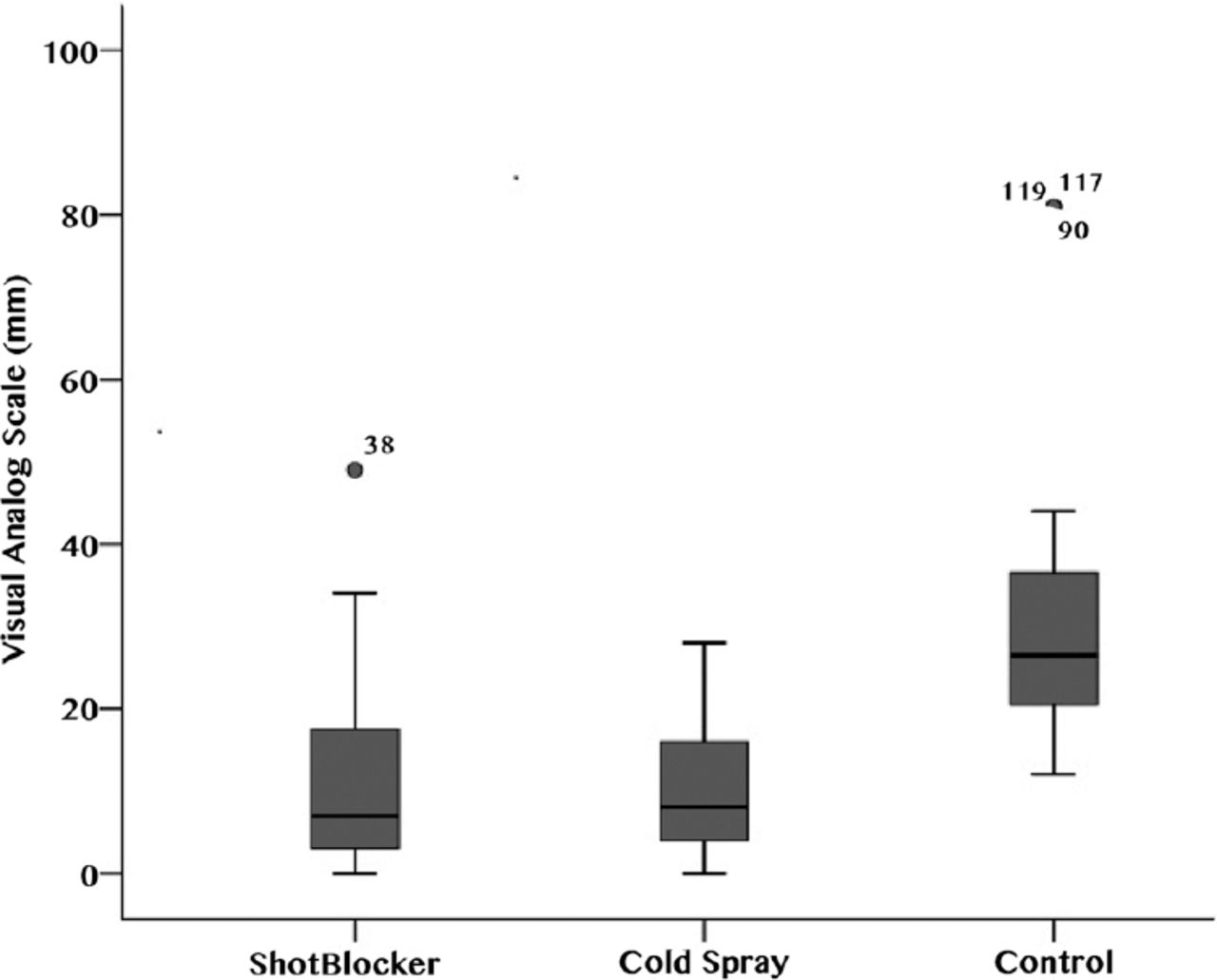
Demographic data (including gender, age, and body weight), fear of injection, and skin characteristics were similar in all 3 groups (Table 1). The VAS scores were lower in the ShotBlocker (11 mm) and cold spray (10 mm) groups than in the control group (31 mm) (p=0.001). The VAS scores of the cold spray and ShotBlocker group were found similar to each other (Figure 3).
Intergroup analysis of the demographic data and clinical characteristics of study groups.

Mean pain scores of the ShotBlocker, cold spray, and control groups.
No significant differences were observed in VAS scores according to gender and skin characteristics among the study groups (Mann–Whitney U test; p=0.467 and p=0.408). In the ShotBlocker and cold spray groups, the VAS scores were significantly higher in patients with fear of injection than in those without (Table 2). When the VAS scores of the 3 groups were examined according to age and body weight, no significant differences were observed (Table 3).
Group-based Statistics for visual analog scale.
Correlation between age and weight based on visual analog scale scores according to the study groups
Operator difficulties in using ShotBlocker were reported by the users as follows: “it was not difficult at all” (n=8/40), “mildly difficult” (n=16/40), “moderately difficult” (n=11/40), and “very difficult” (n=5/40). Operator difficulties associated with the use of cold spray were reported by the users as follows: “not difficult” (n=37/40) and “slightly difficult” (n=3/40). Other degrees of difficulty were not selected by operators in the cold spray group.
The linear regression analysis performed to define the risk factors affecting the VAS scores revealed that fear of injection was a significant risk factor increasing the severity of VAS scores both in the ShotBlocker (p=0.002) and cold spray groups (p<0.001). On the other hand, fear of injection was not found as a significant risk factor increasing the VAS scores in the control group (p=0.061). The results of the linear regression analyses of the study groups are presented in Table 4.
Results of the linear regression analysis in the study groups.
Discussion
Different methods that reduce IM injection-related pain in both adult and pediatric patients have been reported. Prior experiences of patients, pH, osmolality, viscosity, speed of injection, and chemical properties of the drug have been associated with this type of pain.7,11 The gate control theory was described by Melzack and Wall.12 This theory proposes that a painless physical input, such as warm-cold application, compression, vibration, acupuncture, or transcutaneous electrical nerve stimulation, closes the gates to painful input in the central nervous system, thereby preventing painful stimuli. This method can alternatively induce stimuli that inhibit pain sensations. In ShotBlocker and cold spray applications, the gate control theory may underscore the mechanisms of action by which IM injection-related pain is attenuated.
ShotBlocker can be used as a non-pharmacological method in the ED during injections for reducing pain. ShotBlocker is a plastic material that is compressed to the site of injection during the procedure, and the injection is performed through the space at the center. The ShotBlocker has several short and blunt contact points on its surface which contact the patient’s skin. When the device is pressed against the skin, these contact points stimulate the small-diameter, fast-conducting nerve fibers. However, the requirement for pressing ShotBlocker with one hand has been considered a complicating factor.
In the study by Celik et al,7 the effects of ShotBlocker in reducing pain associated with IM injection of diclofenac sodium, VAS scores were lower in the ShotBlocker arm (7 mm) than placebo (20 mm) and control (26 mm) arms. Our study was conducted on a population with identical characteristics. Our data were compatible with the results of Çelik et al.7 Both studies indicated that ShotBlocker was an effective method to reduce pain caused by IM injection of diclofenac sodium. Furthermore, our study demonstrated that the use of either the cold spray or ShotBlocker reduced IM injection-related pain. No side effects were observed in any group. ShotBlocker was found to be more difficult to apply than the cold spray.
Mawhorter et al13 have applied cold sprays or +4°C saline-impregnated cool cotton balls as placebo at the site of injection to compare the effects of these distinct applications on IM injection-related pain during vaccine administrations. The study concluded that the administration of topical cold spray prevented pain. According to the results of our study, the administration of cold spray contributed to reduction of IM injection-related pain intensity. No complications were observed during the application of cold spray in our study. However, Mawhorter et al13 reported flammability and fluorocarbon content as limiting factors of cold spray administration. Since both ShotBlocker and cold spray effectively reduce pain, ShotBlocker is the preferable option as it is not constrained by any limiting factors.
Irkoren et al14 reported that a significant reduction in the intensity of pain induced by botulinum toxin injections on the forehead was achieved with the use of a topical anesthetic cream and ethyl chloride-containing cold sprays. Similarly, cold spray application reduces the intensity of pain in arteriovenous fistula procedures as effectively as a topical anesthetic cream.15 Moreover, cold sprays decrease the intensity of IM injection-related pain in pediatric patients.16 The results of this study are in accordance with the results of studies conducted on different populations comprising different age and race groups.5,9,16 These studies have collectively demonstrated that cold sprays can reduce the intensity of injection-related pain without causing any complications, and that they are effective in different age groups and body regions when used in different interventional procedures. Nevertheless, patients’ allergies should be taken into consideration when adopting this approach.
In a randomized controlled study comparing the ShotBlocker and control groups, Caglar et al17 evaluated the perception of pain in neonates during IM injections of hepatitis B vaccine. Pain scores in the ShotBlocker group (1.64±0.80) during IM injections were lower (p<0.001) than control group (2.96±0.73), indicating that the use of ShotBlocker reduced the intensity of acute pain.17 In our study, the use of ShotBlocker in the adult group reduced IM injection-related pain; thus, ShotBlocker appears to be effective across different age groups.
Chung et al18 reported that compression applied with the fingers at the site of injection over the deltoid muscle before injections was associated with lower pain intensity scores compared to those for conventional IM injections. Compression with the fingers may adopt the same mechanism in gate control theory as that of the ShotBlocker mechanism.
The relationship between pain and anxiety has been described in the literature, which has revealed that a reduction in the severity of anxiety using non-pharmacological methods may lead to a reduction in pain intensity.19,20 A notable finding of our study is that the use of ShotBlocker and cold spray in patients with fear of injection led to a significant increase in VAS scores. Patients with fear of injection may benefit more from an anxiolytic drug than from cold spray or ShotBlocker prior to injection. Further, inclusion in a clinical study may be an anxiogenic factor.
Study limitations
This study was conducted at a single center, which limits its generalizability; this is considered a major limitation. The anxiety scores of the participants were not evaluated, which is another limitation of the study. In addition, the non-pharmacological methods used in the study were not compared with pharmacological methods, and a placebo group was not included.
In conclusion, the use of ShotBlocker and cold spray can be effective in reducing pain during injections. Neither of these methods caused complications; however, the use of ShotBlocker was associated with application difficulties.
Further studies may be beneficial to facilitate the use of ShotBlocker in routine practice.
Acknowledgment
The authors gratefully acknowledge Editage (www.edditage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 25, 2019.
- Accepted September 15, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.