


Abstract
Objectives: To determine the survival outcomes and to describe the epidemiological characteristics of patients with colorectal cancer (CRC) in western Saudi Arabia.
Methods: Our study is a retrospective analysis of patients with CRC diagnosed between 2002 and 2014. We recruited 279 patients who were selected randomly and followed until the end of July 2017. A Kaplan-Meier curve was used to estimate the survival rate for CRC patients according to gender, histopathological pattern, tumor site, and mutation type, taking into consideration time factor, dropouts, and loss to follow-up.
Results: The mean age of CRC patients was 57±13 years, and most of them were Saudi (87.5%). Regarding tumor epidemiology, 32.4% of the patients at Best American Joint Committee on Cancer (Best AJCC) stage 4; 28.9% were at stage 3; and 1.2% were at stage zero. The most frequent pathological variant was adenocarcinoma (77.4%); the most affected site was the rectum (40.5%). By Cox regression analysis, age at diagnosis, tumor stage, Kirsten Ras (KRAS) mutation, and lymphovascular invasion were significant prognostic factors for survival in CRC patients.
Conclusion: Colorectal cancer patients presented to the hospital late in the disease course. This may call for lowering the screening age, increasing awareness programs, and establishing a national screening program.
Cancer is considered a significant health problem, and it is among the leading causes of mortality and morbidity worldwide.1 The burden of non-communicable diseases is a major threat and continues to be a huge challenge to health-care systems. This is highlighted in the countries of the Gulf region despite the considerable improvements in health services and may be primarily due to unfavorable changes in the lifestyle, such as the high consumption of fast food, minimal physical exercise, and increasing tobacco use. Advanced colorectal cancer (CRC), breast cancer, leukemia, and thyroid cancer are the most common cancers affecting people of the Gulf region compared with other countries.2 Colorectal cancer is one of the most common malignancies and a major health burden worldwide. Genetic and environmental factors play important roles in the development and increased incidence of CRC. Colorectal cancer mortality rates differ significantly worldwide. Internationally, CRC is ranked as the third diagnosed cancer among males and the second among females. Approximately 1.5 million patients were diagnosed with CRC, and the estimated death rate was more than half a million in 2012.3 The incidence of CRC varies significantly worldwide, with the highest incidence rates found in the US, Canada, Europe, and Australia; the lowest rates are found in South-Central Asia and Africa.4 These geographic variations appear to be a result of variances in diet along with environmental exposures that are expressed genetically, as seen in studies of migrants moving from low- to high-risk areas. In the US, the incidence of colorectal cancer has been steadily decreasing by 2% to 3% per year over the last 15 years, and the mortality rate has progressively decreased.5 The incidence of colon and rectal cancer was 42.4 cases per 100,000 population per year in the US, and the incidence of estimated new cases was 132,700 people in 2015.6 Approximately 0.5 million Americans die of CRC yearly, almost 8% of all cancer deaths.7 The establishment of surveillance programs in the US lead to improvement in the outcome of CRC. The surveillance programs include detection of CRC cases at an early stage, removal of colonic polyps, and more effective primary and adjuvant treatments. Surprisingly, recent data from the US Surveillance, Epidemiology, and End Results (SEER) database and other European cancer registries conclude that CRC, predominantly rectal cancer, incidence in the under 50 years of age population is growing, whereas they report decreasing incidences in the older population.8 Other registries suggest a rising incidence of CRC among young adults 20 to 39 years of age, even though these incidences are still low compared with the 50 years and above population.9,10 In most western regions, the incidence rates have been stable or increased slightly over the last 15 years. However, in countries categorized as low risk, including Spain and some countries in Eastern Asia and Eastern Europe, CRC incidence rates have rapidly increased.4,11 Data of CRC from Saudi Arabia have shown a steady increase in incidence and presentation of the disease in younger age groups according to recent studies.12,13 Many previous research studies have suggested that CRC at a young age is associated with advanced stage of the disease and higher mortality rates compared with CRC at an older age. According to data and researcher knowledge, the most recent local studies for survival analysis of CRC patients were conducted by Al-Ahwal et al12 and Alsanea et al13 for the period 1994 to 2004. There is a gap of knowledge for the survival rate analysis and the associated predictors related to outcomes of CRC, and the researchers assumed that incidence of patients presented with advance stages will be high, particularly in the absence of an established awareness program about CRC and screening programs in Saudi Arabia.
The objectives of this study were to determine the survival outcome of CRC patients at King Faisal Specialist Hospital and Research Center (KFSHRC), Jeddah, Saudi Arabia during 2002 to 2014, and to assess the possible predictors affecting survival outcome.
Methods
This study was conducted in the city of Jeddah, at King Faisal Specialist Hospital and Research Center, after receiving ethical approval (no. FMR-04-39-H), on 19 April 2017, from the Institutional Review Board of Faculty of Medicine in Rabigh, Saudi Arabia.
A retrospective analytical study of CRC patients diagnosed between 2002 and 2014 was conducted, for which a representative random sample of all diagnosed cases of CRC during that period was included in the study. We calculated the sample size using a Cox regression of the log hazard ratio (HR) on a covariate with a standard deviation of 1.0. A sample size of 279 achieves 91% power at a 0.05 significance level to detect a regression coefficient equal to 0.2 (namely, HR of 1.2).14
We generated a list of all the 877 CRC cases, and then we randomly selected our 279 cases from the list. We then calculated the overall survival (OS) period from the date of diagnosis to the date of death or last follow-up in months using the Kaplan-Meier method. The date of the patient’s last hospital contact was determined from electronic hospital records, which included clinic and drug dispensing visits, in cases of loss to follow-up. A data collection sheet developed by the researchers following many literature reviews was used for gathering data of CRC patients. These data were obtained from patients’ files and electronic records of the Oncology Department Registry at KFSHRC, Jeddah, Saudi Arabia. The data included age, gender, nationality, residency, date of initial diagnosis, date of last contact, cause of death, stage and grade of disease, histopathological site and characteristics, presence of lymphovascular invasion, family history, tobacco history, presence of Kirsten Ras (KRAS) mutation, and comorbid diseases. The patient data were evaluated and classified at presentation, including the stages, which were coded as described by the American Joint Committee on Cancer (AJCC) fifth and sixth editions according to the tumor, node, and metastasis (TNM) stage.
We included in our study all patients diagnosed with CRC, both gender, and all nationalities. We excluded other type of cancers. Colorectal cancer cases were classified according to the International Classification of Diseases for Oncology (ICD-O 3rd edition) as colon (codes C18.0-C18.9 and C26.0) or rectum (codes C19.9 and C20.9). Colon tumors were further designated by location as proximal (codes C18.0 and C18.2-C18.5), distal (codes C18.6-C18.7), or other (codes C18.1, C18.8, C18.9, and C26.0).
The categorical variables are presented as frequency and percentages, and the quantitative variables are presented as mean and standard deviation (SD). The Chi-square test and the Fisher exact test were used to explore the associations between the mortality of CRC patients with various demographic and clinical variables. The survival pattern of CRC patients was presented using a Kaplan-Meier survival curve. A Cox regression proportional hazard model was used to identify significant predictors of CRC. The data were analyzed using IBM SPSS Statistics Version 24.15
Results
Our study included 279 patients; the sociodemographic data are shown in Table 1. Almost half of the patients (48.7%) came from Jeddah region. Other regions: Madinah, 14.9%; Makkah, 11.3%; and only 4% from the Jizan and Taif regions. More cases from other regions such as Tabouk, Abha, and Albaha regions were also recorded.
Sociodemographic data of colorectal cancer patients.
Regarding family and smoking history, 38.4% of the diagnosed patients had no other family member with CRC; 57% did not know about their family history; and only 4.7% had at least one member of their family with CRC. Approximately 20% of the studied patients never smoked; 7.9% were still smoking; and 3.6% were ex-smokers. Considering the general health status and comorbidities, 23% of patients in our sample were hypertensive, 19.3% were diabetic, 12.9% had KARS mutation, and only 4.7% had ischemic heart disease.
Regarding tumor epidemiology, The epidemiology of CRC is illustrated in table 2, the result indicate that the majority of CRC was adenocarcinoma and the most frequent presentation was stage 3. Most of the tumor were located primarily in the rectum and the most frequent grade was grade 2. With regard to lymphovascular invasion, 44.4% of the cases were unknown or undetermined, and 22.9% were positive. Further, 44.3% of the sample patients with recorded KRAS mutation were positive; there were approximately 200 cases with unknown data regarding this mutation (Table 2). With regard to survival outcome of the studied patients, death was recorded for 55 patients (19.7%); 47 (85.5%) deaths were directly due to cancer-related causes; 3 patients (5.5%) died due to causes indirectly related to cancer; and 5 patients (9.1%) died due to other causes.
Tumor data of colorectal cancer patients treated at King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia in the year 2002-2014.
Table 3 shows the relation between the different patient/tumor characteristics and patient survival. American Joint Committee on Cancer stage was the significant predictor for survival, as 34.2% of those at stage 4 had died compared with 20.7% of patients at stage 3, 11% of patients at stage 2, and none of the patients at the other stages (p=0.001). Regarding age at diagnosis, 22.2% of those who were diagnosed below the age of 40 years had died compared with 21.2% of those who were diagnosed above 60 years, with no statistical significance. As for gender, the death rate was insignificantly higher among females than among males (22.8% and 13.7%). Considering nationality, 20.9% of the Saudi patients had died compared with 11.4% of non-Saudi patients (p>0.05). The death rate among current smokers was slightly higher than among ex-smokers and non-smokers. Regarding tumor grade, the highest death rate was recorded among patients with tumor grade 1 followed by patients with grade 3 and then patients with grade 2 with insignificant difference (p>0.05). As for primary site, 25.9% of patients with the tumor at a proximal site had died compared with 22.1% of those with the tumor in the rectal region (p>0.05). Regarding KRAS mutation, patients who were positive had higher death rates than those who did not have the mutation (34.3% versus 15.9%; p<0.05).
Predictors of survival among patients with colorectal cancer treated at King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia in the year 2002-2014.
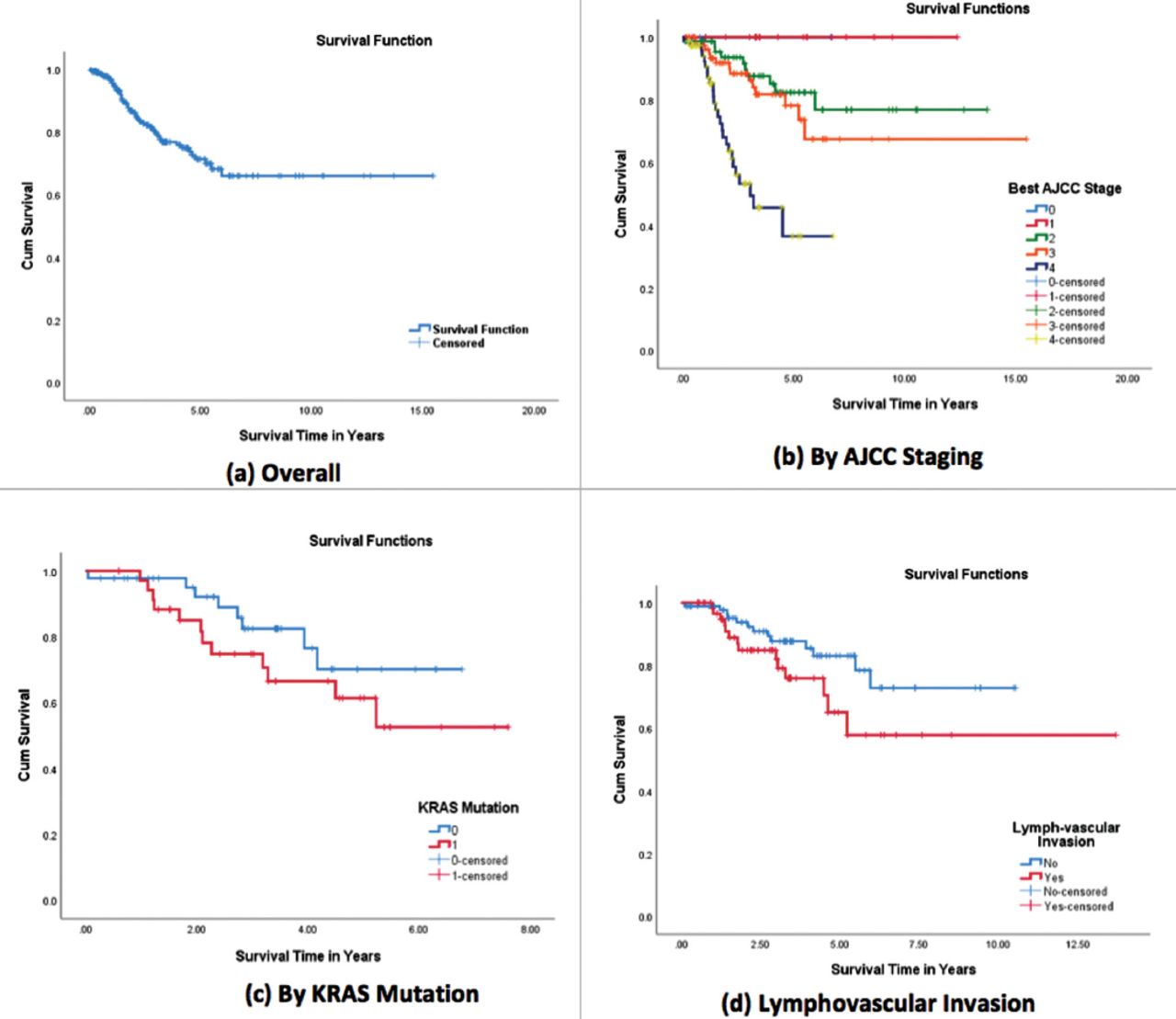
The overall survival rate of the studied patients decreased over time, with survival years ranging from 10 to 12 years, with an average of 11 years. The 5-year survival rate was approximately 69% (Figure 1A). With regard to survival rate according to AJCC staging, patients at stage zero had an average survival time of 6 years, and 85% had 5 years of survival. Patients at stage 4 had an average survival time of 4 years, and 61% had 5 years of survival (Figure 1B). As for the survival rate according to KRAS mutation, the survival years among patients with positive mutation status ranged from 4 to 6 years with an average of 6 years; and 61% of patients with positive mutation survived for 5 years. As for those patients without the mutation, the survival time ranged from 5 to 6 years with an average of 5 years; 61% survived for 5 years (Figure 1C). Significantly poor survival times were observed in patients with lymphovascular invasion (Figure 1D).

Kaplan-Meier curves for overall survival and by significant predictors among patients with CRC treated at King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia in the year 2002-2014. AJCC - American Joint Committee on Cancer, KRAS - Kirsten Ras, CRC - colorectal cancer
The Cox regression analysis included all identified predictors for patient survival, among which age at diagnosis, cancer staging, KRAS mutation, and lymphovascular invasion were the most important predictors for survival keeping all other factors constant (Table 4). As for age at diagnosis, a higher age at diagnosis was associated with a 1.03 times higher probability of death compared with patients diagnosed at a younger age (HR=1.03; 95% confidence interval [CI]: 1.01-1.05). While patients with higher cancer AJCC staging had tripled risk of death compared with those at lower stages (HR=3.05; 95% CI: 2.01-4.6). Also, patients who had KRAS mutation had doubled risk for death compared with those without the mutation (HR=2; 95% CI: 1.01-5.30). Patients with lymphovascular invasion had a higher risk of death than those without (HR=1.11; 95% CI: 1.03-1.19). All these factors had a significance value less than 0.05 when keeping all other predictors constant.
Results of Cox regression model for identifying predictors of survival among patients with colorectal cancer treated at King Faisal Specialist Hospital and Research Center, Jeddah, Saudi Arabia in the year 2002-2014.
Discussion
The incidence of colorectal cancer is related mostly to non-modifiable risk factors, mainly to age and hereditary factors. In other words, the CRC incidence increases after 40 years of age, and continues to increase after age 50.15,16 Although 90% of CRC affects people who are more than 50 years old,17,18 the incidence seems to be growing more among young people.6 This study showed that the mean age for presentation of CRC patients to KFSHRS was 57 years (95% CI: 44-70 years), and there was a slight male predominance (55.5%) over female (44.1%) among diagnosed cases. Although the majority of cases presented at an age older than 50 years (Table 1), the percentage of patients younger than 50 years (32.3%) was relatively high. According to a national survival study in Saudi Arabia conducted by Al-Ahwal et al,12 which included 549 cases during the period 1994 to 2004, the mean age of the patients diagnosed with CRC was approximately 54 ± 14.7 years, and males represented 66.9%. Similar findings were obtained from an epidemiological study that included 4201 CRC patients between 2001 to 2006 based on a cancer registry. The study concluded that the mean age of patients at the time of diagnosis was 58 years.19 Another national study by Alsanea et al13 that analyzed the Saudi Cancer Registry data of CRC for the period 1994 to 2010 showed that the median age at presentation was approximately 60 years (95% CI: 57-61 years) for men and 55 years (95% CI: 53-58 years) for women. It also showed a higher proportion among males compared with females, with an average ratio of 116:100 over the study period. These previous studies agreed with our findings that CRC patients present at a younger age with high male-female ratio. The reason for younger mean age at diagnosis among Saudis compared with Americans (68 years for male and 74 years for female) and other developed countries requires further studies. This finding may be related to the presence of risk factors such as sedentary lifestyle and obesity, dietary habits, and smoking; or, it may be a reflection of a younger Saudi population compared with western countries.
This study has found that 23% of CRC patients were hypertensive and 19.3% were diabetic, and the researchers assumed that the actual percentage may exceed that due to a possible under reporting of these conditions in the medical records. There is strong evidence that metabolic syndrome (obesity, diabetes, hypertension, and dyslipidemia) is associated with greater risk of CRC, and there is a theory correlating the worldwide epidemic of metabolic syndrome with the increasing incidence of CRC. A recent population-based study showed that CRC patients with diabetes or hypertension are at a greater risk of recurrence of cancer after treatment and have a worse survival outcome compared with those who do not have either condition.20
Study limitations
The main limitations of this retrospective study were patients who were lost to follow-up. There was also missing information regarding predictors of survival due to insufficient patient data.
In conclusion, the 5-year overall survival for CRC patients during the years 2002 to 2014 was 69% at KFSHRC in Jeddah, which may reflect improvement in medical management and an overall higher quality of care. Colorectal cancer patients presented at younger age to hospitals and were diagnosed in late stages. These findings may call for lowering the screening age, increasing awareness, establishing a national screening program, and increasing access to specialized medical facilities.
Acknowledgment.
This project was funded by the Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, Saudi Arabia (Grant no. 43-828-1440). The authors, therefore, acknowledge with thanks DSR for technical and financial support. We would also like to thank Elsevier Language Editing Services for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Saudi Arabia (Grant no. 43-828-1440).
- Received August 6, 2019.
- Accepted October 29, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.