


Abstract
Objectives: To evaluate the relationship of the first and second mandibular molar roots to the inferior alveolar canal (IAC) and cortical plates using cone beam computed tomography (CBCT) in the Saudi population.
Methods: Scans of 60 patients were collected retrospectively from the dental hospital database in King Saud University, Riyadh, Kingdom of Saudi Arabia. Measurements of the right and left first and second mandibular molars for each dental root and the mandibular bone thickness were determined. The position of the IAC was estimated using axial, coronal, and sagittal views. Three examiners performed the measurements independently.
Results: The mean distance between the root apices of the mandibular molars and the IAC ranged from 1.68-4.79 mm, whereas the mean distance from the outer surface of the buccal cortical plate to the buccal root surface ranged from 2.33-6.72 mm. Similarly, the mean distance from the outer surface of the lingual cortical plate to the lingual root surface ranged from 2.62-4.80 mm. Finally, the mean distance from the outer surface of the lingual cortical plate to the outer surface of the buccal cortical plate was 11.93-13.19 mm.
Conclusion: The measurements reported in this study may be of value to practitioners treating Saudi patients, as they need to be familiar with the distance of the mandibular first and second molars in relation to the IAC and surrounding cortical plates to accurately assess and plan endodontic surgeries, surgical extractions, and implant placements.
The inferior alveolar canal starts from the mandibular foramen in the medial side of the mandibular ramus and descends downward and forward obliquely towards the body of mandible at which it becomes horizontally oriented. It contains a neurovascular bundle that includes the inferior alveolar nerve (IAN), which runs through the canal and branches into the mental nerve. The IAN exits the mental foramen, and the incisive nerve continues through the mandibular incisive canal.1 The inferior alveolar canal has variant forms and courses that affect its proximity to adjacent structures.2 Studies agree on the high proximity of the posterior teeth, especially the mandibular second and third molars. Injury to neural tissues within the IAC is a possibility during multiple dental procedures, including dental implant placement, tooth extraction, endodontic surgeries, and even during non-surgical root canal treatment.3-6 The extraction of third molars has been reported to be the most common reason for IAN injury.7 Implant placements cause IAN injury more frequently than endodontic intervention, however, when combined, they cause injury at a rate lower than that of third molar extraction.8 The most common reasons for non-surgical endodontic associated IAN injury are: 1) over instrumentation that mechanically traumatizes the nerve; 2) presence of endodontic points or sealants in the IAC causing pressure; 3) and chemical irritation from endodontic medicament or sealants.9 It is therefore important to understand the relationship of the IAC with its adjacent structures, particularly the root apices of adjacent teeth, as well as the buccal and lingual cortical plates.
Several methods have been used to evaluate the relationship of the IAC to its adjacent structures, including cadavers and conventional panoramic and periapical radiographs.10-13 However, these methods have limitations with regard to the availability of sufficient samples and the accuracy of measurements. More recently, cone beam computed tomography (CBCT) has been used in the evaluation of the relationship between the IAC and its adjacent structures.14 Cone beam computed tomography is a 3-dimensional imaging modality that offers the advantage of observing anatomical structures clearly without any of the superimpositions and distortions that can be seen in conventional imaging.15 In recent years, there has been a widespread use of CBCT in dentistry, mainly due to lower costs, shorter imaging time, smaller unit size, and the lower dose of radiation that is emitted in comparison with conventional computed tomography (CT).13,16 Cone beam computed tomography has been shown to be both a reliable and accurate method to obtain linear measurements for preoperative treatment planning.13,14,17
Previous studies have evaluated the position of the IAC in relation to the mandibular third molars in the Saudi population for extraction purposes.18-19 The objective of this study was to evaluate the relationship of the mandibular first and second molar roots to the IAC and cortical plates using CBCT in the Saudi population.
Methods
The College of Dentistry Research Center (CDRC), King Saud University, Riyadh, Saudi Arabia approved this research. The CBCT data of patients were retrieved from the oral and maxillofacial radiology database of King Saud University Dental Hospital, Riyadh, Kingdom of Saudi Arabia, between January 2014 and December 2016. Patients of Saudi origin who had both their right and left first and second mandibular molars intact and who were 18 years of age or older were included in this study. The exclusion criteria for this study were as follows: 1) presence of a lesion at the region of interest (ROI); 2) history of orthodontic treatment, bone loss, or a defect in the ROI; 3) evidence of external or internal root resorption; 4) radiographic evidence of skeletal or dental malocclusions; 5) evidence of abnormal anatomy of the roots; and 6) endodontic treatment had been previously performed on the teeth in the area of interest.
All CBCT scans were obtained using the Planmeca Promax® 3D Max digital dental imaging device (Planmeca, Helsinki, Finland) with an isotropic voxel size between 0.2-0.4 mm. The assessment of various anatomical structures and measurements were performed using Planmeca Romexis® 3.6 imaging software (Planmeca, Helsinki, Finland). Images were viewed on a 30.4 inch TFT AM Color LCD Dual Domain IPS medical display Coronis Fusion MDCC-6130 (Barco, Belgium) at a resolution of 3280x2048. All measurements and analyses were performed by an oral and maxillofacial radiologist, along with 2 general practitioners who were trained by the oral and maxillofacial radiologist.
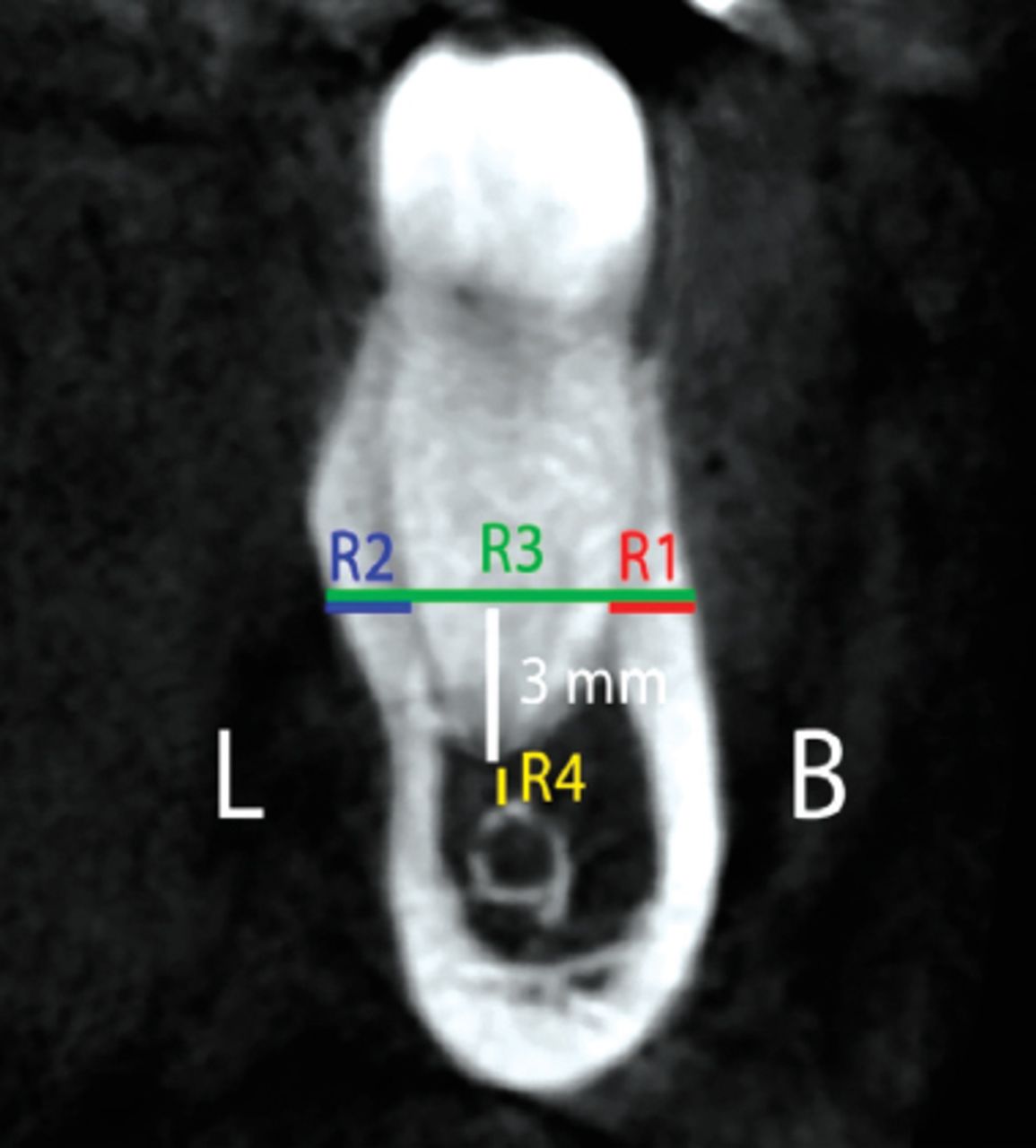
Measurements were obtained at 3 mm coronal to the apex for each root of the right and left first and second mandibular molars for each patient. After aligning the coronal and sagittal planes with the long axis of each root, the mandibular bone thickness was measured as follows: Firstly, the distance from the outer boundary of the buccal cortical plate to the buccal root surface was measured (R1); secondly, the distance from the outer boundary of the lingual cortical plate to the lingual root surface was measured (R2); and thirdly, the total bone thickness including the root was then quantified (R3). Additionally, the position of the IAC was determined using axial, coronal, and sagittal views. The shortest distance from the outer surface of the cortical boundary of the inferior alveolar canal to the nearest root surface was measured for each root (R4) (Figure 1).

Cone beam computed tomography cross-section of a mandibular molar root. The buccal (R1) and lingual (R2) cortical plate measurements are shown. The total bone thickness including the root (R3) and the distance to the IAC (R4) are also included. R1 - distance from the outer boundary of the buccal cortical plate to the buccal root surface, R2 - distance from the outer boundary of the lingual cortical plate to the lingual root surface, R3 - total bone thickness including the root, R4 - shortest distance from the outer surface of the cortical boundary of the inferior alveolar canal to the nearest root surface.
A pilot study was conducted in order to determine the inter- and intra-examiner reliability between the 3 examiners. Nine cases were selected at random and were blinded by an independent clinician. The examiners were required to perform the measurements for the selected cases twice within a one-week time interval. The inter-examiner correlation was high (r=0.99) with a p-value of <0.01. Also, the correlation coefficient between the examiners was excellent (r: >0.92; p<0.05). A paired t-test showed high intra-examiner reliability, as there was no significant difference between the first and second readings performed by each examiner. Cronbach’s alpha indicated a reliability among examiners of approximately 0.83-0.92 (p<0.05).
An independent t-test was used to compare 2 independent groups. A Chi-square test was used to test the association between categorical variables, and the Pearson correlation coefficient (PCC) was used for measuring correlation. For data analysis, we use the Statistical Package for Social Sciences software Version 20.0 (IBM Corp., Armonk, NY, USA) for Windows. A p-value of <0.05 was considered significant.
Results
A total of 60 patients, 36 males (60%) and 24 females (40%), were included in this study. The mean age of the patients was 29.59±14.08 years (18-78 years). The mean distance between the root apices of the mandibular molars and the IAC ranged from 1.68-4.79 mm. The mean distance from the outer surface of the buccal cortical plate to the buccal root surface ranged from 2.33-6.72 mm. The mean distance from the outer surface of the lingual cortical plate to the lingual root surface ranged from 2.62-4.80 mm. The mean distance from the outer surface of the lingual cortical plate to the outer surface of the buccal cortical plate ranged from 11.93-13.19 mm (Table 1). The mesial root of the first molar was in contact with the IAC in one case (1.7%), while the distal root was in contact in one other case. The mesial root of the second molar was in contact with the IAC in 15 cases (25%), and the distal root was in contact in 23 cases (38.3%).
Mean distance measurements of the mandibular first and second molars to the buccal and lingual cortical plates and the IAC (in mm).
There were no significant differences in any of the mandibular first and second molar measurements between the right and the left side of each patient (p<0.05) (Table 2). A shorter distance between the root apices of the first and second mandibular molars in relation to the IAC (R4) was observed in a greater number of female patients compared to male patients; such distances were statistically significant in the distal root of the second molar (p<0.05). There was a statistically significant difference between female and male patients in terms of the overall distance between the buccal and lingual cortical plates (R3) at the distal root of the mandibular second molar (p<0.05) (Table 3). A Pearson product-moment correlation coefficient was conducted in order to measure the correlation between patient age and root distance. Subsequently, this demonstrated that there was a moderate positive correlation in all root distances with respect to the IAC (R4), as well as the mesial root distance of the second molar in relation to the lingual cortical plate (R3) (r=0.3-0.4, n=60, p<0.01).
Mean distance measurements of the mandibular molars in relation to the buccal and lingual cortical plates and the IAC (in mm) according to patient side.
Mean distance measurements of the mandibular molars in relation to the buccal and lingual cortical plates and the IAC (in mm) according to each gender group.
Discussion
Dental practitioners need to be familiar with mandibular first and second molar distances in relation to the IAC and the surrounding cortical plates to accurately assess and plan endodontic surgeries, surgical extractions, or the placement of implants in such areas; even non-surgical endodontic treatment in this area is prone to cause IAN injury, mechanically or chemically.9 The management of such injuries can range from patient reassurance to surgical debridement, depending on the severity of the damage and the speed in which corrective intervention was provided.20 Surgical correction is an effective treatment for such injuries, especially in cases were endodontic material such as calcium hydroxide been extruded.21
In the present study, we anatomically analyzed the first and second mandibular molars using CBCT. This technology was chosen for its ability to provide superior visualization of structures with respect to the molar teeth, the IAC, and the cortical plates.
In the current study, we found that the distance from the root apices to the IAC increased, moving anteriorly from the distal root of the second molar to the mesial root of the first molar. This result is in agreement with that of Aksoy et al,22 who examined the proximity of mandibular teeth to the IAC and found that the second molar is significantly closer to the IAC compared to the first molar and premolars. They also found that the second molar is in direct contact with IAC in 16% of cases, whereas only 3.3% of the first molars were in contact with the IAC. Burklein et al,14 have also found similar results. Our results showed that direct contact of the mesial root was present in 25% and distal root was present in 38.3% of the second molars to the IAC of cases; however, there was only one case in which the distal root of the first molar was in direct contact with the IAC and one other case in which the mesial root was in contact. The number of second molars that were in contact with the IAC in our sample was large compared to that in previously mentioned studies. This could possibly be explained by our sample age distribution, in which most of our subjects (45 subjects, 75%) were younger than 30 years. Previous studies have demonstrated that age affects the proximity of the IAC to the roots of the mandibular teeth, with younger patients having shorter distances between the teeth and IAC.14,22-24 An increase in this distance with age is likely due to the fact that the craniofacial complex continuously changes throughout life.22 Swasty et al,25 demonstrated a continuity of mandibular molar vertical maturation with increasing age (40-49 years), followed by a subsequent reduction in these measurements. Because of the skewed age distribution in our sample, we could not statistically assess age as a factor; however, we did observe a tendency for the distance to increase with age.
When comparing measurements of the mandibular first and second molar teeth from the right and the left side of each patient, we found no significant difference (p<0.05), which is consistent with the findings of both Burklein et al,14 and Kawashima et al.24
Several studies have shown that female patients display a shorter distance between the IAC and the roots of the mandibular molars in comparison with male patients.14,22-24,26 Moreover, female patients tended to have a thinner horizontal mandibular bone width.26 In our study, we found that females tended to exhibit shorter distances in relation to the IAC when compared to males, and it was statistically significant at the distal root of the mandibular second molar.
Further multicenter studies with a larger sample size comprising a greater age and ethnic distribution are needed to confirm the impact of these variables and to overcome our research limitations.
In conclusion, the findings of the current study have revealed the close proximity of the second mandibular molar to the IAC, especially in the distal root. The study has also highlighted significant differences in this relationship with regard to gender. Understanding such anatomical variations will help dental practitioners with pre-surgical assessment and in the planning of treatment pertaining to the first and second mandibular molars. Thus, the findings of this research may facilitate better treatment planning strategies for Saudi patients undergoing dental procedures, including dental implant placement, tooth extraction, endodontic surgeries.
Acknowledgment
The authors gratefully acknowledge the RAED program at King Saud University, Riyadh, Kingdom of Saudi Arabia, for their support.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 10, 2018.
- Accepted December 25, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}