


Abstract
Objectives: To assess the outcome of a myringoplasty procedure during a 5-year period at a tertiary teaching hospital in Abha, Kingdom of Saudi Arabia.
Methods: All patients with chronic suppurative otitis media (CSOM) who underwent elective myringoplasty between August 2012 and February 2018 were included in the study. Patients were investigated preoperatively and postoperatively by pure tone audiometry (PTA). The patients’ demographic data were collected together with the surgical outcome. Postoperatively, patients were followed at the first week, at 6 weeks and then every 3 months, thereafter for one year.
Results: A total of 67 myringoplasty procedures were performed during the period of study. There were 41 females and 26 males, and they had an age range of 16-60 years and a mean age of 32.37±12.95 years. Preoperative PTA indicated that 58 (86.6%) patients had a hearing gap >20 dB. However, after surgery, only 9 (13.4%) patients remained with hearing gaps >20 dB. The success rate of graft stability at the end of one year was 94% with significant difference p=0.0001. However, one patient of the 4 patients with failed graft stability demonstrated graft atrophy, and the remaining 3 developed graft infection.
Conclusion: Myringoplasty remains a useful technique for the management of CSOM. However, it depends on the surgeon’s skills and expertise and on the site of perforation. The success rate of myringoplasty in this study was comparable with that of the quoted literature.
Myringoplasty is an otological surgical procedure in which the perforated tympanic membrane (TM) is repaired.1 The usual cause of TM perforation is infection or trauma. Perforation may lead to hearing impairment, recurrent ear discharge and hearing that requires myringoplasty. It aims to reconstruct the TM and restore the hearing mechanism over the intact and mobile ossicles with cessation of otorrhea.2 It is presently one of the most popular otological operations over the world, and it uses an underlay technique and temporalis fascia graft.3 Though it is a very common and established procedure, it has several known prognostic factors that may affect the surgical outcome, such as the age of the patient, site and size of the perforation, type of graft, technique (underlay versus overlay), surgical approach (transcanal versus postauricle), experience of the surgeons, and condition of the ear (dry versus wet).4 Its success rate in the literature shows variation but it is approximately 95%.5 The quest is to improve the results further by studying the different factors that could possibly affect the outcome. Therefore, this study aims to describe the outcome of myringoplasty over the last 5 years at a tertiary teaching hospital in Abha, Kingdom of Saudi Arabia, in terms of the hearing gap, size of TM perforation, and tympanoplasty graft uptake.
Methods
Approval from the Research and Ethics Committees at the College of Medicine, King Khalid University at Abha, Kingdom of Saudi Arabia, was obtained. A retrospective study design was followed. Data from patients undergoing myringoplasty surgical operation between August 2012 and February 2018 was collected. The data included age, gender, type of operation, hearing gap, size of TM perforation, tympanoplasty graft uptake, and postoperative complications. Fisher’s 95% confidence intervals (CI) were calculated for the proportions. Pearson’s Chi-square test was used as a test of significance at the 5% level. The inclusion criteria included patients of myringoplasty surgery over the last 5 years at Aseer Central Hospital in Abha, Kingdom of Saudi Arabia. Patients with safe-type CSOM with a good cochlear reserve, good eustachian tube function, patients with audiogram gap between 20 and 40 dB were selected. The exclusion criteria included patients with unsafe otitis media of CSOM or any cochlear or ossicular involvement, patients less than 16 years of age, patients with audiogram gap more than 40 dB and all patients who underwent the procedure by consultants. A pure tone audiogram was performed preoperatively and postoperatively for all patients. The operations were performed under general anesthesia using a microscope. The inlay technique was used for all perforations; the perforation was approached via postauricular incision, and we used either the temporal muscle fascia or thin tragus cartilage graft with its perichondrium, with different hands on surgery. All patients were followed after the surgery at the first week, at 6 weeks and then every 3 months for one year. The audiogram was performed on the 6th and 12th week and was used to assess the outcome of hearing objectively. The outcome of hearing was assessed subjectively by asking each patient for a self-assessment of the hearing outcome. Microsoft Excel 2018 was used for the data entry, and Statistical Package for Social Sciences (SPSS) version 20.0 software (IBM Corp., Armonk, NY, USA)was used for the data analysis. Fisher’s 95% CIs were calculated for the proportions. Pearson’s Chi-square test was used as test of significance at the 5% level.
Results
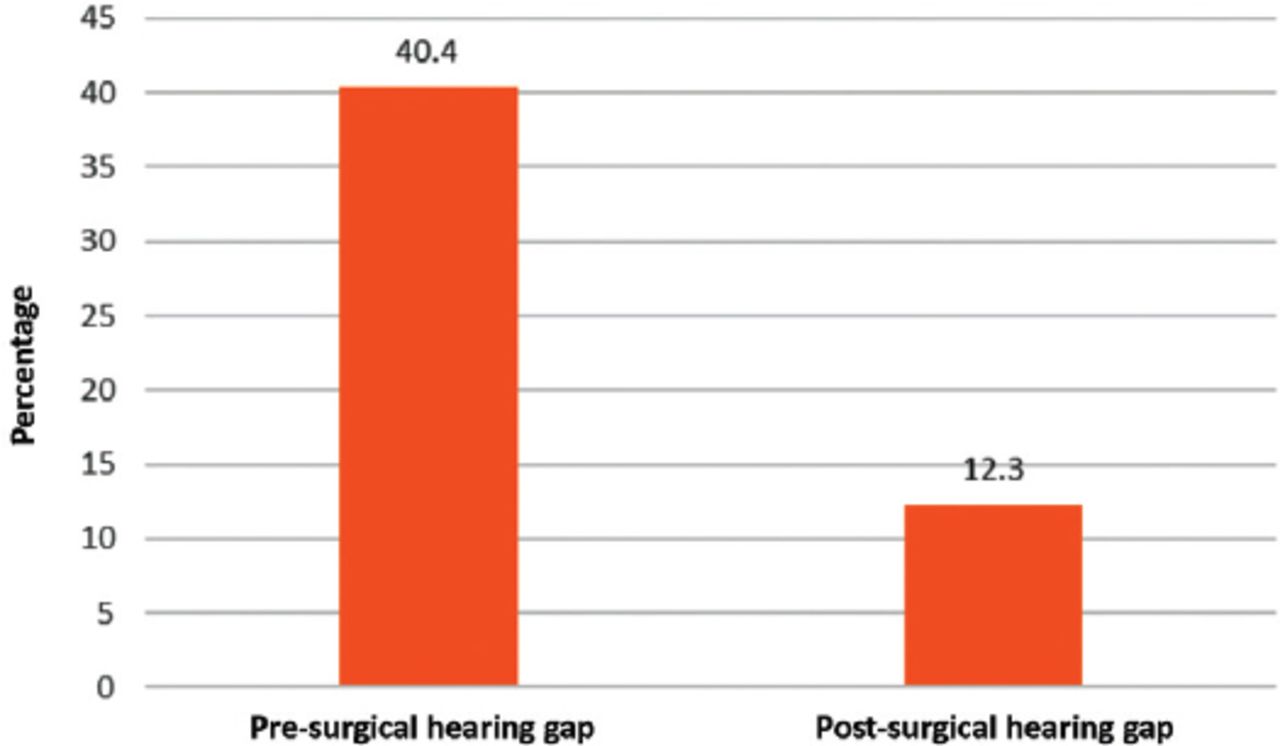
During the period of study, 67 patients underwent myringoplasty, including 41 females and 26 males (male:female ratio of 1.6:1). Forty-one percent found to be male and 26% are female, and they had a mean age of 32.37±12.95 years (range: 16-60 years). The myringoplasty procedure was performed on the right side in approximately half of the patients (n=34, 50.7%) and on the left side in 33 patients (49.3%). Three patients developed graft infection, and all of them were treated conservatively. In this series, the success rate of the graft at the end of one year was 94% with significant difference (p≤0.0001). However, the graft failure rate in all of the patients was 6% (Table 1). Comparison between preoperative and postoperative hearing gaps. (Figure 1). Graft failure was shown in 3 (4.5%) patients with anterior perforation and in one (1.5%) patient with total perforation, and this difference was found to be statistically significant (p=0.05) (Table 2).
Success rate and infected graft rate.

Comparison between preoperative and postoperative hearing gaps.
Types of tympanic membrane perforation.
Discussion
Myringoplasty is indicated to restore hearing ability as well as to prevent recurrent ear otorrhea.6 The present study analyzed the outcome of 67 patients who underwent myringoplasty at a tertiary teaching hospital in Abha, Kingdom of Saudi Arabia, during the last 5 years. There was a female predominance of the procedure among our patients (61.2%). This finding also has been reported by Indorewala et al,7 who explained that females have been found to pay more attention to their health than males. Tympanic membrane perforations were mainly of the anterior type (44.8%), while 13 patients with these had subtotal perforation (19.4%). The least common type was posterior perforations (28.4%). In all, 1.5% of patients with these had attic TM, while 19.4% of these patients had chronic mastoiditis. The results of the present study showed that TM perforations were mainly anterior, or subtotal, while the least affected sites were the posterior, total and attic types. However, graft failure was shown in 3 (4.5%) patients with anterior perforation and in one (1.5%) patient with total perforation, and this difference was found to be statistically significant. Maharjan et al,8 indicated the importance of the perforation site. They stated that the perforation site corresponds to the degree of hearing loss, with posterior perforations having a greater dB level of hearing loss, which is likely a result of the loss of protection of the round window membrane from impinging sound pressure waves. In our study, preoperative PTA indicated that 58 (86.6%) patients had a hearing gap >20 dB. However, after surgery, only 9 (13.4%) patients remained with hearing gaps >20 dB. Five patients of the nine with a persistent hearing gap were found to have a healed graft. This indicates that some patients may not improve even though their graft healed. Udaipurwala et al,9 stated that hearing loss in CSOM usually results from the middle ear pathology and that the inner ear is typically unaffected. The prevalence of hearing improvement after surgery among our patients was better than that reported by several studies. The prevalence of hearing loss of CSOM ranges from 9-83%.10 Sergi et al,6 reported that 57-97% improvement in hearing function for patients of myringoplasty. Another prospective study by Philips et al,11 was conducted involving multiple hospitals in the United Kingdom (UK) showed the overall closure rate for myringoplasty was 98.9%. The results of the present study showed that almost all grafts were intact postoperatively (94%). However, partial graft defect and nonintact grafts occurred in 6% of patients, while graft complication or infection occurred in 3 patients. Indorewala et al,9 reported that complete graft uptake occurred in 98.6% of patients, and more than 86% of patients had improvement of hearing function postoperatively. However, Andersen et al,12 reported a graft uptake rate that was 93.0%. In our study, the graft uptake rate was 94%. Multiple factors may affect the outcome of myringoplasty, like the age of the patient, site and size of the perforation, type of graft, surgical technique, experience of the surgeons, and condition of the ear whether it is dry or wet.2 Mandour et al,13 compared the use of the fat graft to the cartilage graft the reported success rates of 92% fat graft and 88% of cartilage graft. In our study, 2 important factors had an effect on the outcome of myringoplasty: the surgeon’s skills and expertise and the site of perforation. There are different surgical approaches of myringoplasty by transcanal or postauricular using endoscope, or microscope. Different study showed no significant differences.14-15 It is likely that multiple factors affect the success rate of myringoplasty, including the experience of the surgeons and site and size of the perforation. However, the technique remains useful for hearing improvement and prevention of ear discharge. Limitation of this study is that procedure has been carried out by different surgeons.
In conclusion, myringoplasty remains a useful technique for the management of CSOM. However, its outcome depends on the surgeon’s skills and expertise and on the site of the perforation. The technique remains useful for hearing improvement and prevention of ear discharge. The success rate in this study is comparable with that of the quoted literature.
Acknowledgment
The authors gratefully acknowledge Dr. Muhammad A. Khan, Department of Medical Education, King Khalid University, Riyadh, Saudi Arabia for his valuable assistance with the statistical analysis. We would like to thank American Journal Experts for the English language editing.
- Received September 7, 2018.
- Accepted December 25, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.