


Abstract
Objectives: To compare use of ultra-fast high-pitch dual-source free-breathing computed tomography pulmonary angiogram (CTPA) with conventional standard-pitch single-source breath-hold CTPA.
Methods: This retrospective comparative study was conducted in Radiology Department at King Fahad Military Medical Complex Dhahran, Saudi Arabia from July 2016 to December 2017. Patients (N=130) were divided into 2 groups, each having 65 consecutive patients; Group-1 (single-source CT) and Group-2 (dual-source CT). Previously treated pulmonary embolism cases, pregnant patients and those with incomplete data were excluded. Image quality was subjectively assessed by 2 readers for adequacy of contrast opacification and pulmonary vessel outline, and presence of artifacts (breathing motion, cardiac pulsation, and contrast related). Scan acquisition times and radiation doses were also compared. Chi-square and t-test were used to determine association.
Results: Improved image quality (optimal studies without artifacts 91%) was seen in Group-2 compared to Group-1 (optimal studies without artifacts 75.4%). Also, reduced scan time (1-2 sec.) and radiation dose (mean dose length product (DLP)-248 mGy-cm) were observed in Group-2 compared to Group-1 (scan time- 6.5 sec, mean DLP-375). Results were found significant (p<0.05).
Conclusion: High-pitch dual-source CT with free-breathing yields better image quality, reduces image acquisition time and radiation doses.
Pulmonary embolism (PE) is a life-threatening condition, if left untreated.1 Clinical presentation may be acute or chronic, and commonly associated with deep vein thrombosis (DVT).2 Acute pulmonary embolism is the third most common cardiovascular emergency, after coronary artery disease and stroke.3 Symptoms can be non-specific and may include shortness of breath, rapid breathing and chest pain. Patients with PE who received mechanical ventilation, cardiopulmonary resuscitation, and thrombolytic treatment have very high mortality rates. However, patients stable enough for diagnostic procedures have mortality rates of 1 to 2%.4 With introduction of helical CT, diagnosis of pulmonary embolism relies mostly on pulmonary computed tomography angiography (CTA).5 Computed tomography pulmonary angiogram (CTPA) has become the imaging method of choice in diagnosis of acute PE and has advantages over conventional pulmonary angiography and nuclear (ventilation-perfusion, V/Q) study as it is fast, non-invasive and now widely available modality capable of directly visualizing emboli, and may provide an alternate diagnosis. Image quality, scan time, contrast volume, and radiation dose remain important considerations with CTPA imaging, that lead to development of Spectral CT (also called dual-source or dual-energy CT). Dual-source CT with 2 X-ray tubes and 2 detectors has the potential to overcome limitations of conventional CT systems, particularly speed and temporal resolution.6 Tube voltages can be reduced and modified, and further reductions can be made by using enhanced data processing methods like iterative reconstruction (IR) algorithm that uses cyclic image processing reducing noise.7 Conventional single-source CT scanners require a short period of breath-hold to ensure motion-free imaging of the pulmonary arteries. However, breath-hold is associated with loss of contrast enhancement within the pulmonary arteries due to valsalva induced changes in hemodynamics along vena caval system.8 On high-pitch dual-source scanner, 2 image datasets are acquired in quick succession, reducing motion artifacts even with free-breathing that can be of particular significance in older age groups, patients with co-morbidities or lung disease or those who are unable to follow breath-hold commands.9 Volume of contrast administered can be minimized due to speedy scan acquisitions coupled with appropriate injection techniques resulting in optimal contrast enhancement and opacification of pulmonary vasculature.10 Various studies have shown improved diagnostic capabilities of dual-source CT scanners in pulmonary CTA studies. Some only discussed image quality on either single or dual-source scanners, while others have individually studied the radiation dose aspects (and iterative reconstruction), contrast volumes, and utilization of dual-energy application.11-13 As we experienced a transition from a single-source to dual-source CT scanners during recent interval, we were able to observe and compare important aspects (like image quality, scan acquisition time and radiation doses) of CTPA imaging performed under each scanner technology.
There is scarcity of studies in the Kingdom of Saudi Arabia documenting this ‘information set’ formulated in a comparative manner, to validate such limited data available in literature. Therefore, we aim to highlight the use of high-pitch dual-source CT in comparison to standard-pitch (conventional) single-source CT in detection of acute pulmonary embolism in this region.
Methods
All patients with clinical suspicion of acute pulmonary embolism and subsequent CTPAs performed in the Radiology department were retrospectively reviewed for imaging techniques and findings. As the study was retrospective and did not involve disclosure of any patient information and privacy, the ethics committee of our hospital waived the need for patient consent. The study was conducted in accordance with the Helsinki Declaration. Pregnant women, patients with previously known or treated pulmonary embolism, and patients with incomplete data were excluded. All clinical and radiologic information were kept strictly confidential. Literature review was performed through electronic search (Google Scholar, PubMed).
All patients (N=130) were divided into 2 groups, each having 65 consecutive patients; those who underwent CTPA on a single-source (Group-I) and those on dual-source CT (Group-II) in a period of 18 months. Demographic information about age and gender of all patients was collected. Clinical information and radiographic/imaging findings were acquired through patients’ clinical notes/Hospital Information System (HIS) and Radiology Information System/Picture Archiving and Communication System (RIS/PACS). Initial chest radiograph findings were documented as negative (normal study) or positive (in case of demonstration of any other abnormality like pleural effusion, opacity, atelectasis, mass or consolidation).
Computed tomography pulmonary angiograms in both groups were performed on 128-slice CT machine (SOMATOM Definition, Siemens Healthcare, Germany), with source-specific parameters adopted in each group (Table 1).
CT specifications and acquisition related parameters of each
A double syringe power injector (Stellant D, Medrad, Indianola, PA) infused contrast through an accessible (antecubital, subclavian, or an internal jugular) vein access. Intravenous contrast (Iomiron, GE Healthcare, Cork, Ireland) was followed by 50ml saline at flow rate of 5ml/sec. The CT acquisition was timed by using bolus tracking for both CTPA protocols with a region-of-interest placement in the pulmonary trunk. Once a threshold of 90 Hounsfield Units (HU) was reached, the scan automatically started after a 5-second trigger delay.
All CT images were reconstructed in transverse plane, with a section thickness of 1.0mm (increment of 0.7mm), both in mediastinal window (level: 50HU, width: 355HU, medium smooth convolution kernel B26) and lung window (level: 745Hu, width: 1600HU, sharp convolution kernel B80). Images were also reconstructed in the coronal plane, with a section thickness of 1.5mm (increment of 1.5). The coronal images were reconstructed in a mediastinal window (level: 50HU, width: 350HU, medium smooth convolution kernel B30). We were able to record machine calculated thoracic dose-length product (DLP) for each examination, a product of CTDIvol (CT Dose Index; a measure of radiation dose output of a CT scanner) and scan length (in centimeters) that was measured in milligray-centimeters (mGy-cm).
Image quality was subjectively assessed for image characteristics: (i) adequacy of contrast opacification (250HU) within the main pulmonary artery (PA)/ pulmonary artery enhancement and vessel outline until subsegmental arteries, (ii) presence or absence of artifacts (cardiac pulsation artifacts, breathing/ diaphragmatic movement related artifacts, beam hardening artifacts related to residual high-density contrast along superior vena cava and right atrium or contrast column interruption). A 3-point Likert type scale (labels as Good, Fair, and Poor) was used for contrast opacification and vessel outline, and corresponding scores of 1 (Good), 2 (Fair) and 3 (Poor) were allotted. Another 3-point scale was used to assign scores for assessment of artifacts (1- Diagnostic image without artifacts, 2- Acceptable image despite presence of artifact, and 3- Non-diagnostic image due to artifacts). A score of 3 in either of 2 image characteristics was considered a suboptimal image quality.
We used a sinogram affirmed iterative reconstruction algorithm (Sinogram Affirmed Iterative Reconstruction [SAFIRE], Siemens Healthineers, Forchheim, Germany). The iterative reconstruction algorithm was set to a strength level of 5 for all CTPA protocols (as recommended by the manufacturer) and was applied to Group-2 studies (for all images). An optimal image quality was documented if image showed adequate contrast opacification, clear vascular outline and luminal content (contrast or clot), without diagnostically limiting artifacts. Image quality was interpreted by 2 readers; an experienced general radiologist (with special interest in chest imaging) and an expert thoracic radiologist, each having more than 7 years of experience, who were kept blinded of clinical information. Good inter-observer agreement was noted (with Cohen’s kappa value of 0.7), and subsequent consensus reading was carried out by these 2 radiologists. Scan acquisition times and radiation doses for each CTPA technique were also compared. The statistical analysis was carried out using Statistical Package for Social Sciences (SPSS, version 22) (IBM Corp., Armonk, NY, USA). Chi-square test and t-test were used to determine association, and p-values less than 0.05 were considered significant.
Results
In Group-I, 41 (63.1%) were males and 24 (36.9%) were females, while there were 30 (46.2%) males and 35 (53.8%) females in Group-II. Mean age was 46 years (SD=17) in Group-I and 48 years (SD=21) in Group-II. Patients in each group were categorized in age groups as well (Table 2).
Age group distribution in both CTPA groups.
Initial chest radiographs were found to be normal in 44.6% (n=29) of patients in Group-I, and 36.9% (n=24) in Group-II, while the respective remaining patients in each group were found to have abnormal findings.
Mean contrast enhancement along main pulmonary artery was found to be 330 HU with SD of 82.3. Out of 9 true positive cases of embolism in each group, more cases of central thrombi were seen (n=5, 55.5%) in Group-I, while in Group-II more cases of peripheral thrombi (n=4, 44.4%) were seen (Figures 1 & 2).

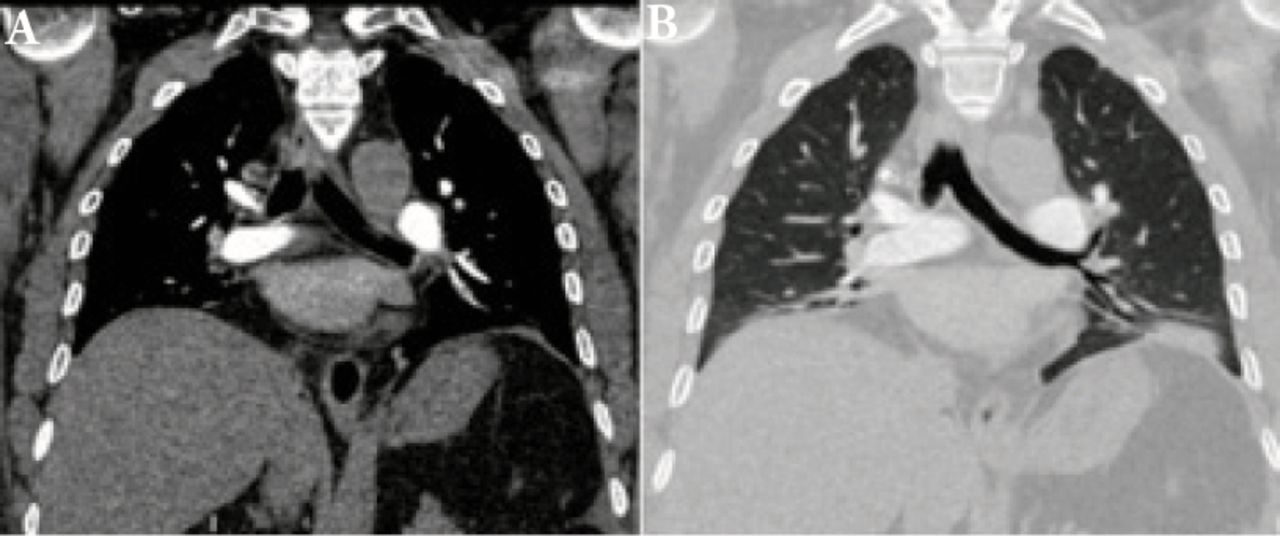
Coronal reformat images of pulmonary computed tomography angiography with A) mediastinal and B) lung windows showing a left lower lobe (peripheral) segmental thrombus with distal wedge-shaped area of dense parenchymal opacity/ infarct.

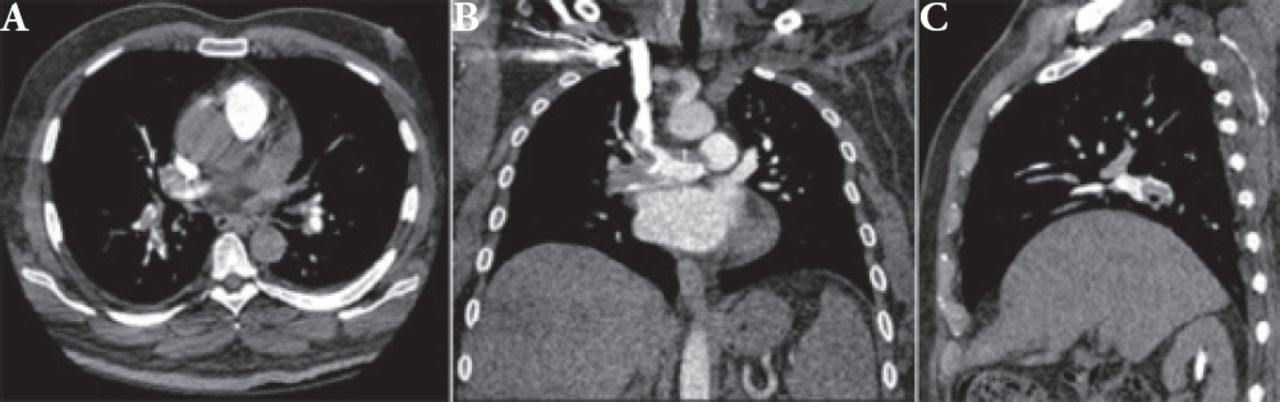
A) Axial, B) coronal and C) sagittal reformat images of pulmonary computed tomography angiography (mediastinal windows) showing both central and peripheral emboli.
Suboptimal images with artifacts were seen in 24.6% (n=16) patients of Group-I and 9.2% (n=6) patients of Group-II (Table 3). Chi-square value was calculated to be 5.45 (p-value 0.02, CI=2.43-28.02).
Image quality among both single and dual-source CT groups.
Most of the artifacts seen in each group were related to beam hardening due to high-density residual contrast within the SVC (causing streak artifacts), and motion/ breathing artifacts (Figures 3 & 4).

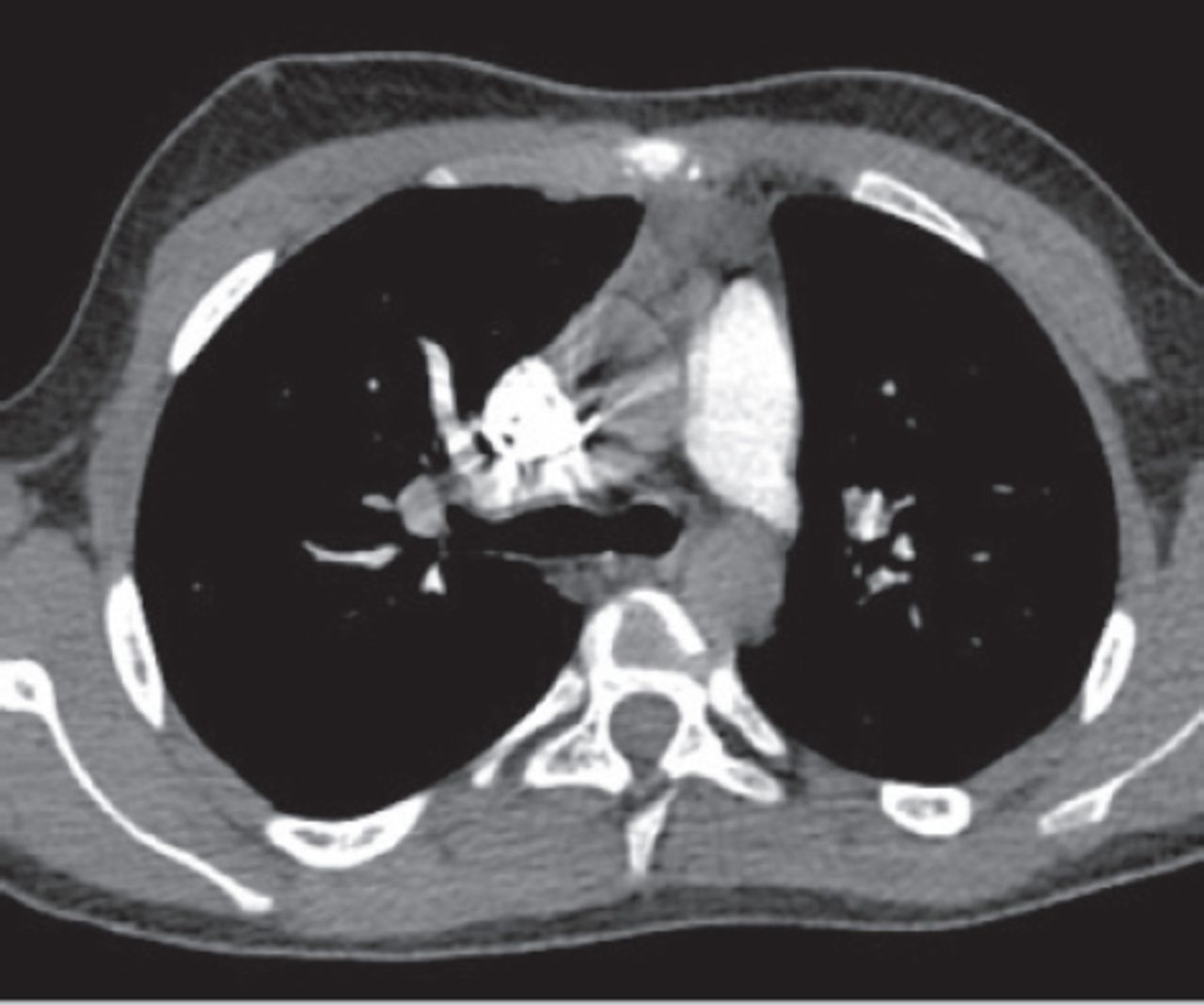
Axial computed tomography pulmonary angiogram image (mediastinal window) showing streak artifacts related to hyperdense contrast within the superior vena cava (SVC) hindering details and making it difficult to exclude right upper lobe emboli along the pulmonary artery branch. Also note subtle pulsation artifact seen along the right wall of the main pulmonary artery.

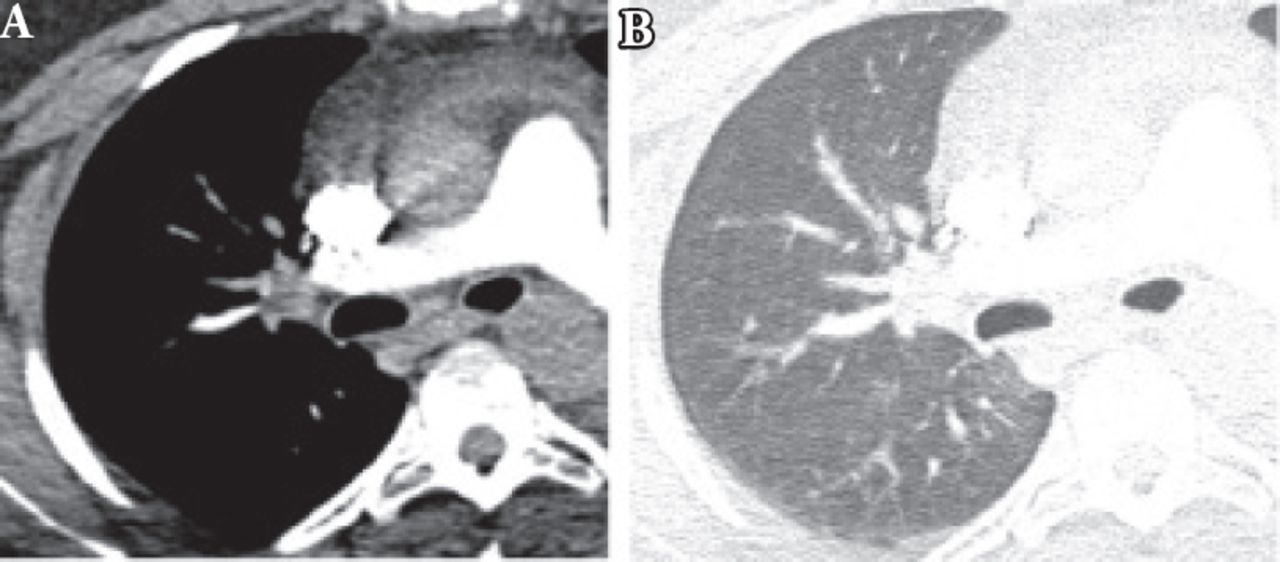
Axial computed tomography pulmonary angiogram images in A) mediastinal and B) lung windows showing blurring or ill-definition of vessels with subtle overlapping.
Scanning acquisition times were recorded in each group, that showed significantly reduced time in Group-II studies (1.1s versus 6.4s in Group-I), with p-value of 0.0005 (t-test value 14.40).
Available DLPs were documented in each group (Table 4), that showed significantly reduced radiation doses in Group-II studies, with p-value of 0.0005 (t-test value 10.72). A mean effective dose of approximately 3.4 mSv was measured (DLP x 0.014) for Group-II.
Dose length products (DLPs) in each group (n=65).
Discussion
Acute PE has a high mortality rate requiring early diagnosis and management.14 In 2014, Al Otair et al1 found a mortality of 8.6% in 105 patients at a University Hospital in Riyadh. They found surgery, obesity and immobility to be the most common risk factors.1 Young and middle age groups (20-60 years) were found mostly affected as indicated by AlGahtani et al2 amongst 341 suspected PE patients. In 2015, Al-Hameed et al3 highlighted recommendations by Saudi Association for Venous Thrombo-Embolism (SAVTE) in assessing clinical probability of DVT before going to sequential diagnostic evaluation. Clinical assessment pathways like Wells score or revised Geneva scores may help to define clinical probability for PE, and needs to be calculated prior to further imaging.15 Results of Prospective Investigation Of Pulmonary Embolism Diagnosis (PIOPED)- II suggested high predictive value of CTPA (utilizing 4-detector CT) in diagnosis of PE in patients with high probability on clinical assessment; however, additional tests might be needed in cases with low clinical suspicion.16 Nevertheless, CTA on fast-speed helical CT has been considered the imaging method of choice for evaluation of PE.17
Improved image quality with reduced dose utilizing dual-source CT scanners (enabling high pitch image acquisition) has been depicted in various studies such as Bauer et al18 in 2012 and Ajlan19 in 2016, and we were able to demonstrate similar results in our study using this scanner technology. However, it should be emphasized that obtaining an optimal image has never been a single-person or a single-step task, rather active involvement of both technologist and radiologist are needed to plan and deliver the right amount of contrast (optimization) at the right time (monitoring) in a right way (delivery technique and system) for the right subject (patient selection), to properly execute image acquisition (scanning parameters and machine settings) and to effectively use post-processing techniques. Patient condition, cooperation and understanding of procedure are also vital to obtain quality imaging. We noted that the number of patients in the older age group (61 and above) were more in dual-source group than in the single-source group (Table 1), these patients are usually unable to hold breath and at times do not follow adequate breathing instructions due to their condition, yet we found a higher sensitivity of pulmonary CTA in Group-II denoting the fact that image quality was not seen hindered by the breathing artifacts. We also observed that CT-true positive cases for PE were seen more in the younger age group (20-40 years) in Group-I (5 patients) versus 3 patients in Group-II, highlighting compliance of breath-hold instructions in these patients facilitating image quality and diagnosis.
Artifacts related to CTPA are well recognized, of these are partial volume artifacts secondary to motion/breathing or cardiac pulsation artifacts, poor contrast opacification due to mixing of opacified and un-opacified blood, beam-hardening artifacts by high density structures (like contrast in SVC and right atrium), confusion with venous structures (venous contamination) and mucous-filled bronchi.20,21 In our study, most of the artifacts in each group were related to breathing that limited the evaluation of subsegmental arteries, and beam-hardening artifacts related to residual concentrated contrast along the SVC limiting evaluation of adjacent upper lobe arteries. We observed that nearly all false positive cases in both groups (3 in group-II versus 5 in group-I) were found to have diagnosis of isolated small subsegmental thrombi, but those patients were seen discharged later on by the clinicians after improvement of symptoms (without anticoagulation) or treatment of cause other than PE, and exclusion of DVT by compression sonography. Although there are debates on clinical relevance of isolated subsegmental thrombosis in stable patients and whether to treat such patients or not, however, presence and diagnosis of such small thrombi may be important and clinically relevant to treat particularly in unstable patients with limited cardiopulmonary reserve.22 Therefore, patient selection (habitus and condition), cannulation access, contrast concentration, flow rate and volume as well as injection protocol technique/optimization (biphasic or triphasic with saline flush) and clear breathing instructions and patient coaching (prior to examination) have been advocated to better image quality and reduction of artifacts.23
It should be noted that radiation dose remains a major concern in utilizing CT studies as these are used in all age groups.24 Therefore, careful review of the clinical information and discussion with referring physician (about clinical assessment scores and laboratory results like D-dimers) are important to ensure proper justification of such studies. Post processing of raw CT data using ‘iterative reconstruction’ has been a topic of interest in the radiology platforms to further minimize dose without compromising image quality.25 We found a 40% reduction in DLPs acquired through the dual source reduced KV and at expense of reducing noise by SAFIRE software. Even further reductions in radiation doses can be possible if dual-energy is also used as studied by Pontana et al26 who documented an even 60% dose reduction using SAFIRE. We emphasize that radiologists should be familiar with the DLP metric information on the scanner console and should monitor this metric in their clinical practice.
Ability of CT to determine embolus burden, location (central or peripheral) and degree of obstruction seem to be important in predicting short-term mortality.4,27 We did not focus on these parameters in our study as these were not our primary objectives. It is also worth noting that certain information like RV function (RV/LV diameter ratio >1.0) and right heart strain (interventricular septal bowing, inferior vena cava reflux, and pulmonary artery diameter exceeding that of aorta) can be easily obtained through these CT studies that could have been added to prognostic value of CT. Computed tomography is also the method of choice for diagnosis and follow up of chronic thromboembolic pulmonary arterial hypertension (CTEPH), demonstrating intravascular web, signs of pulmonary hypertension such as dilatation of pulmonary arteries and RV, mosaic lung parenchymal attenuation, and RV hypertrophy.4 However, as we did not include known or treated patients of pulmonary embolism in our study, therefore, these entities were not discussed in our study. We also excluded pregnant patients with suspicion of PE, because of special consideration (of gestational age, in-utero exposure to contrast and radiation concerns) and possible variability in adaptation of alternative pathway that might be considered in such patients.
Computed tomography pulmonary angiogram has an overall good inter-observer agreement in diagnosis of large and central pulmonary embolism, but there may be significant discordance among radiologists particularly in evaluation of solitary, segmental, and small pulmonary embolism. Discordance of approximately 25% was noted in initial and retrospectively reviewed reports amongst the original radiologist and the chest radiologist by Hutchinson et al.28 Although we did not observe such discordance in our study, yet small defects should always be decided by consensus interpretation to avoid over-diagnosis of small pulmonary embolism. About nearly one third of subsegmental contrast filling defects interpreted by community radiologists were deemed indeterminate and approximately half of these were found to be false positive.29 All pulmonary embolism may not be treated equally like subsegmental pulmonary embolism without DVT in healthy individuals may not be clinically important versus subsegmental emboli with DVT in patients with reserved cardiopulmonary status that should be treated.30 In our study, we did not consider relevance of such diagnosed cases and their prognosis. Also, we did not consider an objective assessment criterion or scoring system for image quality in our study to have more validation of results as were documented in various other studies. Single-center, small sample size and retrospective study are few other limitations of our study.
Certain modifications in CT techniques and scanner technology may be considered in selected patients of chest pain. For exmaple, an ECG-synchronization (as seen in triple-rule-out examinations) and adjustment of contrast material timings may help exclude other causes of acute chest pain (acute aortic syndrome, acute coronary syndrome).4 Utilization of dual-energy CT may help acquire material differentiation and perfusion imaging to increase confidence level for diagnosis of PE.5 Dual-energy perfusion maps display iodine-perfused lung tissue, analogous to pulmonary scintigraphy, and allow assessment of perfusion deficits distal to vessels affected by PE. These may have value in assessing non-obstructive emboli and subsequent risk stratification.31 It would be of interest in future studies to consider utilization of dual-energy CT and acquisition of perfusion imaging and evaluating its impact on diagnosis in both acute and chronic pulmonary cases.
In conclusion, ultra-fast high-pitch dual-source CTPA with free-breathing yields better image quality and diagnosis, as well as reduced image acquisition times and radiation doses when compared to conventional standard-pitch single-source breath-hold CTPA.
Acknowledgment
We would like to thank our colleague Dr. Donya Al Hassan for providing her assistance in reviewing the submitted figures for clarity and correctness.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 30, 2018.
- Accepted January 16, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.