


Abstract
Objectives: To describe the trends in the incidence rates of 5 most common cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade.
Methods: The incidence rates of cancers (2001-2014), communicable diseases (2003-2016), and non-communicable diseases (1990-2017) were retrieved, classified, and analyzed retrospectively during November 2017, based on data available with the Ministry of Health and were analyzed at the Imam Abdulrahman Bin Faisal University in Dammam, Kingdom of Saudi Arabia.
Results: Age-standardized incidence rate (ASR) (per 100,000 population) of breast cancer among women increased dramatically from 11.8 in 2001 to 22.7 in 2014, indicating a 92.4% increase over the decade. Colorectal cancer incidence was the highest among men, and its ASR per 100,000 population increased from 5.0 to 10.6 in men and from 5.0 to 8.2 in women. Among communicable diseases, incidences of hepatitis B, measles, chickenpox, and brucellosis decreased while dengue fever increased. An alarming increase was observed in the incidence rate of non-communicable diseases namely, obesity, diabetes, and hypertension.
Conclusion: The incidence rate of non-communicable diseases increased over the decade and was associated with increased mortality and disability, reduced quality of life, and increased health-care costs, indicating an urgent need to establish prevention and control programs. The rising trend in the incidence of cancers may also become a health care issue in Saudi Arabia in the coming years.
Over the last 3 decades, Saudi Arabia has witnessed enormous progress in its socioeconomic condition that has resulted in prosperity and changes in lifestyle.1 This, in turn, has decreased the prevalence of communicable diseases and increased the prevalence of non-communicable metabolic diseases such as diabetes and obesity.2 The Saudi Arabian population is relatively young. Several factors increase the risk of metabolic and chronic diseases in the Saudi Arabian population.2 Cardiovascular ailments are at the top of the list of diseases causing highest number of mortality in Saudi Arabia.3 Among this, ischemic heart disease accounts for 14% and stroke accounts for 11% of the total casualties in 2010.3 Saudi Arabia provides free health-care services to its citizens. The government of Saudi Arabia in collaboration with the World Health Organization (WHO) has emphasized on improving the health situation in the country by focusing on 5 key health issues; namely, 1) health security and disease prevention, 2) control of communicable diseases, 3) control of non-communicable diseases, 4) accidents and injuries, and 5) strengthening of health systems, on a priority basis.1 Cases of some infectious diseases were recently identified in Saudi Arabia, indicating that despite technological developments in diagnostics, treatment, and vaccination programs, various infectious diseases have re-emerged in Saudi Arabia after a decade.4 For instance, the prevalence of Middle East respiratory syndrome coronavirus infection increased in Saudi Arabia during 2012, and this disease continues to be a concern during the summer season and religious congregations in holy sites.5 Cancers are a major health concern globally. In Saudi Arabia, the incidence of the most common cancers has increased steadily, with colorectal cancer being the most common cancer among men and breast cancer being the most common cancer among women.6-8 The scientific information available on the current status and trends of various communicable, non-communicable diseases and cancers are limited to the primary statistics available in the portals of Ministry of Health and other health agencies. However, studies on these publicly available data regarding its analysis to derive a conclusion regarding the trends of major disease in Saudi Arabia is scanty and scattered if existed. Hence, the present study was aimed at analyzing the trends in the incidence of 5 most common cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade.
Methods
Five most common diseases in cancer from cancer registry (2001 to 2014), communicable diseases from Ministry of Health Statistics Year Book (2003 to 2016) and non-communicable diseases from studies published in PubMed (1999 to 2017) were included in the present study. As the existing data from the database/registry were taken, no informed consent and institutional review board (IRB) approval were required for this study.
Data on the incidence of breast cancer, colorectal cancer, thyroid cancer, non-Hodgkin’s lymphoma (NHL), and leukemia according to gender for the period 2001–2014 were extracted from the Saudi Cancer Registry during November, 2017 at Imam Abdulrahman Bin Faisal University in Dammam, Saudi Arabia.9 These data were segregated based on cancer type and gender, and age-standardized incidence rate (ASR) per 100,000 population was plotted according to gender for the period between 2001–2014.
Data on 5 common communicable diseases, namely, hepatitis B, dengue fever, measles, chickenpox, and brucellosis, were obtained from the Ministry of Health statistics year book for the period between 2003–2016 and was accessed during November, 2017.10 Trends in the incidence rate per 100,000 population of these communicable diseases were plotted for the same period. Data on 5 common non-communicable diseases, namely, obesity, diabetes, hypertension (HTN), coronary artery diseases (CAD), and pulmonary disease, were retrieved from studies (PubMed) published over the last decade, reviewed, and expressed as prevalence percentage. For literature search, we used PubMed and Google Scholar databases with keywords specific to selected cancers, communicable and non-communicable diseases.
Results
The incidence rates of the 5 common cancers, communicable diseases, and non-communicable diseases have been summarized (Tables 1, 2, & 3), and the trends in the incidence of these diseases have been illustrated (Figures 1, 2 & 3).
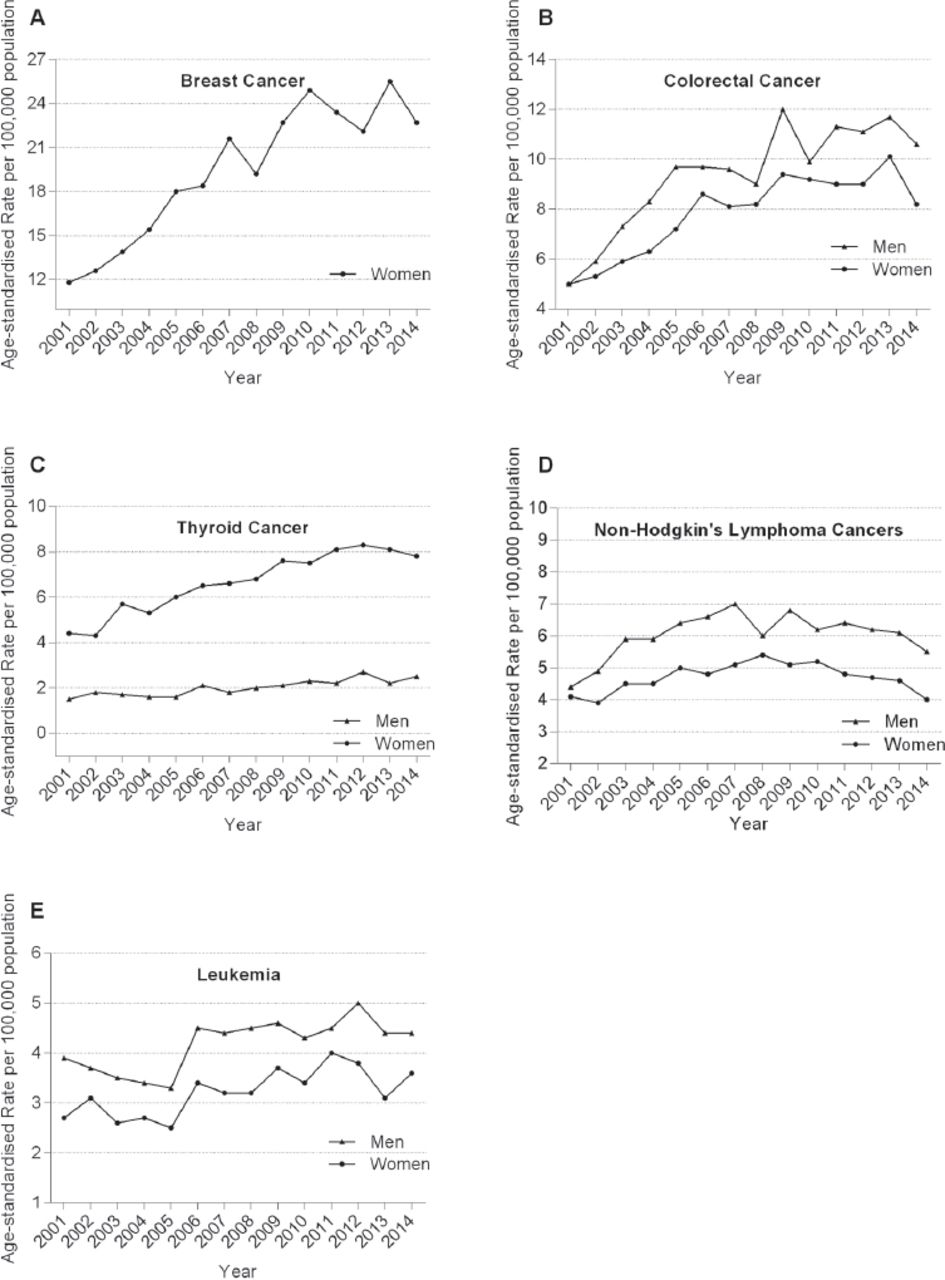
Age standardised incidence rate (ASR) per 100,000 of various cancers among male and female population of Saudi Arabia.
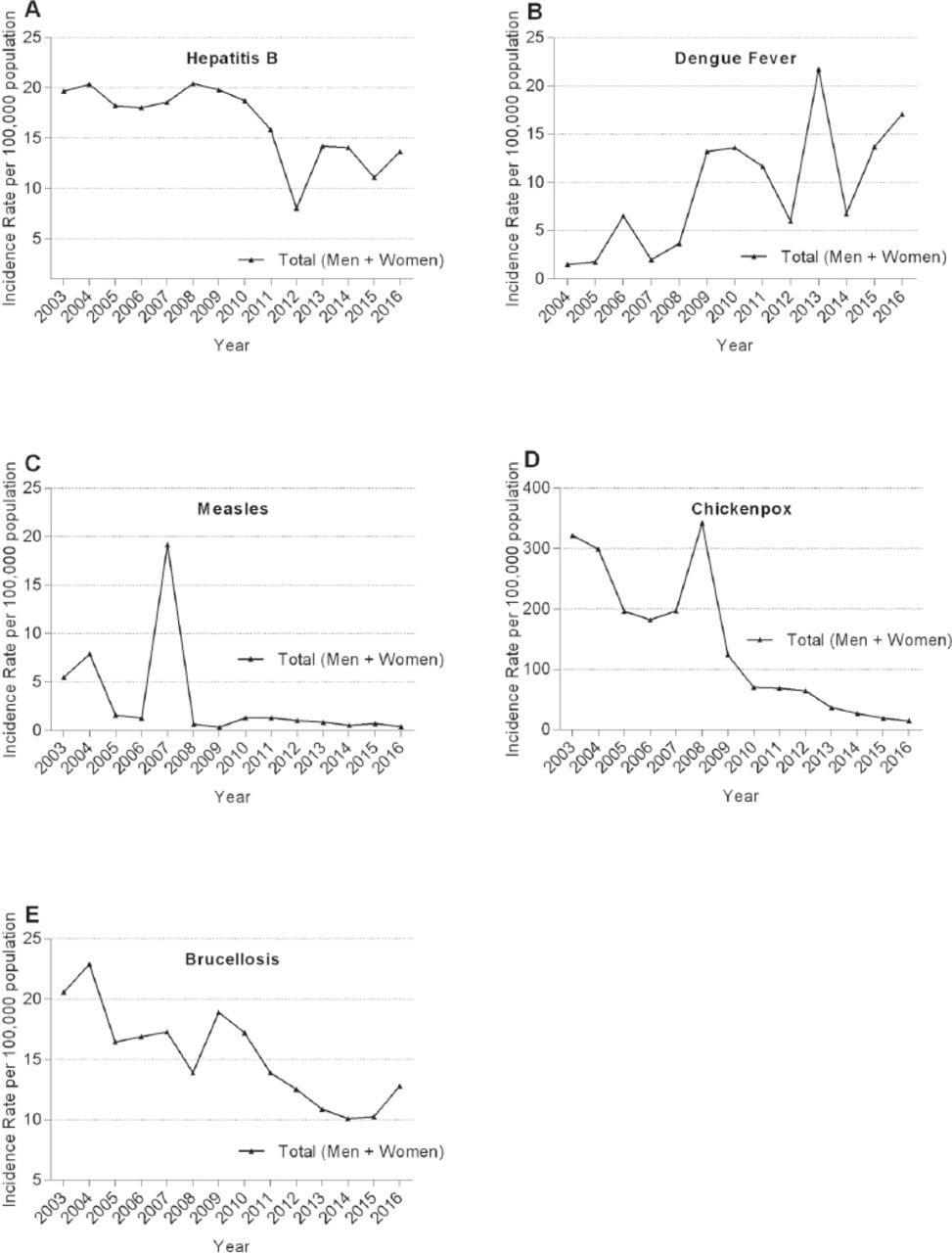
Incidence rate (per 100,000) of various communicable diseases among general population in Saudi Arabia
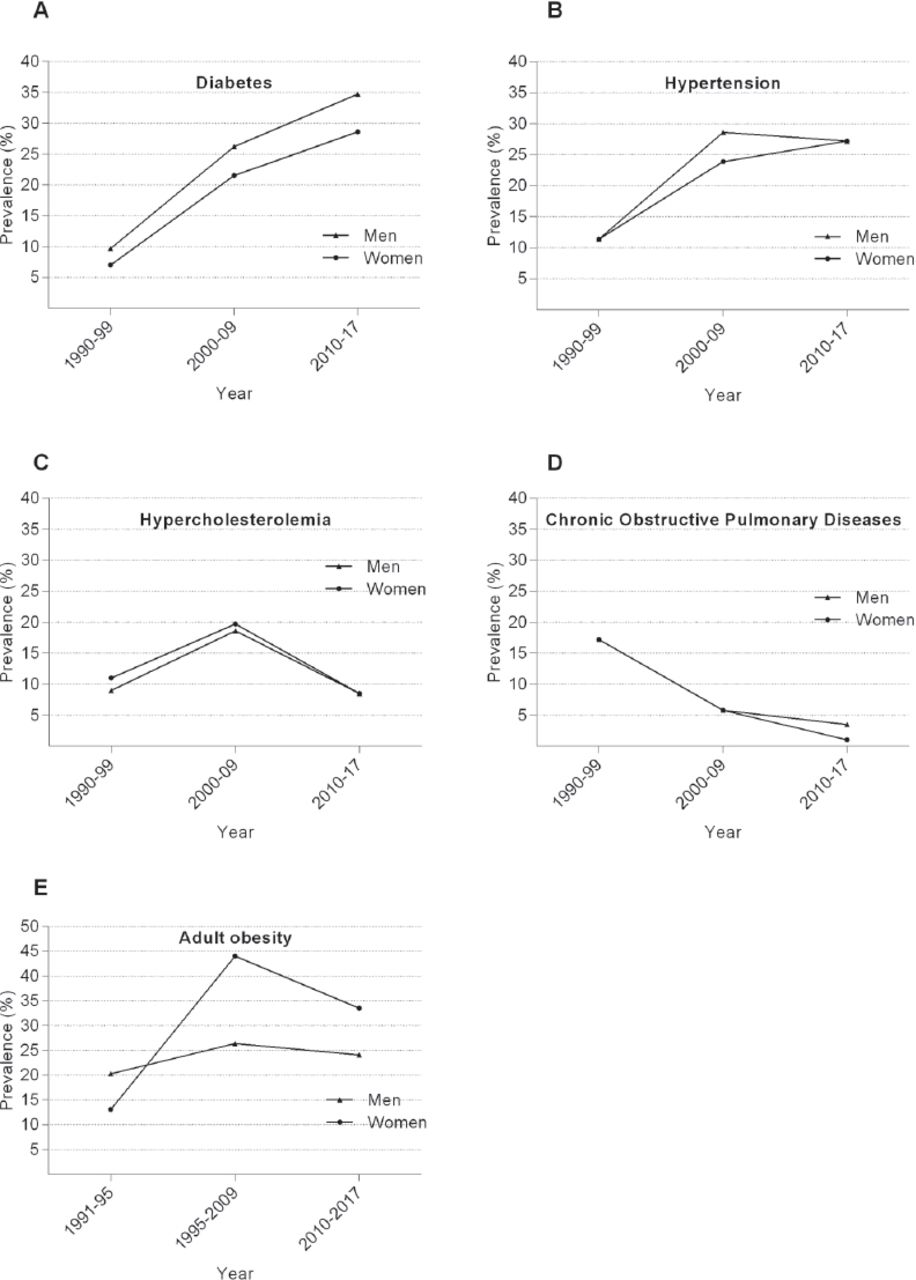
Prevalence (%) of various non-communicable diseases among male and female general population of Saudi Arabia.

The age-standardized incidence rate (ASR) per 100,000 population of breast cancer (A), colorectal cancer (B), thyroid cancer (C), Non-Hodgkin’s lymphoma (D), and leukemia (E). The graphs have been plotted using data obtained for Saudi Arabian men and women for the period 2001-2014.

The incidence rate per 100,000 population of communicable diseases, including hepatitis B (A), dengue fever (B), measles (C), chickenpox (D), and brucellosis (E).
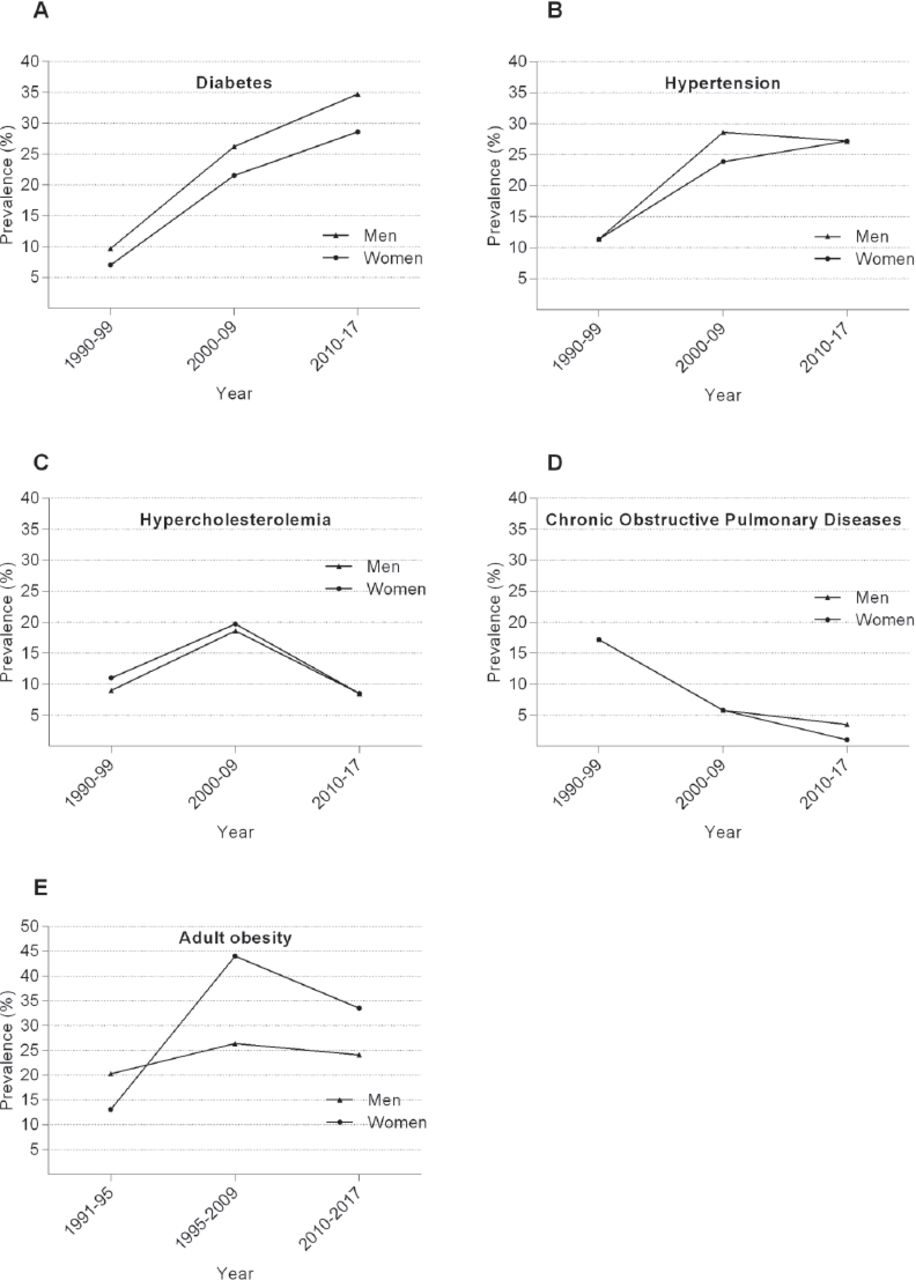
The prevalence (%) of non-communicable diseases such as diabetes (A), hypertension (B), hypercholesterolemia (C), chronic obstructive pulmonary disease (D), and obesity (E) is shown over a decade.
Incidence of cancers
Table 1 and Figure 1 show the incidence rates and trends in the ASR of breast cancer, colorectal cancer, thyroid cancer, NHL, and leukemia from 2001 to 2014. The ASR of breast cancer among women per 100,000 population increased dramatically from 11.8 in 2001 to 22.7 in 2014, indicating a 92.4% increase in incidence over the decade. The ASR of colorectal cancer (per 100,000 population) increased from 5.0 to 10.6 in men and from 5.0 to 8.2 in women during the same period. The ASR of thyroid cancer (per 100,000 population) increased from 1.5 to 2.5 in men and from 4.4 to 7.8 in women during the same period. The ASR of NHL (per 100,000 population) noticeably increased from 4.4 to 5.5 in men and stabilized at the same rate, with only a marginal decrease (4.1-4.0), in women. The ASR of leukemia (per 100,000 population) increased from 3.9 to 4.4 in men and from 2.7 to 3.6 in women.
Incidence of communicable diseases
The incidence rates (per 100,000 population) and trends in the ASR of hepatitis B, dengue fever, measles, chickenpox, and brucellosis for the period 2003-2016 are shown in Table 2 and Figure 2. The incidence rate of hepatitis B per 100,000 population decreased from 19.65 in 2003 to 13.63 in 2016, indicating a 30.6% decrease in incidence. In contrast, the incidence rate of dengue fever per 100,000 population remarkably increased from 1.52 in 2004 to 17.10 in 2016. The incidence rate of measles per 100,000 population decreased from 5.48 in 2003 to 0.39 in 2016. Similarly, the incidence rate of chickenpox per 100,000 population drastically decreased from 321.75 in 2003 to 14.25 in 2016. Moreover, the incidence rate of brucellosis per 100,000 population decreased from 20.58 in 2001 to 12.80 in 2016, indicating a 37.8% decrease in incidence.
Incidence of non-communicable diseases
The prevalence of diabetes increased from 9.7% in 1970-1979 to 26.2% in 2000-2009 among men and from 7% in 1970-1979 to 21.5% in 2000-2009 among women (Table 3 and Figure 3A). The prevalence of diabetes further increased to 34.7% among men and 28.6% among women in 2010-2017.11-15 The prevalence of HTN also increased from 11.4% to 28.6% in men and from 11.4% to 23.9% in women from 1970-1979 to 2000-2009 (Table 3 and Figure 3B).13,16,17 The prevalence of hypercholesterolemia (elevated serum cholesterol level) increased from 9% to 18.6% in men and from 11% to 19.7% in women during the same period (Table 3 and Figure 3C).11,18 However, the prevalence of chronic pulmonary diseases such as bronchitis and emphysema decreased from 17.2% among both men and women in 1990-1999 to 5.8% in 2000-2009 and further decreased to 3.5% among men and 1.0% among women in 2010-2017 (Table 3 and Figure 3D).19-24 The prevalence of CAD was 6.6% in men and 4.4% in women.19 The prevalence of obesity was increased from 22% in 1990-1993 to 36% in 2005 (Figure 3E).20 The prevalence of obesity was 24.1% in males and 14% in females.21 In Buraydah and Unaiza, the male obesity was found to be 34.3% and female obesity was 17.3%.22 In Tabuk, male obesity was 18.1%.23 The prevalence of obesity among Saudi children was found to be 9.3%.24 In Jeddah, moderately obese was 10.7% and severely obese was 7.9%.25 In Aseer, the prevalence of obesity was 23.2%.26
Discussion
Saudi Arabia, with a population of 31.5 million people (in 2015), spends 7.25% of its annual budget on health services and has witnessed an increase in life expectancy from 69.0 years (1990-1999) to 74.3 years (2015), decrease in crude birth rate from 47 per 1000 population (1990-1999) to 21 per 1000 population (2015), and increase in GDP per capita income of USD 20,723.10 The present study assessed the trends in the incidence rate of 5 most common cancers, communicable diseases, and non-communicable diseases in Saudi Arabia.
Our data showed that breast cancer was the most common cancer among Saudi Arabian women. This finding highlights the very low rate of breast cancer screening and the need to intensify breast cancer screening in Saudi Arabia. In the United States (US), literate women are more likely to undergo a mammography.27 However, the rate of mammography is only 6.7% in Saudi Arabia compared with 72.4% in the US.8,28 Therefore, women empowerment is imperative for achieving the national goals of health education. Knowledge about breast cancer and its screening is still very poor among Saudi women. Therefore, awareness programs regarding the importance of breast cancer screening should be initiated more aggressively among Saudi Arabian women. The median age for colorectal cancer was 60 years for men and 55 years for women during 1994-2000 in Saudi Arabia and was 68 years for men and 72 years for women during 2004-2010 in the US.7,29 Therfore, it is recommended to begin screening of colorectal cancer in Saudi Arabia at the age of 40 years and it may be strictly implemented.28 The incidences of cancer in Saudi Arabia have reached a plateau recently, at least for colorectal cancer and the data supports this for the years 2010-2014. The increase in the number of reported cases of colorectal cancer in the last 5 years is merely due to an increase in the size of the population, but not an increase in the incidence rate which has fluctuated between 9-10/100,0000 and this is different from the rate in the 1990’s.
Thyroid cancer is the third most common cancer among Saudi Arabian women. Increased incidence of thyroid cancer over the last decade may be attributed to its increased detection and diagnosis.30 The mean age at diagnosis for thyroid cancer is 50 years in men and 42 years in women, which is significantly low.31 The incidence of thyroid cancer is almost equal among individuals in the third, fourth, and fifth decades of life; however, this incidence differs according to gender, with most cases occurring in the third decade of life (20-30 years) in women and in the fifth decade of life (40-50 years) in men.30 The increase in the incidence rate of overall cancer could be due to availability of better diagnostic tools now in Saudi Arabia compared to the early 1990’s. Moreover, there is more robust registration of cancer cases compared to the past when the registry was launched and the experience was small in this vital field. Finally, Saudis live longer now, which explains the rise in cancer cases and chronic illnesses like diabetes, hypertension and hyperlipidemia. As the population ages and the infertility rate drops with more women joining the work force and with increased financial burden of the large families and higher education of the married couple; the younger age groups will make a less portion of the society. This will have an impact on the overall incidence rates of cancer and non-communicable diseases.
Prevention and management of emerging, re-emerging, and stable infectious diseases is a continuous process. These diseases can be successfully monitored and controlled by adopting effective supervision, research, and drug development strategies and by introducing counter measures such as surveillance, diagnosis, and effective affordable drugs and vaccines. Saudi Arabia has witnessed a steady decrease in the incidence of hepatitis B, measles, chickenpox, and brucellosis. In 1989-1990, Saudi Arabia introduced a highly effective hepatitis B vaccination program in schools, through which all Saudi Arabian individuals aged ≤34 years (as of 2017) were vaccinated at birth or at school. This has steadily decreased the incidence of hepatitis B in Saudi Arabia. Except for an unknown increase in the incidence of measles, a vaccine-preventable infectious disease, in 2007, there has been a decrease in the incidence of other communicable diseases in Saudi Arabia.
Although the incidence of chickenpox was high before 2008, introduction of a varicella zoster vaccination program in 2008 drastically decreased the incidence of this viral infection to a minimal level, indicating a successful control of this virus in Saudi Arabia. The incidence of brucellosis has significantly decreased over the last decade; however, its incidence is noticeably high in Saudi Arabia compared with that in developed countries. Therefore, it is important to implement effective nationwide measures for controlling brucellosis. In contrast to the decreased incidence of major preventable infectious diseases, the incidence of dengue fever, a mosquito-borne viral disease, has increased in Saudi Arabia. Saudi Arabian tourists travelling to tropical destinations and infected immigrants from dengue fever endemic regions may have increased the dissemination of this contagious infection. Moreover, unavailability of effective vaccines against dengue fever hinders the nationwide measures for controlling this infection.
Non-communicable diseases such as diabetes (including types 1 and 2 diabetes) and obesity are a major challenging health issue in Saudi Arabia (Figure 3). Over the last decade, the incidence of diabetes has dramatically increased and was 34.7% among men and 28.6% among women during 2010-2017, indicating that one in every 3 individuals in Saudi Arabia is diabetic. Moreover, Saudi Arabia has one of the highest incidence rates of adult obesity worldwide. Data obtained from a previous study predicts an alarming increase in the incidence rate of obesity (men: 41.40%; women: 77.6%; overall: 59.5%) by 2022.20 If left unchecked because of the absence of appropriate health education and policies, the incidence of diabetes and obesity in Saudi Arabia could increase to epidemic proportions, which may further lead to health issues such as micro- and macrovascular diabetes-associated complications, including cardiovascular diseases. The rapid increase in the prevalence of diabetes and obesity among the Saudi Arabian population may be attributed to distinct factors such as sedentary lifestyle with physical inactivity, irregular feeding habits, and intake of high-calorie foods and beverages.30,32 Therefore, a shift in attitude toward regular exercise, proper food habits, and physical activity in addition to appropriate health education from educational institutions, governmental and non-governmental organizations, and corporates may be beneficial in ensuring better health of the Saudi Arabian population in the long run.
The prevalence of chronic non-communicable diseases has increased in most countries, including Saudi Arabia, and is likely to increase further. Increased life expectancy and aging population increase the risk of chronic diseases. Although medical technology is enabling many people to cope with chronic diseases, its effects on the lives of elderly people are relevant when considered in terms of loss of life, disability, family hardship, poverty, and economic loss to the country. Therefore, increased emphasis should be given to the control and prevention of chronic diseases among the elderly population. However, lifestyle and behavioral patterns of the young generation are also changing rapidly, leading to the early onset of chronic diseases among the youth.
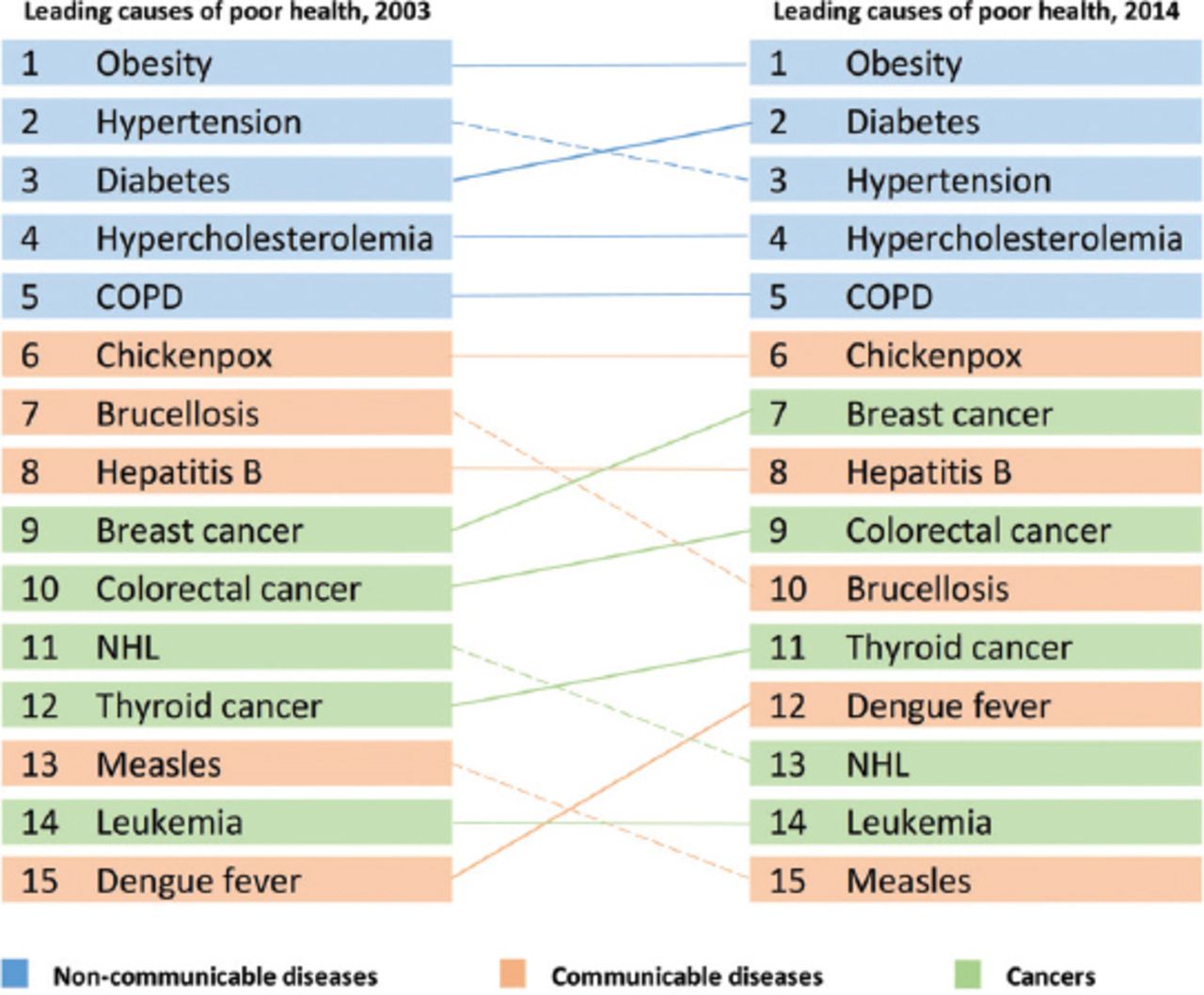
Non-communicable diseases present a considerable challenge both in human and economic terms, with many countries introducing policies to improve their health infrastructures. The critical challenge for Saudi Arabia is to enhance its capacity for monitoring, preventing, and controlling non-communicable disease while maintaining and advancing the landmarks established in controlling communicable diseases (Figure 4). Organizations such as the World Health Organization (WHO) and stakeholder nations should continue their efforts toward the global prevention and control of non-communicable diseases. Such programs could reduce morbidity and mortality associated with these diseases and could improve the quality of life and economic condition of the affected individuals.33 The key components of such programs are to promote awareness regarding the burden of non-communicable diseases, improve surveillance, train public health professionals, and increase healthcare capacity building at the national level by establishing feasible goals to prevent these diseases. This also includes the establishment of national health promotion programs and effective non-communicable disease prevention and control policies and programs.
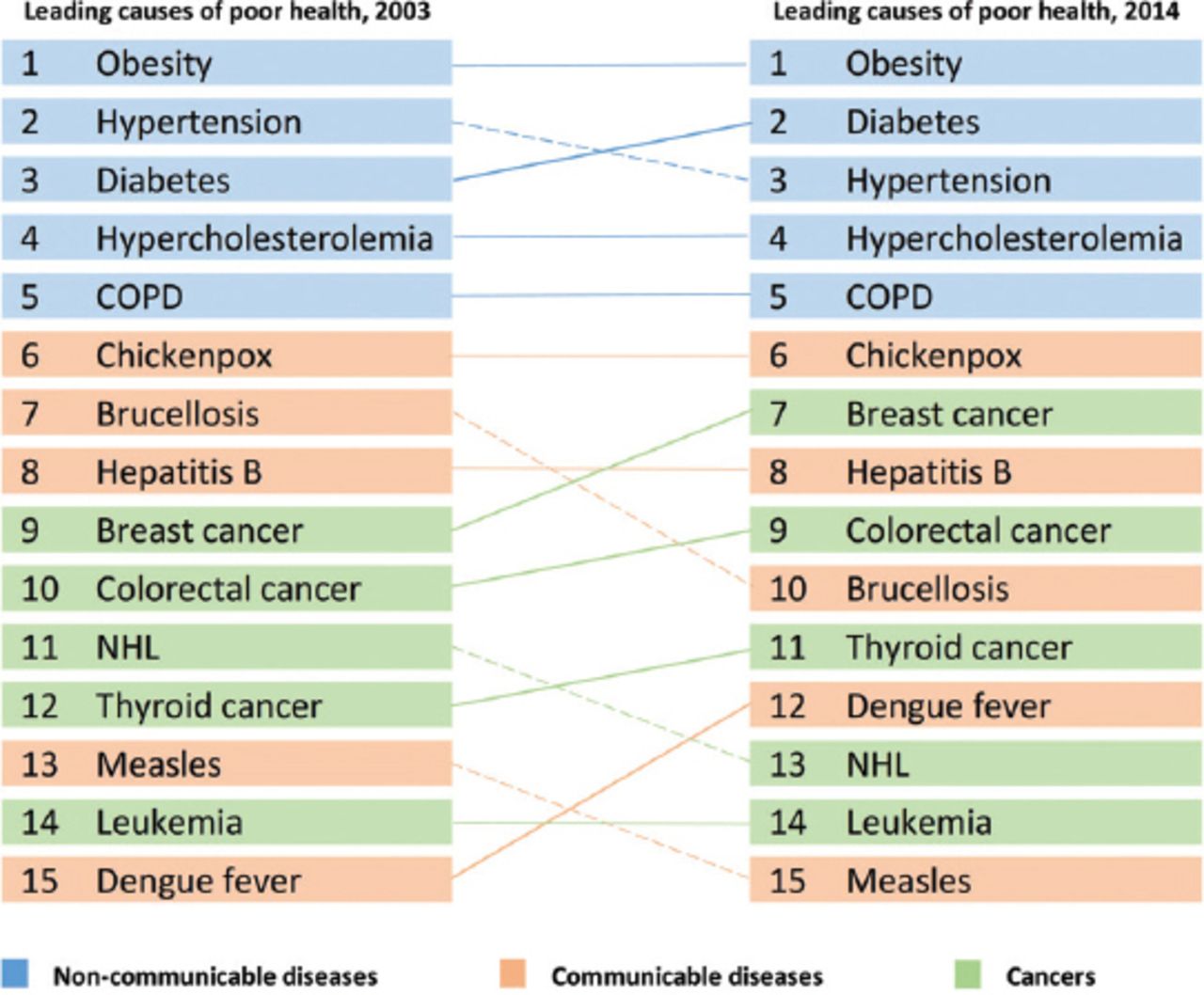
Leading causes of poor health in Saudi Arabia in 2003 are compared with those in recent years (2014). Dotted downward lines indicate descending trend, solid bold upward lines indicate ascending trend, and thin solid horizontal line indicates maintenance of the ranking among these causes. COPD - chronic obstructive pulmonary disease, NHL - non-Hodgkin’s lymphoma.
Though non-communicable diseases present a major challenge in the present scenario, the limitation of this study is prevalence studies on non-communicable diseseas are very limited and vary in methodologies including population size and disease definition. Nevertheless, the findings of the study has several future implications such as; addressing the problems of increasing cancer cases; early screening of common cancers and planning of national health awareness schemes and vaccination programs. Additionally, the need for establishment of health promotion programs to combat noncommunicable diseases, developing preventive measures and increasing public health awareness becomes today’s need in ensuring good community health.
In conclusion, the national data for Saudi Arabia indicates its considerable success in preventing communicable diseases through national health awareness programs and effective vaccination programs. However, an unprecedented increase in the prevalence of diabetes and obesity over the last decade is a major public health concern that requires the urgent establishment of health programs.
Acknowledgment
We would like to thank Scribendi Inc., Chatham ON, Canada for English language proofreading and editing. Assistance received from Dr. Sadananda Acharya in preparation and formatting of graphs and figures is greatly acknowledged.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 15, 2018.
- Accepted January 23, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}