


Abstract
Objectives: To investigate the intercourse between the platelet/lymphocyte (P/L) and neutrophil/lymphocyte ratio (N/L), and vitamin D (Vit-D) levels in low bone mineral density (BMD) of women.
Methods: Two hundred fifty-two postmenopausal female outpatients who were admitted to the obstetrics and gynecology and physical therapy clinics between July 2016 and December 2017 were retrospectively analyzed. The patients were grouped in relation to their T-score (normal [n=92], osteopenia [n=112], and PMO [n=48]). The serum levels of P/L, N/L, Vit-D, BMD and complete blood count of the patients were retrospectively examined.
Results: The median P/L was significantly higher and Vit-D levels were significantly lower in the PMO group (130.75 [52.89-385] versus 123.05 [54-232.5], p=0.02 and 15.4 [4-34] versus 20.1 [4-47], p=0.003). While BMD and P/L were negatively correlated, a positive correlation between BMD and Vit-D was found. Vitamin D levels were negatively correlated with P/L (p<0.001) and N/L (p=0.04). Older age (≥65 years), Vit-D deficiency and P/L values >125.06 were found as independent prognostic factors for PMO in regression analysis.
Conclusion: Higher P/L seems to be a quite simple marker to help predict postmenopausal PMO. As seen in our study, having low levels of Vit-D is crucial for PMO.
Postmenaposal osteoporosis is a frequent disease among postmenopausal women. Bone loss and decreasing of bone mineralization is an important cornerstone in the pathology. In postmenopausal osteoporosis, there is a diminish in total bone mass, especially in the trabecular part of the bone, predisposing to pathologic fractures as a result of increased bone fragility. Fractures associated with PMO are one of the most leading causes of disability; limitation of activity; shortening of height, hunching, and difficulty in breathing; deterioration in quality of life; increased mortality; and leads to substantial medical care costs worldwide. Moreover, in many regions of the world, the incidence hip fractures has increased every year by 1-3%.1 Risk factors for PMO includes low bone mass, advanced age, family history of fractures, smoking, physical inactivity, Vit-D and calcium deficiency, malnutrition, and long-term use of steroids.2,3 Among these, Vit-D deficiency in particular as a predisposing factor to PMO, has become increasingly important in recent years. Vitamin D is essential for the body it is mandatory for bone health and metabolism, and its deficiency is quite common in society.4 Studies describing the relationship between Vit-D levels and inflammatory cytokines have indicated that, the levels of C-reactive protein (CRP) and Interleukin 6 (IL6) might be correctable following supplementation therapy.5-7
Inflammatory markers play a modulating role through osteoclast activation by surrounding cytokines in bone formation and destruction.6,7 In epidemiologic studies, PMO has been found more commonly in inflammatory diseases such as systemic lupus erythematosus (SLE), ankylosing spondylitis, ulcerative colitis, Crohn’s disease, and rheumatoid arthritis, which has drawn attention to the association between PMO and chronic inflammation.8-10 There are some reports showing that the levels of CRP, IL6, and tumor necrosis factor-alfa (TNF-α) increase in PMO.11,12 In contrast, Berlunglundh et al,13 showed that CRP was not seen as a marker of osteoporosis in older women, they found that the highest CRP level might be associated with PMO-related mortality. The interaction of some factors in platelets with Vit-D receptors is important for bone turnover. Therefore, it is estimated that platelets may contribute to PMO.14 Another theory is that platelets can contribute to inflammation by releasing thromboxane.15,16 The ratios of P/L and N/L are simple, easily accessible and inexpensive inflammation parameters. They have been shown to be associated with various inflammatory and cardiovascular diseases, and cancer. Furthermore, these parameters are now being evaluated as prognostic indicators for pre-treatment in some inflammatory diseases and cancer.17-19 However, the relationship between N/L, P/L, and PMO has not yet been fully elucidated.
In the literature, the relationship between N/L, P/L, and PMO has been investigated in several studies.20-23 In this article we have examined the association between N/L, P/L, Vit-D level, and low BMD.
Methods
All postmenopausal females, 252 outpatients who were admitted to the obstetrics and gynecology and physical therapy clinics between July 2016 and December 2017 were retrospectively analyzed. While the patients who were known to have been menopausal for at least one year were including, on the other hand, the patients who have <1 year history of menopause, acute or chronic infection, anemia, thrombocytopenia and leucopenia, history of oncologic or hematologic diseases, liver or kidney disease, rheumatologic disease, any trauma history requiring hospitalization in the last 6 months, history of blood transfusion in the last one year and steroid use were excluded in the study. Demographic characteristics along with the laboratory findings including BMD, complete blood count measurements (the value of hemoglobin [Hb], mean platelet volume [MPV], neutrophil, monocytes, lymphocyte and platelet), and Vit-D levels were carefully recorded. Neutrophil/lymphocyte ratio, monocyte-lymphocyte ratio (M/L), and P/L were calculated through the formulas as shown; N/L level, M/L level, and P/L level. Bone mineral density measurements were evaluated using dual energy x-ray absorptiometry (DEXA). Bone mineral density (g/cm2) values and T scores of total lumbar (L1-L4) spine, femur neck and femur total values obtained by DEXA were recorded. In accordance with the World Health Organization (WHO) endorsement, its PMO was accepted as bone density showing a T-score -2.5. Osteopenia was defined as T-scores between -1.0 and -2.5. Normal BMD was defined as T-scores -1.0. Based on these definitions, 3 groups of patients were defined according to BMD as normal, osteopenia, and PMO.24 The patients’ demographic characteristics, body mass index (BMI) and age were recorded. Body mass index was defined by calculating; weight/(height*height) (kg/m2).
Patients were included in the osteopenia group if the lumbar total, femur total or femur neck values were -1, and in the PMO group if it was <-2.5. Google Academic and PubMed were used to review similar previous studies. The Ethical approval of the study was obtained from the local institutional ethical committee (Date: 25.01.2017, Decision: 1/28), and it was conducted in consideration of the Helsinki Declaration.
Statistical analysis
All data were analyzed by using the Statistical Package for Social Science (SPSS) Version 22.0 (IBM Corp., Armonk, NY, USA). In normally distributed data, Student’s t-test and Analysis of Variance were used for comparison (age and BMI), and the Mann-Whitney U and Kruskal-Wallis tests were used to compare non-normally distributed data (Hb, P/L, N/L, M/L, Vit-D, and MPV). The Pearson and Spearman tests were used for correlation analysis between age, BMI, P/L, N/L, and M/L. Receiver operating characteristics (ROC) curve analysis was used to establish the cut-off value of P/L levels. Multivariate logistic regression analysis was performed in order to find the strongest predictors of the outcome variable in PMO. A p-value<0.05 was considered significant.
Results
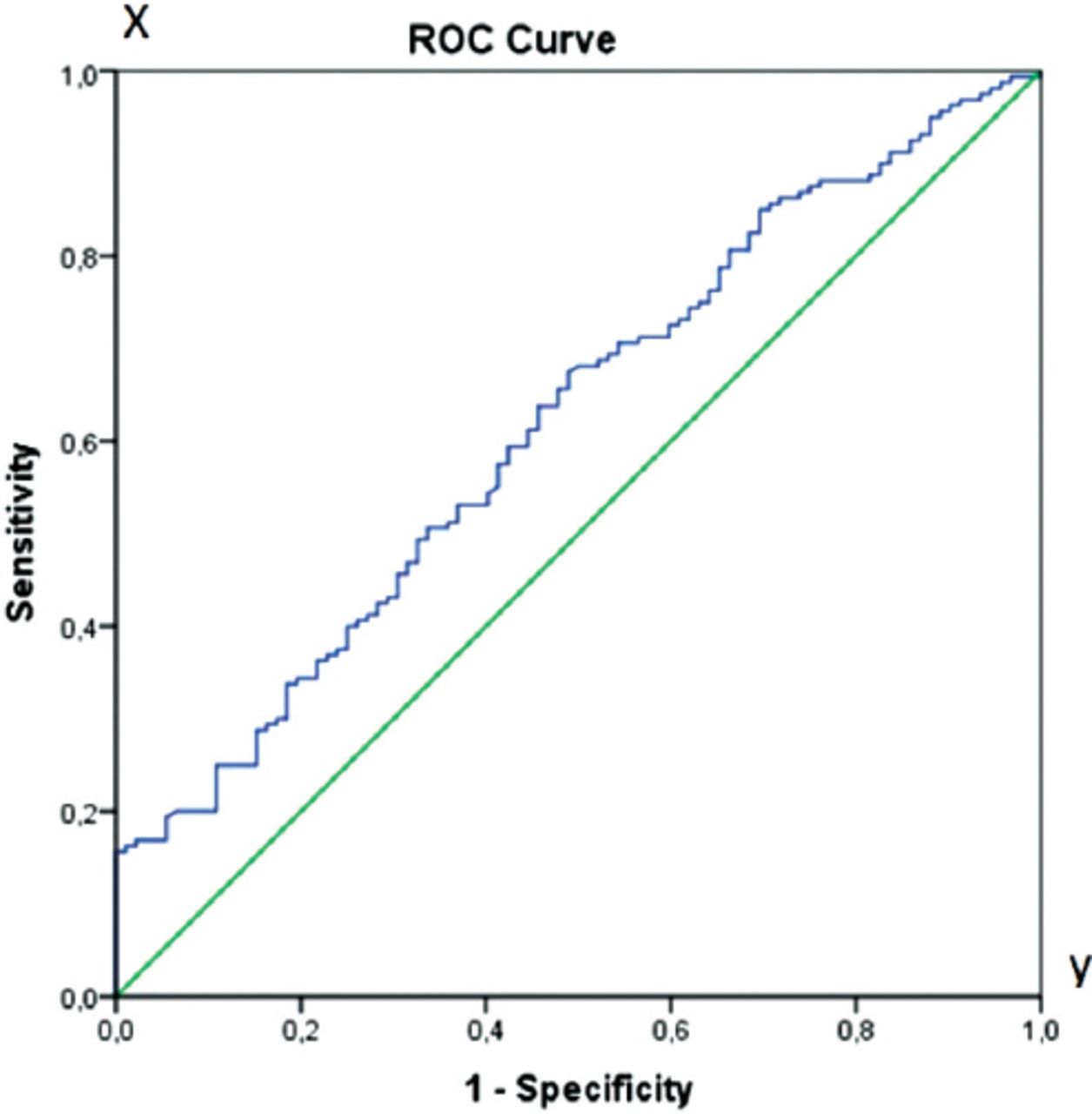
In all groups, the mean age was 54.12±7.34 years and BMI was 29.84±4.97 kg/m2. First, the patients were divided according to their BMD values (without distinguishing them according to the lumbar total or femur total values) as normal and low BMD. Only the P/L value was significantly higher in the low BMD patients (p=0.02). The P/L was significantly different between the groups (p=0.02); however, there was no remarkable difference when the other values were examined (p>0.05). Table 1 shows P/L, N/L, M/L, and MPV values, according to the patients’ BMD values. The patients’ BMD values were also divided; lumbar total, femur total, and femur neck. There was a meaningful difference in P/L values when patients were grouped according to their lumbar total value (p=0.028), femur neck (p=0.013), and femur total values (p=0.015) (Tables 1-3). Vitamin D levels were being fairly higher in the normal BMD group according to the other groups (p<0.001), (Vit-D normal range 20-100 ng/mL). The correlation analysis showed a reverse relationship between P/L, N/L and Vit-D levels (Table 4). There was also an inverse association between BMI, P/L (p=0.005) and M/L levels (p=0.01) in the correlation analysis. Age was found to be positively correlated with BMI (p=0.005) and reversely correlated with the lumbar (p=0.001), femur neck (p=0.01) and femur total BMD (p=0.01). There was an inverse correlation between P/L and lumbar total (p=0.01), femur neck (p=0.04), and femur total (p=0.02) BMD (Table 4). Receiver operating characteristics analysis was used to identify the significance of the P/L value. The ROC curve area was found to be 0.62, which was considered as significant for low BMD (osteopenia and PMO). Considering the ROC analysis, the cut-off P/L value for low BMD was found as 125.6 (Figure 1).
The levels of hemoglobin, Vitamin D, mean platelet volume, body mass index, ratios of platelet/lymphocyte, neutrophil/lymphocyte and monocyte/lymphocyte according to bone mineral densitometry.
The levels of hemoglobin, Vitamin D, mean platelet volume, body mass index, ratios of platelet/lymphocyte, neutrophil/lymphocyte and monocyte/lymphocyte according to lumbar bone mineral density.
The levels of hemoglobin, Vitamin D, mean platelet volume, body mass index, ratios of platelet/lymphocyte, neutrophil/lymphocyte and monocyte/lymphocyte according to femur neck and femur total BMD.
The correlation between lumbar-femur neck-femur total BMD values and Hb, Vitamin D, MPV, BMI, ratios of platelet/lymphocyte, neutrophil/lymphocyte and monocyte/lymphocyte.
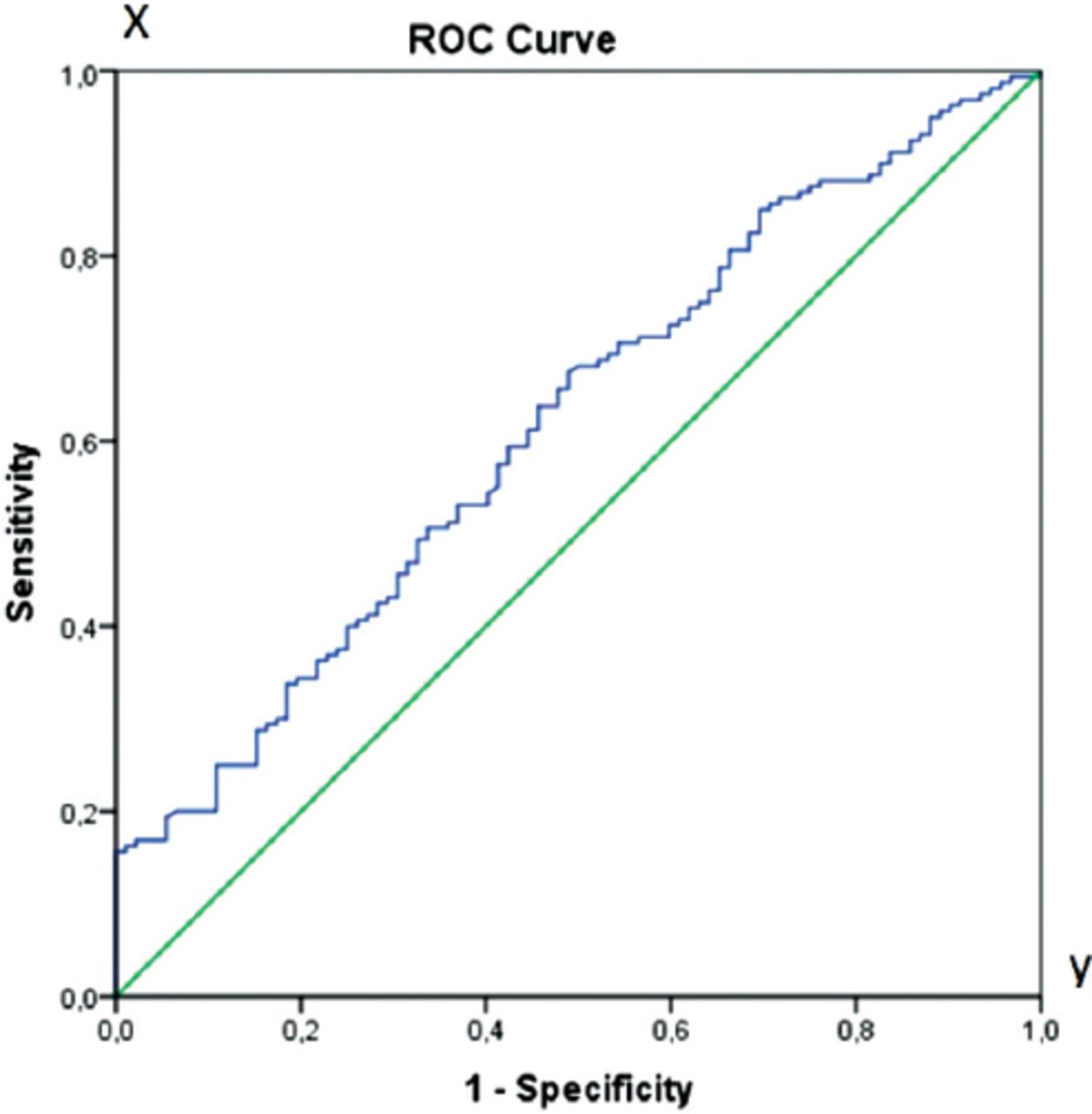
Receiver operating characteristic (ROC) analysis for platelet/lymphocyte (P/L) level. (x) sensivity, (y) spescificity.
In the logistic regression analysis, P/L >125.06, age >65 years, and Vit-D deficiency were identified as independent predictors of low BMD (Table 5).
Risk factors for osteoporosis and P/L in logistic regression analysis.
Discussion
In this study, the P/L was importantly elevated in the osteopenia and PMO groups compared with the normal BMD group. According to the correlation analysis, there was a negative correlation between P/L and bone densitometry. Based upon the findings of this study, it can be concluded that P/L may be used as an osteopenia and PMO marker in postmenopausal patients. In addition, low BMD group was associated with low Vit-D levels. It was observed that high P/L and low Vit-D were independent risk factors for low BMD. Bones are dynamic organs where construction and destruction always continues. Inflammation is necessary for this transformation. However, this cycle is disrupted in chronic inflammation in favor of osteoclastic activity, resulting in osteopenia, PMO and even fractures. Several studies have investigated the association between inflammation and PMO. C-reactive protein is secreted from the liver and its level increases through the stimulation of TNF-α, IL6, and IL1. Many studies have showed a positive association between elevated serum CRP levels and PMO.13,25 In meta-analysis involving 34,840 patients, most studies have shown that high-sensitivity CRP (hs-CRP) elevation and fracture risk are correlated, but the remaining few studies have not supported this result.26 In contrast, Oei et al,27 investigated the data of 6338 patients, and serum levels of CRP were slightly increased (as not statistically significant) in fracture formation; so there is no proof of this relationship. Besides this, the authors claimed that the strongest effect in osteoporotic fracture was the lowest level in femur neck BMD. In this study, it was observed that the relationship between hs-CRP and femur neck BMD was weak.27 The high incidence of PMO accompanying many inflammatory diseases in the literature reveals the relationship between chronic inflammation and PMO. The association of PMO with Crohn’s disease, ulcerative colitis, rheumatoid arthritis, and SLE has been demonstrated in previous studies.10 Al-Daghriet al,28 showed that IL6 was a predictor of bone loss in the postmenopausal period, indicating that increased biologic age along with early postmenopausal status (within 10 years after menopause) were significantly and independently associated with high serum IL6 levels. By contrast, in a recent study of 2915 patients, Sponholtz et al,11 found no association of IL6 and TNF with hip and spine BMD in postmenopausal patients receiving hormone replacement therapy (HRT). In postmenopausal patients who did not receive HRT, there was no relationship between CRP level and BMD; however, there was an association between CRP level and femoral neck in postmenopausal patients receiving HRT.11 Although there are an increasing number of studies investigating the relation between PMO and inflammatory markers, the number of studies examining the association of N/L and P/L with BMD has remained insufficient. In this study, we found high P/L levels in the osteopenia and PMO groups; however, there was no significant relationship with N/L. Contrary to our study, Huang et al,29 showed a positive correlation between N/L and PMO. Yu et al,20 suggested that N/L was associated with arterial stiffness in patients with PMO. Fisher et al,21 stated that high N/L displayed as a potential indicator of bone fracture. Although Yılmaz et al,22 showed that N/L and CRP were significantly higher in the osteoporotic group than in the control group, N/L was found to be more effective for predicting PMO than CRP. There is only one study exploring the association of P/L and PMO along with N/L.23 Similar to our study, the relationship of P/L-BMD, but not N/L-BMD and Vit-D-P/L-N/L, was found to be similar in Koseoglu’s study in which postmenopausal patients were divided into 2 groups as normal and low BMD, and an inverse relationship was found between P/L and BMD, without any statistically significant relation between N/L and BMD.23 In addition, different from our study, low density lipid (LDL) was seen but it was no related with BMD.23
When the association of Vit-D with N/L, P/L, and PMO was examined, Vit-D levels were significantly less in the low BMD group and BMD values and Vit-D levels were found to be correlated. In a study in Chinese, BMD and serum 25-(OH) D levels were found to be correlated.30 As in our study, there are a number of studies demonstrating the association of PMO with Vit-D deficiency.31 Similar to our study, the relationship between Vit-D and P/L-N/L was found to be inversely correlated in Akbas et al’s study.32 In another study, it was observed that Vit-D supplementation was associated with a decrease in N/L.33 Some studies have shown that inflammatory markers are elevated in PMO. In this study, we found that P/L and N/L, which are simple serum markers, can be used easily in predicting PMO with low Vit-D.
Study limitations
Major limitations in our study are its small sample size and the fact that we could not assess the dietary intake of calcium and Vit-D.
In conclusion, the association of Vit-D with N/L and P/L supports the relationship between Vit-D and inflammation. Although there is no relationship between BMD and N/L, P/L is higher in PMO. Platelet/Lymphocyte is an easily accessible, cost-effective, and specific marker for inflammation that can help determine osteopenia and PMO, as well as the case of low Vit-D levels. However, there is need for further studies including larger patient groups.
Acknowledgment
The authors gratefully acknowledge Souphi Zitouni for radiologic support and David Chapman for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 28, 2019.
- Accepted February 14, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.