


Abstract
Objectives: To characterize and meta-analyze the pertinent studies concerning celiac disease (CD) among patients with type 1 diabetes mellitus (T1DM) in the Kingdom of Saudi Arabia.
Methods: Data (from the relevant articles) were analyzed using both the Statistical Package for Social Sciences, version 20 (IBM Corp., Armonk, NY, USA) program and the comprehensive meta-analysis (CMA) program. This study was conducted between March and July 2018 at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia. Written ethical approval was not obtained because this study was a retrospective literature review and analysis.
Results: The prevalence of seropositive-CD was 15.88% with high heterogeneity (I2=84.0), while the prevalence of biopsy-proven CD was 12% with high heterogeneity (I2=82.7). Anti-transglutaminase was used in 7 of the 8 studies; alone in 4; with endomysial antibodies in 2; and with antigliadin antibodies (AGA) in one. In the remaining study, antireticulin antibodies was used with AGA. The age of the involved patients ranged from 8 months to 50 years old.
Conclusion: The prevalence of biopsy-proven CD among T1DM patients in Kingdom of Saudi Arabia (12.0%) was double the global prevalence (6.0%), and much higher than the normal Saudi population (1.4%). The female-to-male ratio (2:1) of CD patients in T1DM was the same as in the normal population in Kingdom of Saudi Arabia. No significant difference was detected between the reported serologically-proven rates and the reported biopsy-proven rates (p=0.093).
Studies concerning the association between celiac disease (CD) and type 1 diabetes mellitus (T1DM) started to appear in the middle of the last century.1,2 Studies concerning the prevalence of CD among patients with T1DM showed high heterogeneity and contradiction (1.4->10%).3-5 Nevertheless, screening for CD in patients with T1DM was often recommended.6 Additionally, some studies concerned with T1DM in CD patients showed that the risk of T1DM in CD was doubled before the age of 20 years.7 In the Kingdom of Saudi Arabia,8,9 the first study10 concerning the CD in T1DM appeared in 2003, followed by another 7 studies, the last of which was published in 2018.10-17 The current study represents characterization and meta-analysis for these studies concerned with CD among patients with T1DM in Kingdom of Saudi Arabia.
Methods
This study was conducted between March and July 2018 at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia. The involved data were part of our previous comprehensive systematic retrospective review and analysis.8 Data analysis was performed using 2 programs; the Statistical Package for Social Sciences (SPSS), version 20 (IBM Corp., Armonk, NY, USA) program and by the comprehensive meta-analysis (CMA) program, version 3 (Biostat, USA). I-squared (I2) has been used to evaluate heterogeneity. Interpretation of I2 values was as follows: 0% (for nil heterogeneity), <25% (for low heterogeneity), 25-49% (for moderate heterogeneity), and >50% (for high heterogeneity).18 For the illustration of the results, we used tables, figures, and diagrams. We considered the results as significant if the p-value was less than 0.05.
Strategies used om the sytematic search and study selection
The systematic search involved 3 steps. The first step was a comprehensive database and journal search.8 In this step, the following keywords were used: 1) prevalence of celiac disease in Saudi Arabia, 2) celiac disease in Saudi Arabia, and 3) celiac disease in Saudi children. We performed a retrospective search, with no specific period, via PubMed (US National Library of Medicine), Ovid, EBSCO, and Google Scholar. We also searched via the library of King Fahd Research Centre in King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia, and via the Editorial Department of the 2 journals of King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia (the Medical Science journal and the Saudi Journal of Internal Medicine). Duplication of the obtained articles was checked via their titles, date of publication, and authors. This step was followed by 2 selection steps (inclusion/exclusion) for the pertinent studies. The second step involved selection (inclusion) for those articles concerning celiac disease in Saudi Arabia.8 The third step involved selection (inclusion) for the articles concerned with T1DM, and their data were stored as a separate SPSS file that was used in this study.
Strategy for age grouping
Keeping in mind that the ages of 10 years (for females) and 12 years (males) are the cut-off levels for puberty14 and that the ages of 1-18 years corresponds to children and adolescents;13,14,19 studies were divided (age wise) into groups: pediatric (for males that are <12 years, and for females that are <10 years), adults with adolescents (>12 years), pediatric with adults (>1 year), and pediatric with adolescents (1-18 years).
Results
Characteristics of the patient studies
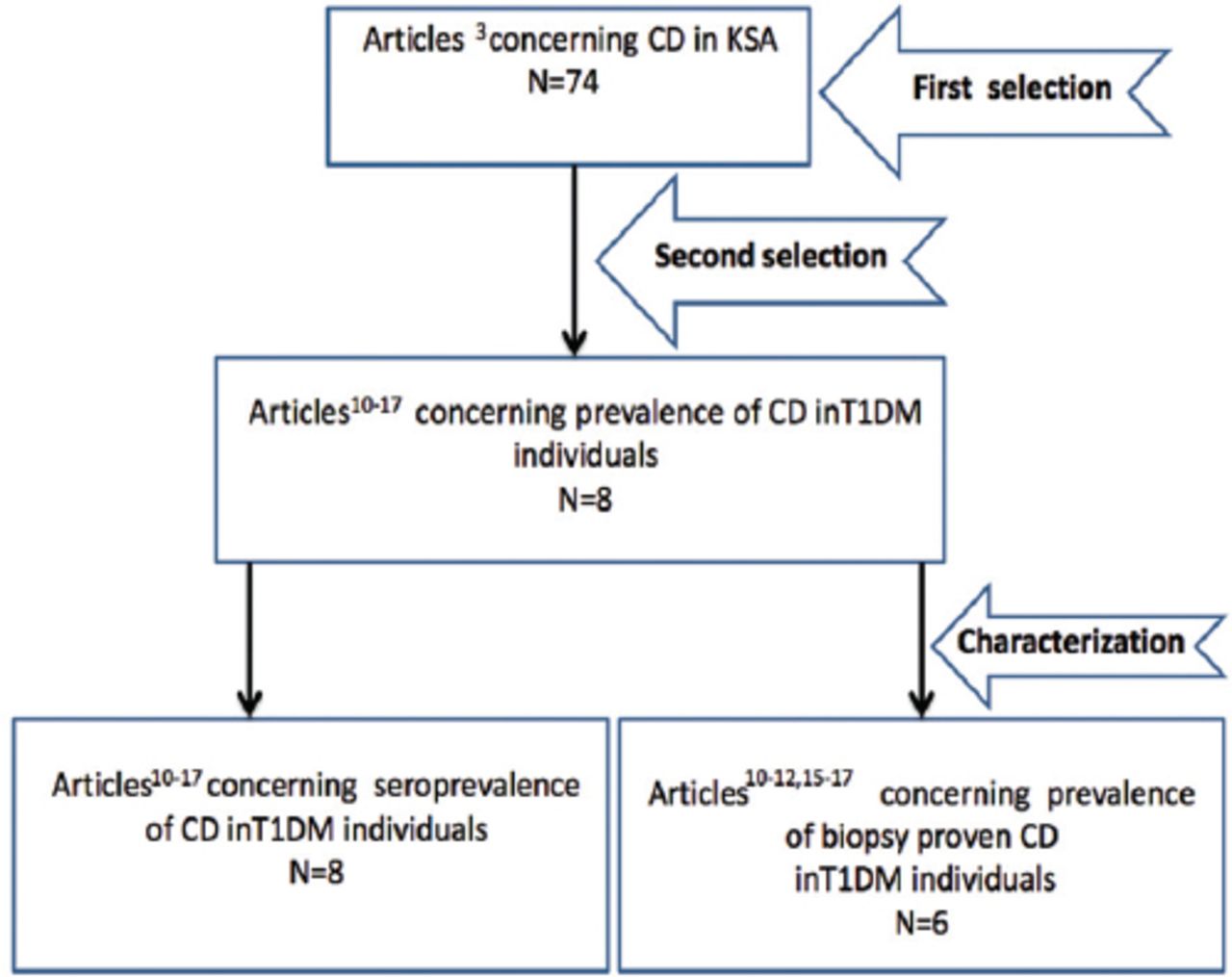
At the end of the systematic search and study selection, 8 studies were retrieved (Figure 1). Data of the 8 studies were recorded in a separate SPSS file. The characterization of the studies is shown in Table 1. The 8 studies were arranged chronologically according to the year of publication; covered a wide range of ages (8m-50 years) and 2 types of age groups: children and adolescents (4 articles), children and adolescents and adults (4 articles). These studies covered 3 regions in Kingdom of Saudi Arabia: Riyadh (2 studies), the Western region (4 studies), and the Southern region (2 studies). Cohorts and positivity rates of the serologically-proven status and biopsy-proven status are also shown in Table 1. The total cohorts (of T1DM) is illustrated in Table 2. The total number of CD positivity, and rates for both seropositivity- and biopsy-proven positivity. The total cohort of CD seropositivity was 1685 (range was 106-430), with a total CD positivity of 244 and positivity rate of 14.4%, while the total cohort for CD biopsy-proven was 1215 (range was 106-430) with a total positivity of 132 and positivity rate of 10.8% (Table 2). However, higher rates were obtained by meta-analysis for both seropositivity (15.8%) and biopsy-proven positivity (12.0%) (Table 2). The cohort, seropositivity rate and biopsy-proven rate of CD among T1DM patients in each of the retrieved studies are shown in Table 1 and Figure 2.
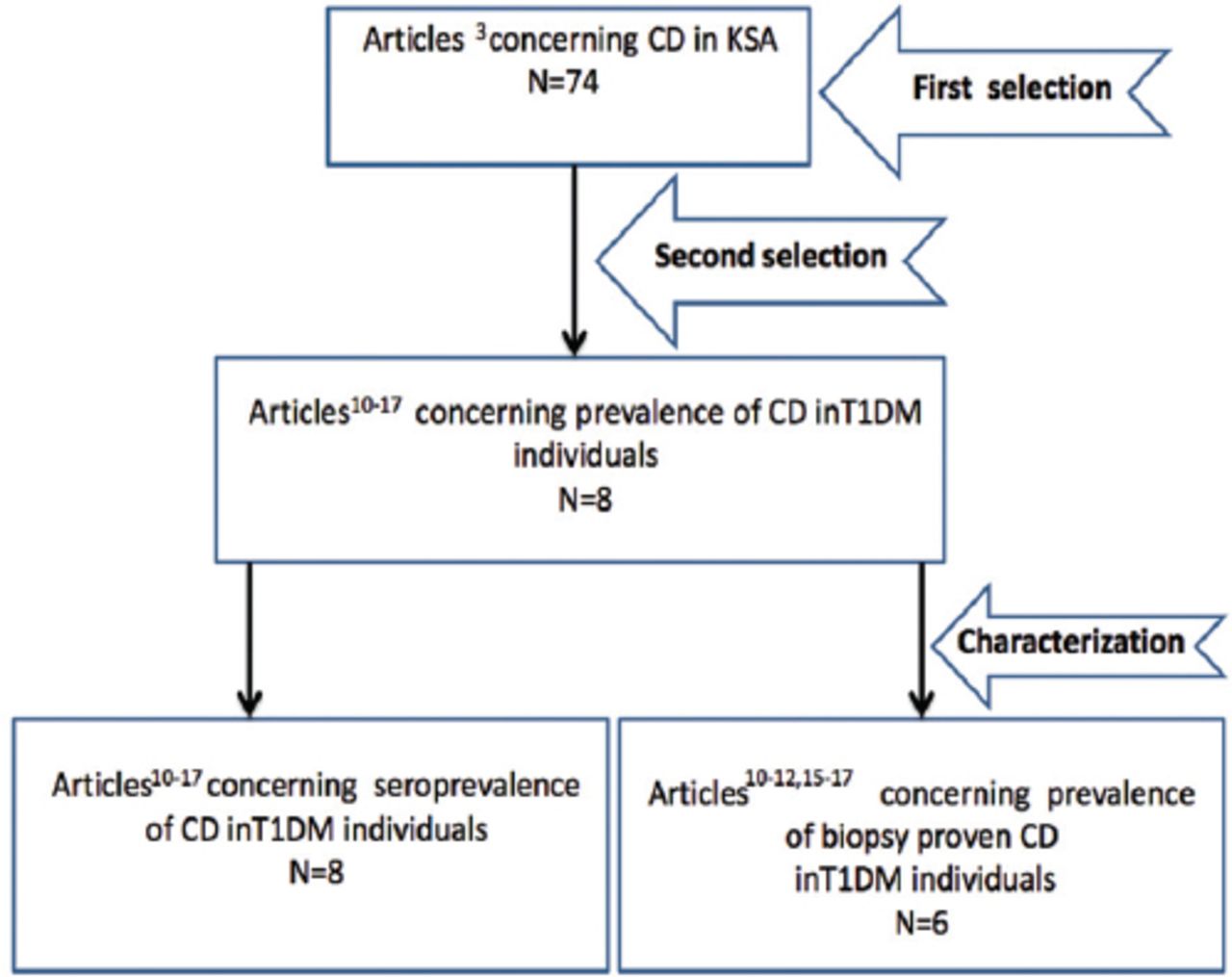
PRISMA flow-diagram showing the selection process of the pertinent studies. CD- celiac diseases, KSA - Kingdom of Saudi Arabia, T1DM - type 1 diabetes mellitus.
Characterization of the pertinent studies.
Rate of celiac disease in type one diabetes mellituspopulation; comparison between meta analysis and traditional statistical analysis.
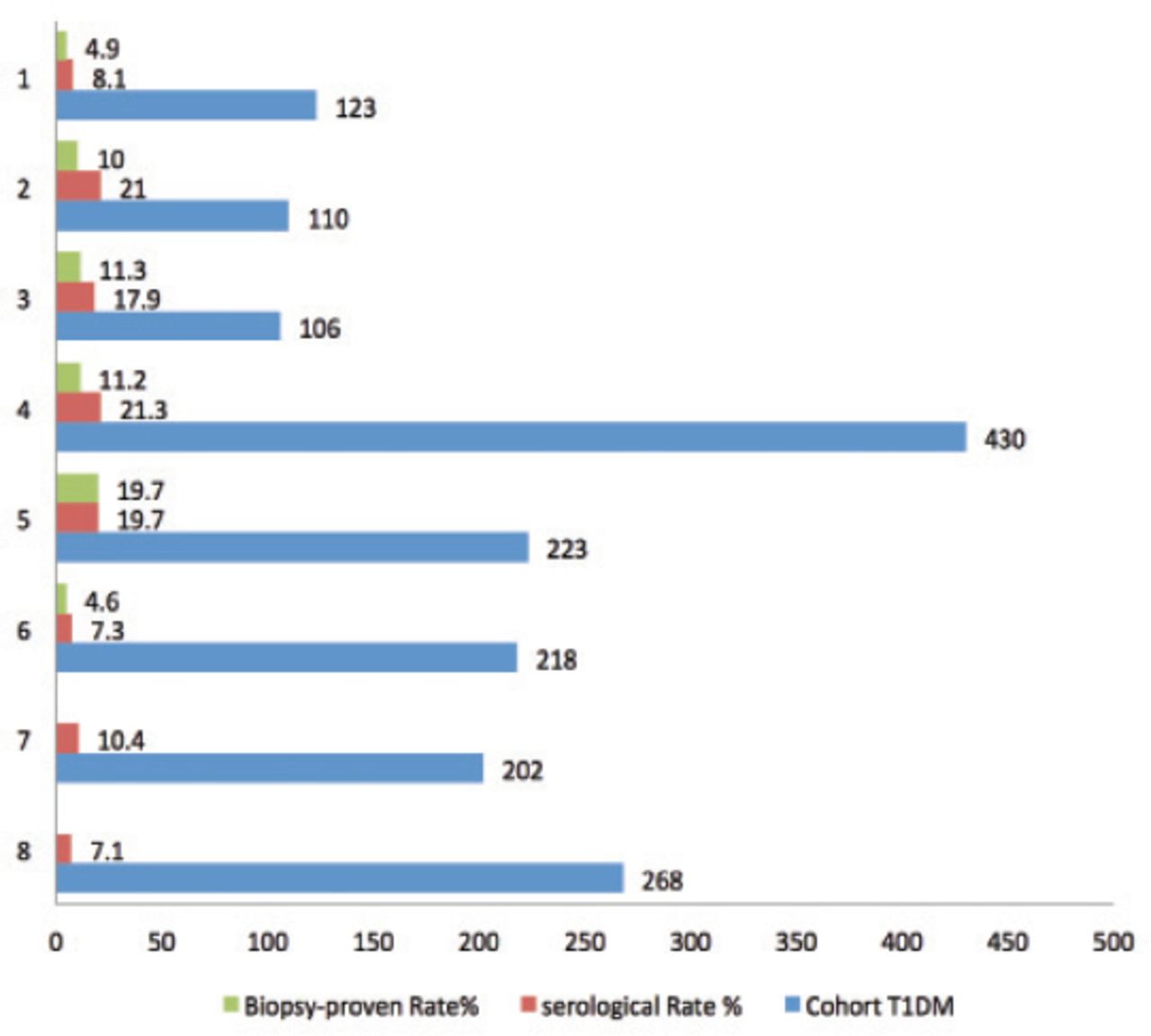
Sample size and prevalence (seropositivity rate and biopsy-proven rate) of celiac disease among type 1 diabetes mellitus patients in the retrieved studies. Al-Ashwal AA et al 200310 (1), Saadah OI et al 200411 (2), Al-Hussaini A et al 201212 (3), Saadah OI et al 201213 (4), Al-Agha AE et al 201514 (5), Al-Hakami AM 201616 (6), Alshareef MA et al 201615 (only seropositivity rate) (7), Alghamdi RA et al 201817 (only seropositivity rate) (8).
Female to male ration
Gender information was found in 5 studies.10,12,15-17 The female:male ratio was 2:1 (60:29) (Table 1).
Duration span
The included 8 studies were published between 2003-2018, covering different periods: in Riyadh region (1995-1996 and 2008-2010); in the Western region (retrospectively until 2004, retrospectively until 2015, January 2013-2014 and January 2008 and June 2009); and in the Southern region (Aseer) (March 2013 and June 2014) and retrospective record based until 2018 in the Southern region (Al-Baha) (Table 1).10-17
The pattern of serology and biopsy
Anti-tissue transglutaminase (anti-tTG) was used in 7/8 studies; alone in 4; with anti-endomysium antibody (EMA) in 2; and with anti-gliadin antibody AGA in one. Antireticulin antibodies (ARA) was used with AGA in the remaining study. A biopsy was used in 6/8 studies (Table 1).
The worldwide prevalence of CD in T1DM patients, as noted in the retrieved studies
The worldwide prevalence was mentioned in 5 of the retrieve studies (Table 3). Al-Ashwal et al,10 mentioned a prevalence of 1.2% (Finland in 1996) and 11.1% (in Italy in 2000).20,21 Al-Hussaini et al,12 mentioned a prevalence of 5.4% (in France in 2005), 10.4% (in Denmark in 2001), 5.1% (North America [USA] in 1998), 2.6% (in Argentina in 2006), 13.9% (in Brazil in 1996), and 16.4% (Algeria in 1996).22-27 Saadah et al,13 mentioned a prevalence of 6.8% (Italy in 2004), 1.6% (France in 2007), 0.6% (Germany in 2004), 10.4% (Denmark in 2001), 16.4% (in Algeria in 1996), 5.3% (Tunisia in 2007), and 10.3% (in Libya in 2003).3,23,27-31 Alshareef et al,15 reported prevalences from Arab regions as follows: Algeria (16.4%), Tunisia (5.3%), Eygpt (11.2 and 5.4%), and Libya (11%).15,27,30,32,33 Al-Hakami,16 mentioned a prevalence of 1.6% in France, 3.3-4.0% in the United Kingdom, 4.6-7.0% in the United States of America, 3.6-6.6% in Italy, and 9-9.7% in Sweden.5 These worldwide prevalences (as mentioned in the retrieved studies, ranged from 0.6% (one in every 166 patients in Germany) to 16.4% (one in every 6 patients in Algeria).27,29
The worldwide prevalence of celiac disease in type one diabetes malittus patients as mentioned in 5 of the retrieved studies.
Meta-analysis
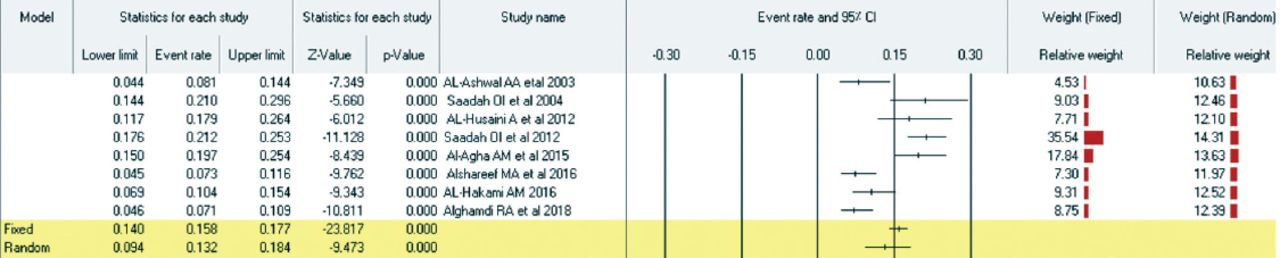
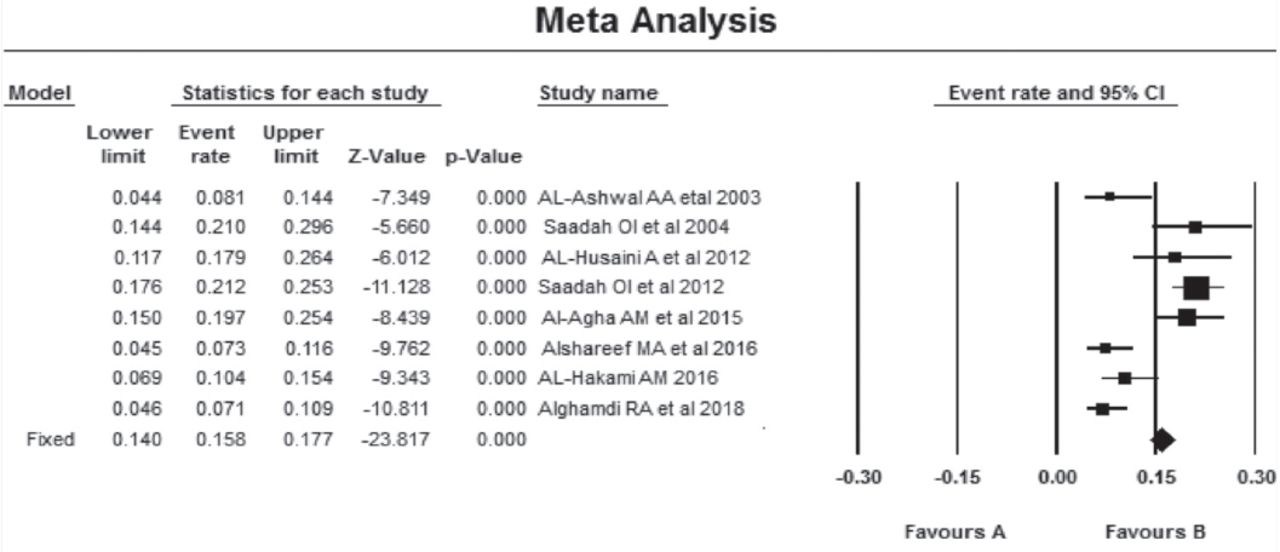
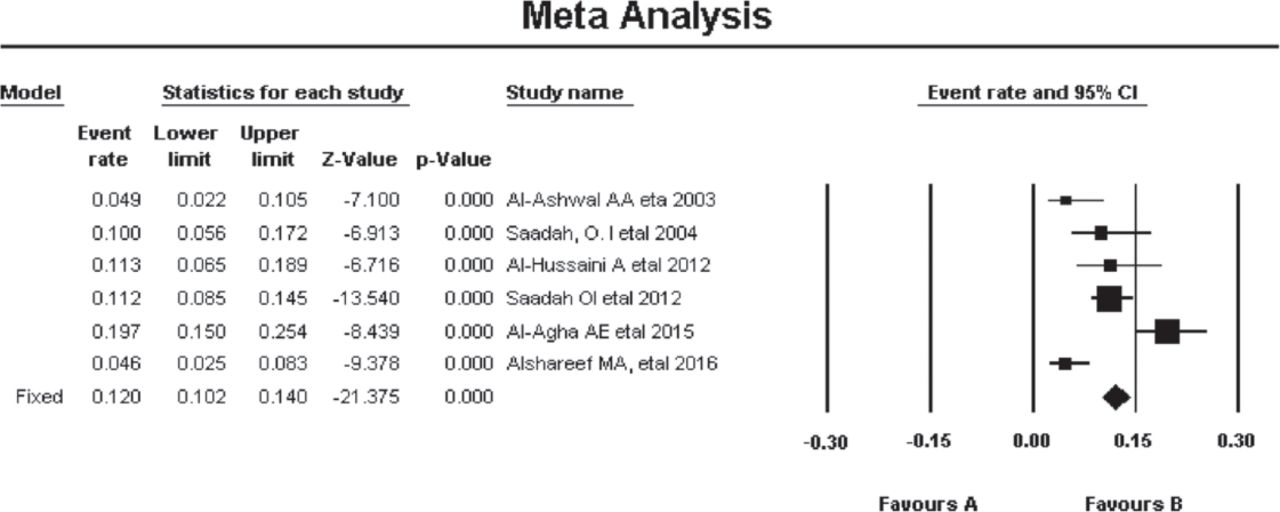
Using the CMA program, we performed a meta-analysis for the eight studies concerning seroprevalence of CD in T1DM individuals (articles 10-17), and for 6 studies concerning the prevalence of biopsy-proven CD in T1DM individuals [articles 10-15]. Results of the meta-analysis for seropositivity prevalence (Tables 4 and 5; and Figures 3 and 4) show that the prevalence (by fixed model) for the serologically proven CD (by at least one serological test) was 15.8% (95%CI = 14.0-17.7) with high heterogeneity (I2=85.84); and the meta-analysis (Tables 6 and 7; and Figures 5 and 6) for the prevalence of the biopsy-proven CD (6 studies; by fixed model) was 12.0% (95%CI = 10.2–14.0) with high heterogeneity (I2 = 82.71).
Data for meta analysis of seropositivity prevalence of celiac disease among type one diabetes mellitus in Kingdom of Saudi Arabia.
Seropositivity prevalence(by fixed and random models) with the heterogeneity between studies.

Seroprevalence (by fixed and random models) with statistics and relative weight for each study.
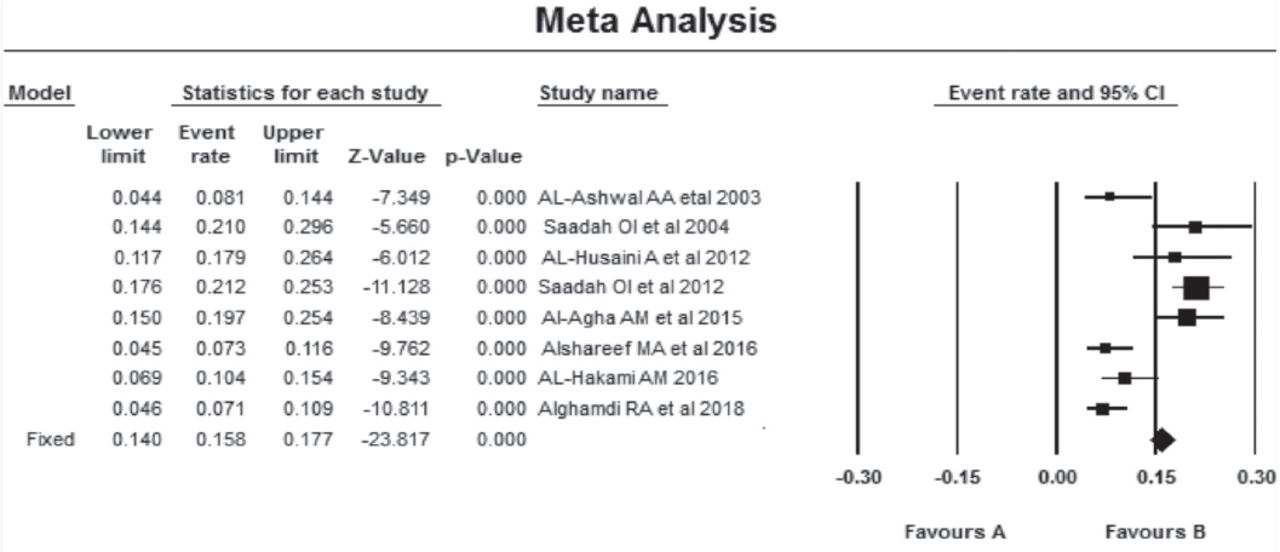
Forest plot for prevalence of seropositive celiac diseases among type one diabetes mellitus in the Kingdom of Saudi Arabia.
Data for meta analysis of biopsy-proven positivity for type one diabetes mellitus.
Prevalence of biopsy-proven celiac disease in type one diabetes mellitus (by fixed and random models) with statistics and relative weight for each study.

Prevalence of biopsy-proven CD (by fixed and random models) with statistics and relative weight for each study. CD- celiac diseases, KSA - Kingdom of Saudi Arabia, T1DM - type 1 diabetes mellitus.
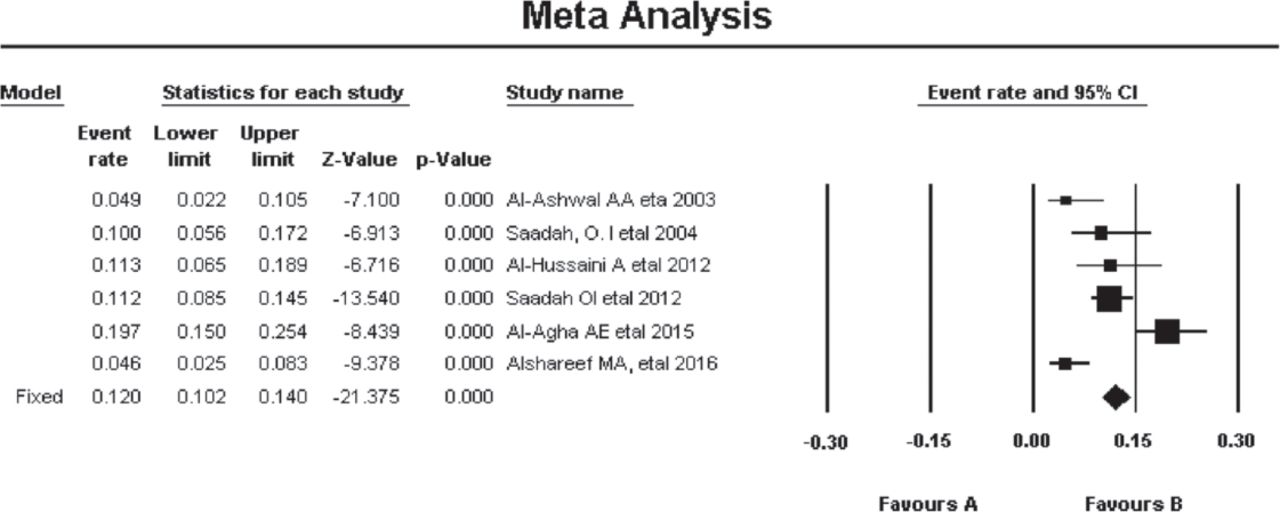
Forest plot for prevalence of biopsy-proven celiac disease among type 1 diabetes mellitus in Saudi Arabia. CI - confidence interval
Discussion
There was a gap of 50 years between the first global publication1 for a relation between CD and T1DM (in 1954) and the appearance of the first related 2 Saudi studies10,11 in 2003 and 2004; followed by a gap of 8 years until 2012 when another 2 Saudi studies appeared.3,12 So far in the Kingdom of Saudi Arabia, only 8 studies concerning CD among T1DM were retrieved via a recent systematic review.8,9 When Al-Ashwal et al10 reported (in 2003) a prevalence of 4.9% for the biopsy-proven CD in T1DM in Kingdom of Saudi Arabia, at that time the worldwide prevalence (of CD in T1DM) was 1.2-11.1%, with the exceptions of Argentina (13.9%) and Algeria (16.4%).20,21,23-25,27,34-38 In the current meta-analysis, 12.0% of T1DM individuals had biopsy-verified CD (95% CI: 10.2-14.0) with high heterogeneity (I2=82.7), which was double the global prevalence (6.0%); according to the systematic review (between 2000 and May 2014) of Elfstrom et al,5 only one study reported a similarly high prevalence (12.3% in 2006) among Danish children;39 in addition to Argentina (13.9%) and Algeria (16.4%), both in 1996.25,27 Celiac disease among T1DM in Kingdom of Saudi Arabia involved a wide range of ages (8 months to 50 years), indicating that both children and adults with T1DM have an increased risk of CD; a phenomenon that was already described to exist in T1DM7 but not in T2DM.40 The female-to-male ratio of CD patients among T1DM was 2:1, which is the same as in the normal population in Kingdom of Saudi Arabia.41 The total cohort of seropositivity was 1685 T1DM patients (range was 106-430), while the biopsy-proven total cohort was 1215 (range was 106-430), indicating that the lowest cohort among the Saudi studies was 106. Low cohorts were also found among non-Saudi studies, including 84 T1DM Mexican Mestizo adults patients, 92 patients in Italy, and 83 T1DM children in Iran.42-44
In the current study, anti-tTG was used in 7/8 studies (alone in 4; with EMA in 2; and with AGA in one), while one study used ARA with AGA without anti-tTG or EMA. This type of serological pattern shows that only one study (Al-Ashwal et al10) did not use anti-tTG despite its high sensitivity and specificity (IgA-tTG sensitivity [98%] and specificity [98%]).45,46 This can be attributed to the unavailability of this test at the time of their research (1995-1996); as well as the development of ELISA-based tTGA tests introduced in 1999 following the identification of the specific tissue transglutaminase autoantigen (tTG2) in 1997.47,48 Anti- tTGA tests were preceded by serological tests for ARA (1977), AGA (1983), and EMA (1984).49-51 Al-Ashwal et al10 also did not use EMA, despite its availability before 1995,51 and despite its high sensitivity (95%) and specificity (99%).45,46,51 This might be because the authors used ARA, which also has high sensitivity (72%) and specificity (99%) and because both EMA and ARA are costly, time-consuming, and introduce inter-observer variability (both are immunofluorescent assays requiring an individual reading of each sample under a fluorescent microscope).45,46,52 Additionally, IgG-EMA (in comparison to IgA-EMA) strongly increases the prevalence of CD in patients of T1DM.43 The increased prevalence of the double autoimmunity individuals (CD and T1DM) can be explained by the overlap of genetic variants (including HLA and non-HLA) between the 2 diseases (T1DM and CD). Several non-HLA loci (such as CTLA4 and IL2RA overlap between T1DM and CD that can introduce risk to double autoimmunity.53,54 The most important HLA loci are HLA-DQ2 (found in approximately 55% of T1DM patients and 90% of CD patients) and HLA-DQ8 (found in approximately 70% of T1DM patients and only 10% of CD patients).55
HLA-DQ2 and DQ8 alleles were found to be the main genetic risk factor for CD.56 Additionally, individuals who possess the HLA haplotypes DR3-DQ2 and DR4-DQ8 were found to have an increased risk for T1DM of nearly one in 20;57 DQ2/DQ8 genotype carries a strongly increased risk of developing T1DM in European populations.58 This genetic association indicates common pathogenic pathways between CD and T1DM.59,60 Global frequencies of HLA DQ ranging 0-28% for HLA DQ2 and 1-9% for DQ8.61 Among Saudi population 52.7% possess the HLA-DQ allele (48.5% for DQ2 and 17.2% for DQ8), making them the highest HLA-DQ genotypes among healthy general populations.62 This (in addition to the genetic association between CD and T1DM; as demonstrated above) may explain the high prevalence (double compared to other countries) of CD among T1DM.
The combined HLA and non-HLA genetic loci constitute 50% of the CD heritable factors, while the remaining 50% heritable factors still have to be demonstrated.63 However, by virtue of the recent genome-wide association studies (GWAS), additional non-HLA loci were demonstrated that are associated with CD.64-66 Additional associations (by virtue of GWAS) have been identified for the single nucleotide polymorphisms (SNPs) with autoimmune conditions, including T1DM and CD.67
Study limitations
There are 3 main limitations in this study. One limitation is the limited number of the involved CD patients (only 1685 serologically-proven and 1215 biopsy-proven patients). Another limitation is the lack of uniformly performance of small intestine biopsies in the serologically-proven CD patients. A third limitation is the lack of anti-tTG test in one study; a point which was discussed thoroughly earlier in this discussion.
In conclusion, the prevalence of biopsy-proven CD among T1DM in the Kingdom of Saudi Arabia was double the global prevalence, and much higher than Saudi normal population. The female-to-male ratio of CD patients in T1DM was the same as in normal population in Kingdom of Saudi Arabia. No significant difference between the reported serologically-proven rates and the reported biopsy-proven rates (p=0.093).
Footnotes
Disclosure. The author has no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 13, 2019.
- Accepted May 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.