


Abstract
Objectives: To assess the insertion and ventilation of the laryngeal mask airway (LMA) classic while using different head positions with or without muscle relaxant.
Methods: This is a double-blind randomized clinical trial. Patients scheduled for ureteral calculus surgery at Shanghai General Hospital, Shanghai, China were recruited between November 2017 and November 2018. A total of 132 adults were consecutively selected. Patients were randomly divided into 4 groups according to head positioning and muscle relaxant use. An 8-cm-high pillow was used to achieve the sniffing position. The insertion time, initial peak pressure (Ppeak), mean pressure (Pmean) of the airway during intermittent positive pressure ventilation (primary endpoint) and fiberoptic score of the LMA position (secondary endpoint) were evaluated via electronic bronchoscopy through the mask bar. All adverse events were recorded.
Results: Data were analyzed by ANOVA, 2-way ANOVA, Chi-squared, Cochran-Mantel-Haenszel, and Kruskal-Wallis tests. The insertion time required for the first attempt, fiberoptic score, Ppeak and Pmean did not differ among the groups. However, the incidence of adverse events in groups not using muscle relaxant was higher than in those using muscle relaxant.
Conclusion: Use of a sniffing position and muscle relaxant slightly eased the insertion of the LMA but did not affect the fiberoptic score or ventilation parameters. Using a muscle relaxant, but not the sniffing position, reduced the incidence of adverse effects.
It has been more than 20 years since the laryngeal mask airway (LMA) has been used in clinical anesthesia. Unlike intubation, the LMA creates a tight airway by enclosing the larynx, thereby avoiding airway obstruction in the oropharynx.1 Because it is easy to insert and associate with lower complication rates, the LMA has been increasingly used by many facilities for various conditions.2-4 The sniffing position, in which the neck is bent and the upper cervical spine is extended, has been suggested for optimal LMA placement.1 However, studies have shown that head positions have different effects on the rate of successful LMA placement and tracheal intubation. Various authors have shown that the success rate of LMA placement does not differ among head positions.5-7 Similarly, a study by Jun et al8 showed no significant changes in the view through the fiberoptic bronchoscope while changing head positions. In patients with cervical immobilization, the LMA classic can also provide a rapid and reliable airway.9 However, these previous studies were performed on patients using muscle relaxants. The LMA is typically used for short-duration surgeries. The placement and ventilation of the LMA can be performed without a muscle relaxant,1,10,11 which may facilitate quicker recovery from general anesthesia. Both the head position and the use of muscle relaxant may influence the placement and ventilation of the LMA, but their combined effects on LMA ventilation have rarely been studied.
Therefore, we proposed this clinical trial to assess the impact of head position and the use of muscle relaxant on the insertion and ventilation of the LMA classic.
Methods
We obtained ethical approval for the study from the Medical Ethics Committee of Shanghai General Hospital (certificate No. 2017KY227). The trial was designed in accordance with the principles of the Helsinki Declaration, registered at the Chinese Clinical Trial Registry Center. All patients provided written informed consent before being recruited for this trial. We searched PubMed using laryngeal mask and sniffing position or muscle relaxation as key words to identify relevant articles.
The inclusion criteria were as follows: aged 20-70 years, American Society of Anesthesiologists physical status of 1 or 2, patient agreement to accept general anesthesia for selective ureteroscopic surgery for ureteral calculi. The exclusion criteria were obesity (body mass index [BMI] >30), loose or missing teeth, neck disease, inability to maintain the sniffing position, and any contraindication for the LMA classic, such as a full stomach, throat disease, and pregnancy. All patients were randomly divided into 4 groups according to the number in an envelope: 1) S-M group: sniffing position, with a muscle relaxant; 2) N-M group: neutral position, with a muscle relaxant; 3) S group: sniffing position, without a muscle relaxant; and 4) N group: neutral position, without a muscle relaxant. An 8-cm pillow was placed under the patient’s shoulder and neck to maintain the sniffing position while patients just lay down on the operating table, and 2 pillows were placed beside the head for the neutral position. The head and pillows, but not the airway, were covered by sheets.
When the patient arrived at the operating room, a 20-gauge intravenous perfusion tube was inserted into the dorsal vein, and 500 ml of Ringer’s lactate solution was infused. Electrocardiography, pulse oximetry, and the end-expiratory anesthetic concentration were monitored throughout the study. For induction and intubation, 2 mg/kg propofol, 2 µg/kg fentanyl were used for the S and N groups, and an additional one mg/kg of succinylcholine was administered to the S-M and N-M groups. Ventilation was performed through a face mask for 2 minutes, followed by a placement of an appropriately sized LMA (3-5#, Tuoren, Henan, China) by the same anesthesiologist who was blinded to the patient group. Another anesthesiologist recorded the insertion time and the rate of successful placement of the first attempt. The insertion time was recorded when the operator opened the subject’s mouth until her hands removed from the LMA. The success of the LMA was determined by a normal square wave on the capnogram. If mechanical ventilation could not be performed or severe gas leakage through the mouth was observed, the placement was considered a failure and was reattempted after one minute of ventilation through the face mask. After 3 unsuccessful attempts, the LMA placement was recorded as a failure. If mechanical ventilation was possible and no leakage from the mouth was observed, the LMA was fixed in position, and the patient’s head was covered with sheets. Ventilation assistance was provided with a ventilator with the parameters: intermittent positive pressure ventilation mode; tidal volume, 7 ml/kg; rate, 12/minute; time of inspiration: time of expiration (TI:TE), 1:2; oxygen 100%, 2 l/min; maintenance of anesthesia with sevoflurane; minimum alveolar concentration, 1.0-1.2. Data from the first ventilation attempt also included the peak pressure (Ppeak) and mean pressure (Pmean) of the airway. The fiberoptic score (LF-GP, Olympus, Japan) was graded12-13 as follows: a) 4- only vocal cords could be observed; b) 3- vocal cords and posterior epiglottis could be observed; c) 2- vocal cords and anterior epiglottis could be observed; d) 1- vocal cords could not be observed, but ventilation was possible; and e) 0- vocal cords could not be observed, and ventilation was not possible. The LMA was removed after surgery at the discretion of the anesthesiologist. The following adverse events were recorded: vomiting, blood on the LMA surface, sore throat and nausea. A nurse who was also blinded to the study data recorded the adverse events while the patients were in the post anesthesia care unit.
Data are shown as the mean±SD (95% confidence interval), number of patients or n(%). We analyzed the data using Statistical Package for Social Sciences for Windows version 19.0 (IBM Corp, Armonk, N.Y., USA). Patient characteristics, including age, height, body weight, BMI were examined using student’s t-test. The LMA insertion time, Ppeak, and Pmean were compared by ANOVA. In addition, 2-way ANOVA was used to test the influences of sniffing position and muscle relaxation on the insertion time, Ppeak and Pmean. The gender ratio, success rate, and incidence of adverse events were compared using a Chi-squared test. The Cochran-Mantel-Haenszel test was used to analyze the influences of head position and the use of muscle relaxant on the incidence of adverse events associated with the LMA. We used the Kruskal-Wallis test to compare the fiberoptic scores. A p-value of <0.05 was considered to indicate significant differences.
We used G* Power (version 3.1.9.2, Germany) to calculate the sample size. In our preliminary study, which included 5 patients per group, the mean insertion times for each group were as follows: S-M: 9.25±2.16 seconds, N-M: 9.87±1.67 seconds, S: 11.48±2.35 seconds and N: 10.84±0.89 seconds. The total sample size was 108, which was calculated based on an effect size of 0.41, a power of 95%, and an a value of 0.05. Considering a 20% dropout rate, we adjusted the sample size to 132 (33 in each group)
Results
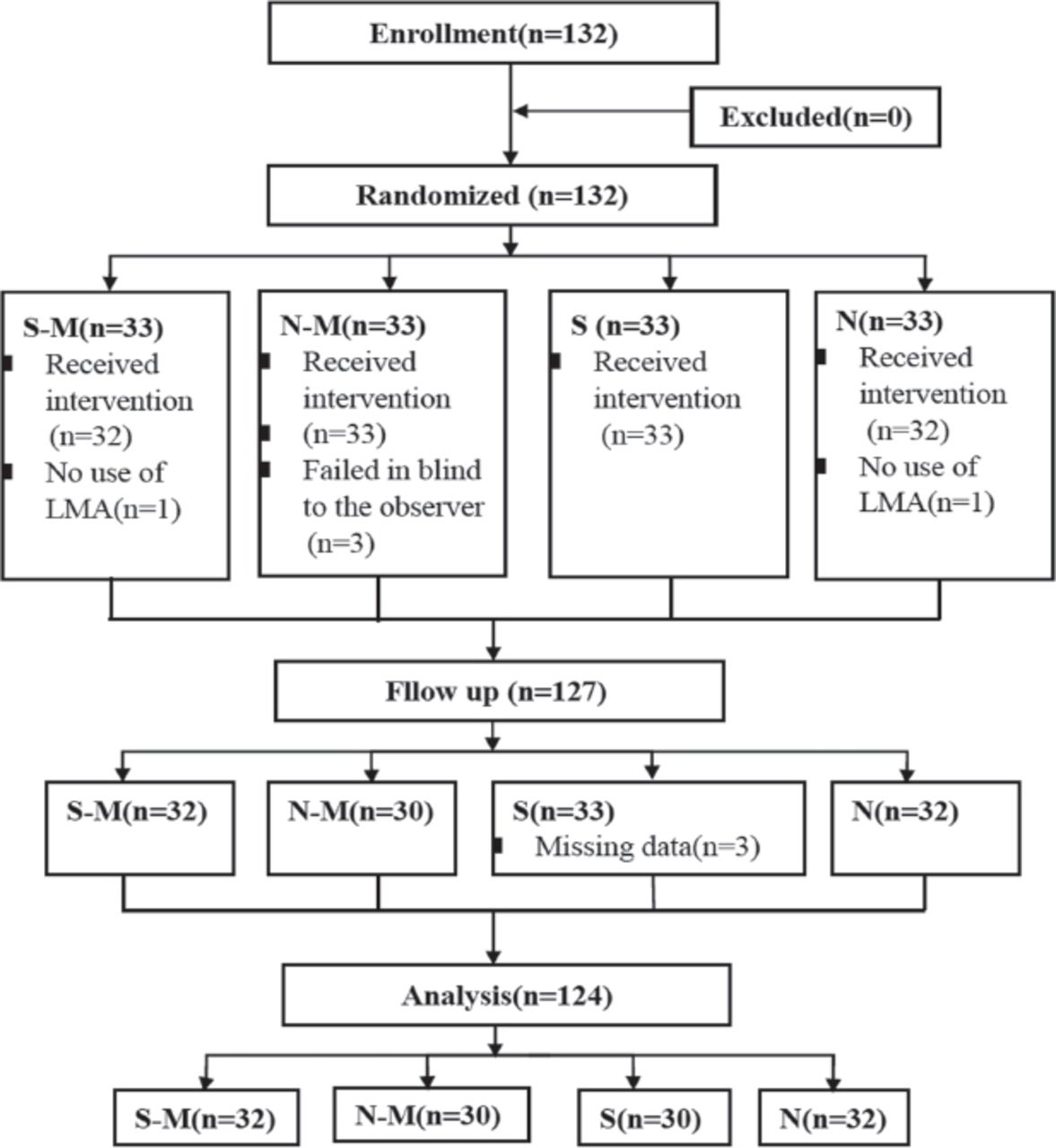
A flow chart of the study is shown in Figure 1. We recruited a total of 134 patients, and data from 124 subjects were analyzed. Differences in the demographic data were not significant among the 4 groups. No significant differences were found for the insertion time, Ppeak and Pmean among the 4 groups (Table 1). The insertion time was 9.50±4.47 seconds in the S-M group, 9.83±3.36 seconds in the N-M group, 9.27±3.21 seconds in the S group and 10.94±4.02 seconds in the N group, and none of the differences among the groups were significant (p=0.332). Two-way ANOVA showed that muscle relaxant use may influence the Ppeak of the airway (p=0.048) (Table 2). The success rate on the first attempt was 93.90% in the S-M group, 93.3% in the N-M group, 90% in the S group and 84.4% in the N group, with no significant differences among the 4 groups (Table 1). The fiberoptic scores also did not differ among the 4 groups (Table 3, p=0.387).

The study flow chart of 132 patients for selective ureteroscopic surgery for ureteral calculi.
Insertion time and success rate of the first attempt, peak pressure and mean pressure of the 4 groups.
Results of the 2-way Analysis of Variance of the influence of sniffing position and muscle relaxation use on the insertion time at the first attempt, peak pressure and mean pressure.
The different fiberoptic scores in each group (N=124).
On the other hand, the incidences of adverse events differed among the 4 groups. The incidences in the S (33%) and N (31.3%) groups were significantly higher than those in the other groups (9% and 10%) (Table 4). We used the Cochran-Mantel-Haenszel test to examine the reason for this difference. When head position was controlled as a layer, the p-value was 0.022 for the sniffing position and 0.039 for the neutral position, and the odds ratio was 4.44 (without head positioning/with head positioning). When the muscle relaxant use was controlled as a layer, the head position of the patients had no impact on the incidence of adverse events associated with the LMA (Table 5). Therefore, muscle relaxant use was the reason for this difference in adverse events among groups.
Type and incidence of adverse events in the study (N=124).
Type and incidence of adverse events in the study (N=124).
Discussion
The LMA has been increasingly used due to its high success rate and low complication rates. The total success rate of the first attempt was 96.8%. The insertion time was 9.50±4.47 seconds in the S-M group, 9.83±3.36 seconds in the N-M group, 9.27±3.21 seconds in the S group and 10.94±4.02 seconds in the N group (p=0.332), which are very short times. The total adverse event rate was 20.96%, and no severe complications were observed. Additionally, the LMA can be smoothly inserted by doctors without experience with the device,14 making it an excellent supraglottic airway device for atypical and difficult airways.
The sniffing position could improve the laryngeal view during direct laryngoscopy compared to that achieved with the neutral position.15-17 The sniffing position has also been recommended for the standard LMA, but our study found that the sniffing position did not affect the first-attempt success rate, placement time or fiberoptic score. All groups achieved satisfactory ventilation. These findings were consistent with those of previous studies.8 The ease of LMA placement depends on the location of the larynx; a posteriorly located larynx may block the downward path of the mask tip. Therefore, it is easier to place the LMA behind a more anterior larynx. The sniffing position may not be helpful in this case. Therefore, patient factors, such as cervical damage and the need for quick placement of the LMA in an emergency, should be considered when choosing the head position rather than automatically using the sniffing position.
Using a muscle relaxant shortened the LMA insertion time, but the differences among the groups were not significant. Satisfactory ventilation was also achieved without a muscle relaxant. Another study by Fujiwara et al10 showed that muscle relaxants increased the successful placement rate and sealing pressure of the ProSal device and reduced the subjective difficulty of placement; the impact of muscle relaxants on the high placement efficacy was potentially due to the muscle relaxant increasing the pharyngeal space.18 In our study, the LMA classic was used, which has only one cuff; therefore, an increased pharyngeal space did not obviously contribute to the quicker insertion and higher success rate. Nonetheless, the incidence of adverse events in the groups using muscle relaxant was much lower than in the groups without muscle relaxant regardless of the head position (Table 3). When the head position was controlled as a layer, the p-value was 0.022 for the sniffing position and 0.039 for the neutral position. Therefore, muscle relaxation explained this difference in adverse events (Table 4). Additionally, the odds ration was 4.44; thus, the incidence of adverse events associated with the LMA in the group without muscle relaxants was 4.44 times that of the group that received muscle relaxants. When muscle relaxant use was controlled as a layer, the head position showed no influence on the incidence of adverse events associated with the LMA. Studies have shown that the trauma during placement is the main cause of sore throat in ventilated patients.19 When a muscle relaxant is not used, more strength/pressure is needed to insert the LMA, which may damage the throat, leading to blood on the cuff and sore throat. Our results also showed that muscle relaxation use may influence the Ppeak of the airway, perhaps due to the increase in thoracic compliance. High airway pressure may increase the likelihood of stomach inflation, leading to nausea and vomiting.20 Because we used only a short-acting muscle relaxant in our study, we did not assess the degree of neuromuscular blockade. Therefore, the effect of the muscle relaxant probably lasted for only the first few minutes and not for the entire duration of the anesthesia. Nevertheless, the use of muscle relaxants only during the placement phase could reduce the rate of adverse events associated with the LMA.
In a successful LMA insertion, the fiberoptic score should be ≥2, and the vocal cords should be visible.13 Among the 124 patients, 100 (80.6%) had scores ≥2. All patients could be ventilated, which indicated that good ventilation was achievable through the LMA, even in difficult locations. Among the 26 patients with complications, such as sore throat and nausea, 11 patients had scores of ≤1, and 15 patients had scores of ≥2. And we have found statistically significant differences between the group of patients with scores ≤1 and those with scores ≥2 (p=0.02). Hence, the location of the LMA may affect the incidence of complications.
This study had several limitations. The sample comprised only 124 patients recruited from a single center. Placebo-control saline was not used in the groups without muscle relaxants, although the observer was blinded to patient grouping. The BMI of our patients was 23.8±2.81 kg/m2, which is higher than normal. Body weight was used to determine the size of the LMA used in this study, which may have influenced the location of the LMA and the incidence of adverse events.21 Additional patients could be enrolled to increase the statistical power of the study.
In summary, the sniffing position and use of a muscle relaxant had no effects on placement of the LMA, the fiberoptic score or the ventilation parameters of the LMA. The use of muscle relaxants could reduce the rate of adverse events.
Acknowledgment
The authors would like to thank American Journal Experts (www.aje.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 27, 2019.
- Accepted June 2, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.