


Abstract
Objectives: To evaluate the attitudes of pregnant women towards different forms of labor pain relief, preferred methods of pain relief, and the effects of social media on their awareness and knowledge.
Methods: This was a cross-sectional study conducted between April and August 2017 in the Maternity and Children’s Hospital, Najran, Saudi Arabia. A total of 416 pregnant women were interviewed and analyzed using IBM Statistical Package for Social Sciences version 20 (IBM Corp, Armonk, NY, USA).
Results: A total of 62.7% were aware of labor pain. However, 58.7% of the total sample group was unaware of labor pain relief, and 79.8% of the total sample group was unaware of the different forms of labor pain relief available. Educational level was significantly associated with awareness and knowledge of labor pain relief (p=0.001). The majority of pregnant women obtained information from friends (57.5%); and only 16.1% of women received information from their health care providers.
Conclusion: Most of the pregnant women recruited into this study had insufficient awareness of labor pain and methods of pain relief. They acquired their information from their friends and families rather than from their health care providers.
Labor is the physiological process that is responsible for expelling conception products from the uterus when gestation is complete. However, regular uterine contractions and the descent of the fetus through the birth canal can cause very painful sensations. Labor pain originates from uterine contractions and takes the form of visceral pain innervated by the nerve between the tenth thoracic spinal cord segment and the first lumbar spinal cord segment (T10 to L1), while the descent of the fetus through the birth canal causes somatic pain innervated by the pudendal nerve. Labor pain is one of the most severe types of pain that a pregnant woman can face during her lifetime. There is no other circumstance in which an individual’s experience of untreated severe pain, amenable to safe intervention, is considered acceptable while under a physician’s care. In the absence of a medical contraindication, a maternal request is a sufficient medical indication for pain relief during labor.1 Therefore, it is important that pregnant women receive education and improve their knowledge of effective analgesia for childbirth to decrease the incidence of maternal request for cesarean section.
A study2 relating to women’s expectations and experiences of labor pain and relief during labor, notes that there was a difference between the expectations and actual experiences of women. A Cochrane review article presented the conclusion that continuous support during labor might improve outcomes for women and their infants; this review also suggested more encouragement for spontaneous vaginal birth, shorter labor durations and a reduced incidence of cesarean births. Further recommendations included a reduced incidence of instrumental vaginal birth, the use of analgesia, low 5-minute Apgar scores and fewer negative feelings about childbirth experiences.3 There are many of pharmacological methods used for labor pain relief such as epidural analgesia, injections, and inhalational agents.4 Many studies have addressed awareness of labor pain relief among pregnant women and identified a distinct lack of knowledge regarding pain relief during labor. For example, Poomalar et al5 studied the awareness of labor analgesia among women in antenatal clinics and found that 89.8% of women (out of a study population of 256) were not aware about the uses of pain relief during labor; furthermore, only 10.2% had some knowledge of pain relief during labor. In another study, Nabukenya et al6 evaluated the knowledge, attitudes, and use of labor analgesia among 1293 participants and discovered that only 7% were aware of labor analgesia. Ekweani and Avidime7 also studied the awareness and desirability of pain relief during labor among pregnant women and found that 56% were aware of labor analgesia. In another study, Karn et al8 found that the awareness and attitudes of women during the antenatal period towards pain during labor and its relieving agents during childbirth were relatively low in developing countries. The main difference between developed and developing countries is the presence of different forms of pain relief. For example, in the United Kingdom, 90% of obstetric units offer a 24-hour epidural service.9 However, in Poland, only 20% of hospitals offer a 24-hour epidural service.10 This disparity is due to insufficient facilities or the cost efficiency of the service itself. In Saudi Arabia, with the exception of governmental specialized hospitals and private hospitals, most governmental hospitals do not provide such services. This is due to a lack of services, a lack of medical staff and a high birth rate. In the Maternal and Children Hospital, Najran, Saudi Arabia there are approximately 7000 and 8000 deliveries per year. With a lack of medical staff, the specialized services such as epidural anesthesia, are not feasible.
There was a global variation in knowledge among pregnant women with regard to pain relief during labor. In the absence of pain relief, many women deliver their babies with extreme labor pain. This experience of pain is unnecessary because the experience is due to a lack of knowledge with regard to labor pain relief. In the present study, we investigated the awareness of different forms of labor pain among pregnant women in the Maternal and Children Hospital, Najran, Saudi Arabia their preferred methods of pain relief and the effects of social media on awareness and knowledge.
Methods
This study was a cross-sectional survey of pregnant women attending the Antenatal Clinic at the Department of Obstetrics and Gynecology at the Maternity and Children’s Hospital, Najran, Saudi Arabia and was carried out by direct interviews between medical staff and patients. The city is located in the Southwestern of Kingdom of Saudi Arabia. The Maternity and Children’s Hospital is a referral hospital for the Najran region, has 200 beds, and has a delivery rate of 7000 to 8000 births per year. The study was conducted between April and August 2017. Any pregnant women attending the hospital during this period and were provided verbal consent to participate in this study were included as subjects. The study was ethically approved by the Research Committee of the College of Medicine, Najran University, Najran, Saudi Arabia prior to patient recruitment, and all study data were kept confidential and anonymous. Prior to recruitment, we determined that our desired sample size was 384, assuming the use of simple random sampling techniques, a 3% marginal error, 95% confidence levels and that the awareness of pregnant women with regards to labor pain relief in a similar study was approximately 10%.11
The following formula was used to determine our desired sample size:
in which ‘z’ represents the confidence level set at 95% by convention, ‘p’ is the % of awareness in a similar study published previously (approximately 10%) and (1-p) represents the % of pregnant women who were not aware of labor pain.
Our calculations showed that our desired sample size was 384. However, our study included 416 women to increase the validity and reliability of the study. Data collection consisted of a structured questionnaire prepared in English by the researchers, which was then translated into Arabic. A pilot study was conducted to test the questionnaire before use in the final study. This test was carried out using 24 women who were not included in the main study and was used to evaluate the validity and reliability of our questionnaire. To test the reliability (internal consistency), we used the Kurder Richardson 20 (KR-20) index due to the dichotomous nature of the patient answers (‘Yes/No’ or ‘Don’t know’). For all domains, the KR-20 ranged from 0.68 for the labor pain relief method to 0.77 for labor pain awareness. Stability was tested using test-retest reliability, as measured by intraclass correlation coefficients (ICC), which ranged from 0.69 for labor pain relief methods to 0.83 for labor pain awareness. Content validity was evaluated by 2 different experts who reviewed all scale items. Any conflicts were resolved by discussion or voting, and any suggested modifications were considered. For construct validity, we used a simple correlation coefficient; all items were moderately correlated with overall score (convergent validity) and poorly correlated with other domain totals (discriminant validity). The correlation coefficients ranged from 0.31 to 0.69. The final questionnaire consisted of 2 parts. Part one focused on demographics and medical and obstetric variables, while part 2 focused on the awareness of labor pain and relief, the preferred method of labor pain relief and information sources. Data collectors received 2 days of training, and data were acquired from patients by the data collectors during direct interviews.
The dependent variables in our analysis were the awareness of pregnant women towards labor pain types, labor pain relief, the preferred method of labor pain relief and information source. The independent variables were the demographic, medical and obstetric characteristics (age, nationality, educational status, occupation, family size, medical history, parity, cesarean section, risk categories, family planning, antenatal care visit, family support and level of support). All data were entered into a Microsoft Excel datasheet and then analyzed using the Statistical Package for Social Sciences for Windows, version 20 (IBM Corp, Armonk, NY, USA).
Results
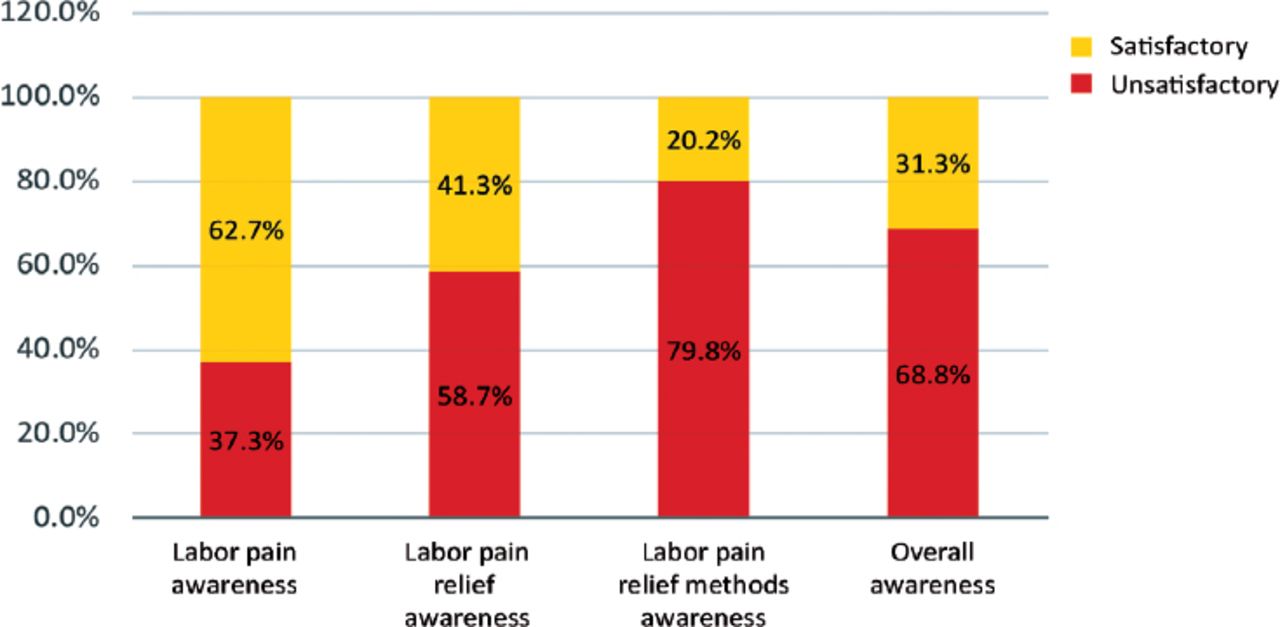
This study recruited 416 pregnant women. The levels of labor pain awareness within this study cohort are provided in Figure 1. Approximately 62.7% of women were aware of labor pain; however, approximately 58.7% of the women in this study were unaware of labor pain relief, and 79.8% of the women in this study were unaware of the methods available for labor pain relief. Thus, overall awareness of all domains was 31.3% for the study population. Sociodemographic data are shown in Table 1. Approximately 69% of the women fall within the 20-35-year age range, 37.8% of the women were educated at either the university or postgraduate level, and 78.8% were housewives.

The levels of labor pain awareness in pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
Sociodemographic characteristics of pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
The medical and obstetric histories of our patients are provided in Table 2. The majority of women were free of medical conditions, although 7% had been diagnosed with anemia. The data also showed that 33.7% had experienced one or more cesarean sections, 57% had visited multiple healthcare providers, and 51% had planned to become pregnant. In total, 87% of the women categorized themselves as low risk. In addition, 97% had family support, but of these, 2% were not satisfied with the level of support provided.
Medical and obstetric history of pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
The domains of labor pain, labor pain relief, and preferred methods of labor pain relief are shown in Table 3. First, in terms of awareness of labor pain, 62% of pregnant women claimed that they had satisfactory awareness of labor pain. Approximately 99% of women stated that they knew about labor pain; 72.4% (n=301) said that the support of the husband would reduce labor pain, while 77.6% (n=317) also thought that family support would help reduce pain. Further analysis showed that 77.4% (n=322) thought that medical and psychological disease, along with exhaustion, would increase labor pain and that 74.3% (n=309) were fearful of childbirth because of labor pain. Because 68.6% (n=212) of women had experienced a previous delivery, 64.1% (n=198) believed that labor pain was so severe that they could not tolerate it. Finally, 61.2% (n=189) of women indicated that the experiences of other women with labor pain led them to fear labor pain, while 48.4% (n=150) were unaware of pain relief for labor.
The dimensions of labor pain awareness in pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
In terms of awareness among pregnant women with regard to labor pain relief, we found that 66.3% (n=276) knew about different types of labor pain relief; 37.3% (n=155) knew of a form of pain relief that could be inhaled, 42.8% (n=178) knew about analgesic injections (intravenous and intramuscular), and 62% (n=258) knew about epidurals. Finally, 54.1% (n=225) believed that labor pain relief was effective, and 20% (n=83) thought that cesarean section was a good option to avoid labor pain.
With regard to the methods of labor pain relief, 60.8% (n=253) preferred labor pain relief; however, among pregnant women who did not show a preference for labor pain relief, approximately 85.9% (n=140) worried about the negative effects of labor pain relief on the mother and baby, 33% (n=54) believed that there was no benefit from labor pain relief, and 46.6% (n=76) said they wanted to try natural childbirth. Multiple stepwise logistic regression was performed using the four models provided in Table 4 to identify predictors of labor pain awareness among pregnant women.
Multiple stepwise logistic regression for predictors of labor pain awareness in pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
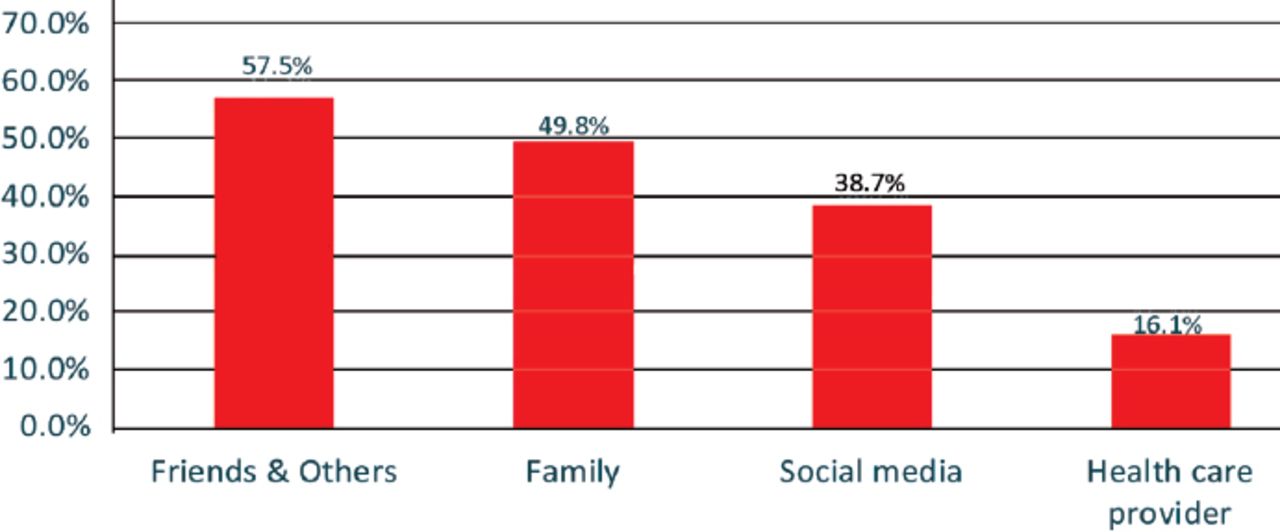
Data relating to the information source are provided in Figure 2. The majority of our study population acquired information from friends and other personal contacts (57.5%) and from family (49.8%); however, 38.7% claimed that they acquired such information from social media, and only 16.1% acquired information from a health care provider.

Source of knowledge regarding labor pain in pregnant women attending the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia in 2017.
Discussion
Labor pain is one of the most severe forms of pain that pregnant women can face during their lifetimes. In the present study, we investigated knowledge among pregnant women with regard to different types of labor pain relief to identify which types they preferred. Our study showed that 63% of women were aware of labor pain, 41% were aware of labor pain relief, and 20% were aware of labor pain relief methods. Previously, Nel et al12 reported that 56% of their cohort were unaware of pain relief,n while Hasan13 reported that 58% of women were not aware of labor pain. In other studies, 89% had no knowledge on the use of pain relief during labor, while 7% had at least some knowledge of labor analgesia.5,6 In another study, Naithani et al14 reported that 90% of women were unaware of labor analgesia. Compared with the populations in these previous studies, our population had good knowledge of labor pain relief. In our study, 72% of women believed that spousal and family support would help reduce labor pain. This is in contrast to a previous Saudi Arabian study by Al-Mandeel11 in which 182 women (45.3%) out of a study population of 402 preferred the presence of a companion during childbirth. Our findings and comparison to other studies show that labor pain relief is a significant factor for pregnant women during childbirth. Consequently, this reflects the importance of counseling pregnant women in terms of their awareness of labor pain types, pain relief, and selecting a preferred method of relief.
The fact that pregnant women have good knowledge about labor pain and pain relief shows that they will select a suitable method of labor pain relief. We found that 60% of pregnant women would prefer to use some form of labor pain relief. However, those who do not prefer to use pain relief appear to have misconceptions and misunderstandings with regard to labor pain relief. In fact, 86% of our study cohort believed that pain relief would have a negative effect on mother and baby. Another factor to consider is that 33% of pregnant women who do not show a preference for pain relief during labor also believed that such methods had no benefit. Furthermore, 46% of pregnant women wanted to try natural childbirth. Another study by Nel et al12 found that 56.7% of pregnant women would ask, or have asked, for pain relief during labor. Hazarika et al15 further reported that 98% of pregnant women believed that medications that reduce labor pain could be harmful, while Poomalar et al5 reported that 7.8% of women were against labor analgesia and that 7 out of 20 women who were against labor analgesia also thought that this practice might cause harm to the baby. Poomalar et al5 also reported that 8 out of 20 women did not believe that these treatments provided pain relief and noted that 5 out of 20 women wanted to experience natural childbirth. Nabukenya et al6 reported that 45% of women wanted to experience natural childbirth, while Prakash et al16 reported that 53.85% of those who did not want labor analgesia also wanted to experience natural childbirth.
This variation in the level of awareness of labor pain relief is influenced by a lack of knowledge. In our present study, the level of overall awareness was affected by the distribution of many factors, such as educational level, cesarean section history, medical history and parity. The educational level of women in our study, at either the graduate or postgraduate level, was high, at 37.8%. This high level of education is the likely cause of the clear awareness of labor pain relief within our study cohort. The number of participants with a higher level of education was 1.64 times higher than the number of participants with lower levels of education (OR; 95%CI:1.335-2.016, p=0.001). Our study showed that the educational level of graduates had a positive impact on their knowledge with regard to labor analgesia.6 Furthermore, Poomalar et al5 reported that approximately 32% of women in their study cohort were graduates. In another study, 23.2% of the study population were college graduates, and 0.7% were postgraduates.14 We also found that pregnant women who had experienced cesarean sections were less aware of labor pain relief. This is because these participants would not have experienced labor pain. Furthermore, pregnant women who had some a medical condition were more aware of labor pain than those without a medical condition. We also found that women with a higher parity were more aware of labor pain.
Most of the pregnant women in our study acquired information from friends (57%) and family (49%), but only 16% obtained information from their health care providers. In a similar study by Mugambe et al,12 55% of women acquired information from friends. In another study, 36.2% of women gained information from friends and relatives, and only 19% obtained information from their doctors.13 Nabukenya et al6 reported that 47% of their study cohort knew about labor analgesia and received this information from friends and family. Hence, the majority of pregnant women appear to acquire information from their friends and relatives. This leads us to consider the source of the information from these friends and relatives and whether this information is actually accurate.
Our study has some limitations that should be considered when interpreting our findings. First, our study only concerns one region in Saudi Arabia, and therefore, our data cannot be extrapolated across the rest of the country. A second, we cannot follow up patients after delivery to assess their attitudes to labor pain relief following education. Additional studies are now needed to investigate patient attitudes towards labor pain relief.
In conclusion, most of the pregnant women in our study showed lack of awareness on the methods that can be use to relieve labor pain. Moreover, most of our study cohort acquired relevant information from friends and family instead of their health care providers.
It is therefore recommended that pregnant women be educated with regard to labor pain relief methods by their health care providers or via the distribution of leaflets during antenatal care visits in primary health care centers or maternity hospitals. The establishment of educational clinics in maternity hospitals for women during pregnancy should increase the level of awareness and reduce the risk of incorrect information being passed on from social media or friends.
Acknowledgment
The author would like to thank his colleagues in the antenatal clinic of the Maternity and Children Hospital, Najran, Kingdom of Saudi Arabia for their assistance with this study. The author would also like to thank Escienta (www.escienta.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 26, 2019.
- Accepted August 20, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.