


Abstract
Objectives: To determine the rate of pediatric orthopedic clinic visits attributable to normal musculoskeletal (MSK) variations in children less than 12 years of age; to characterize the etiology and to characterize the etiology and management plan in this group in an attempt to identify areas that could be improved in pediatric orthopedic clinical practice.
Methods: The study was a retrospective evaluation of 2,321 consecutive patients who visited a private pediatric orthopedic specialty clinic in Jeddah, Saudi Arabia between 2011-2016. All consultations were recorded in accordance with the standard protocol via data record form.
Results: We identified 764 (32.9%) patients with normal variation of the lower limbs, age birth to 12 years old. No significant association between gender and normal variation was noticed. The following types of normal variation were registered: 189 (24.7 %) genu varus or valgus, 257 (33.6%) in-toe gait, and 318 (41.6%) flexible flat foot. Seven hundred and thirty-seven (96.5%) cases were normal variations, while only 27 cases (3.5%) were deemed pathological and required further treatment.
Conclusion: Normal variations represent the most common complaint in pediatric orthopedic private practice. Inappropriate referrals, useless follow-up visits, and excessive investigations were a common practice, overloading the health care system. None of the previous efforts made any notable improvement.
Normal variants refers to normal development of the musculoskeletal system, in particular, the lower limbs. It is important to know about them, as they are a common cause of concern for parents and a frequent reason for consultation. Normal variants include leg alignment issues, flat feet, high arch foot (cavus foot), knock-knees, bow-legs, out-toeing, in-toeing, toe-walking, curly toes, hypermobile knees, or having nocturnal limb pain in childhood. A reasonable description of normal is the mean value of the measurement +2SD.1 Generally, normal variation of the lower limbs, such as flexible flat foot; in-toeing; bow-legs, which will be the focus of our study, will resolve spontaneously, and there is little evidence that intervention changes the natural history; for that, reassuring the parents is the cornerstone of treatment. Investigation and intervention in the majority of these cases is not necessary, and is sometimes harmful to the child, exposing him/her to radiation and surgery, with all the side effects.1,2 Normal variants represent an important proportion of secondary care referrals, and many children referred to pediatric orthopedic clinics are normal and have no specific disease or deformity. Moalony et al2 reported that half of all new referrals to their pediatric orthopedic clinic were children with normal variants of lower limb development. This places undue pressure on these clinics’ resources,2,3 and within the large group of normal children with physiological variants, there is a small number with specific pathology, due to both focal and systemic processes, in which the deformity often progresses and usually requires treatment. Differentiating between the 2 forms is facilitated by a thorough understanding of the natural history of the development of MSK in children. These children should be identified, investigated, diagnosed, and treated appropriately.4 Referral is often unnecessary and may turn out to be harmful, leading to unnecessary interventions for the child. Many parents are not aware of the normal growth and development of lower extremity and desire normal alignment for their children; they are concerned and motivated to seek medical advice. Most parents are happy to be reassured that this childhood deformity is within normal limits and will disappear.5 Radiological and other investigations are not routinely required for children with normal variants of the lower limb, except to exclude a pathological process. Once recognized, a child with a normal variant does not require follow-up. Routine follow-up for a child with normal variation must be avoided, as it gives the impression that a child with a normal variant has an abnormality.6 It is, however, paramount that the treating clinician reassures and educates these children’s families.3
The objectives of this study were to determine the rate of pediatric orthopedic clinic visits attributable to normal variations in children ≤12 years of age, describe the demographic characteristics of this population, and characterize the etiology and management plan in children with normal variations in a private pediatric orthopedic specialty clinic in Jeddah, Saudi Arabia.
Methods
This a retrospective study of 2,321 patients who visited a private pediatric orthopedic clinic in Jeddah, Saudi Arabia during a 6-year period, between 2011 and 2016.
The data was collected from the patients’ files at the medical records department after developing the required ethical approval from the clinic authority. Inclusion criteria were 1) age ≤12 years, 2) musculoskeletal evaluation requested by the family, the patient or referral from another physician and 3) all Saudi and non-Saudi citizens were included. Children who did not have a diagnosis in their file or treatment plan were excluded from the study. Data were recorded in accordance with the standard protocol via data record form. The diagnosis and treatment plan was devised by a certified pediatric orthopedic surgeon.
Data entry and analysis were carried out using Statistical Package for Social Sciences (SPSS), version 25 (Armonk, NY: IBM Corp.). Frequency and percentage were used to describe categorical variables, whereas range, arithmetic mean and standard deviation were used to describe continuous variables. Chi-square test was applied to test for the association and/or difference between categorical variables; student’s t-test was applied to compare the mean of a continuous variable between 2 different groups, and p-value of 0.05 or less was applied for statistical significance.
Results
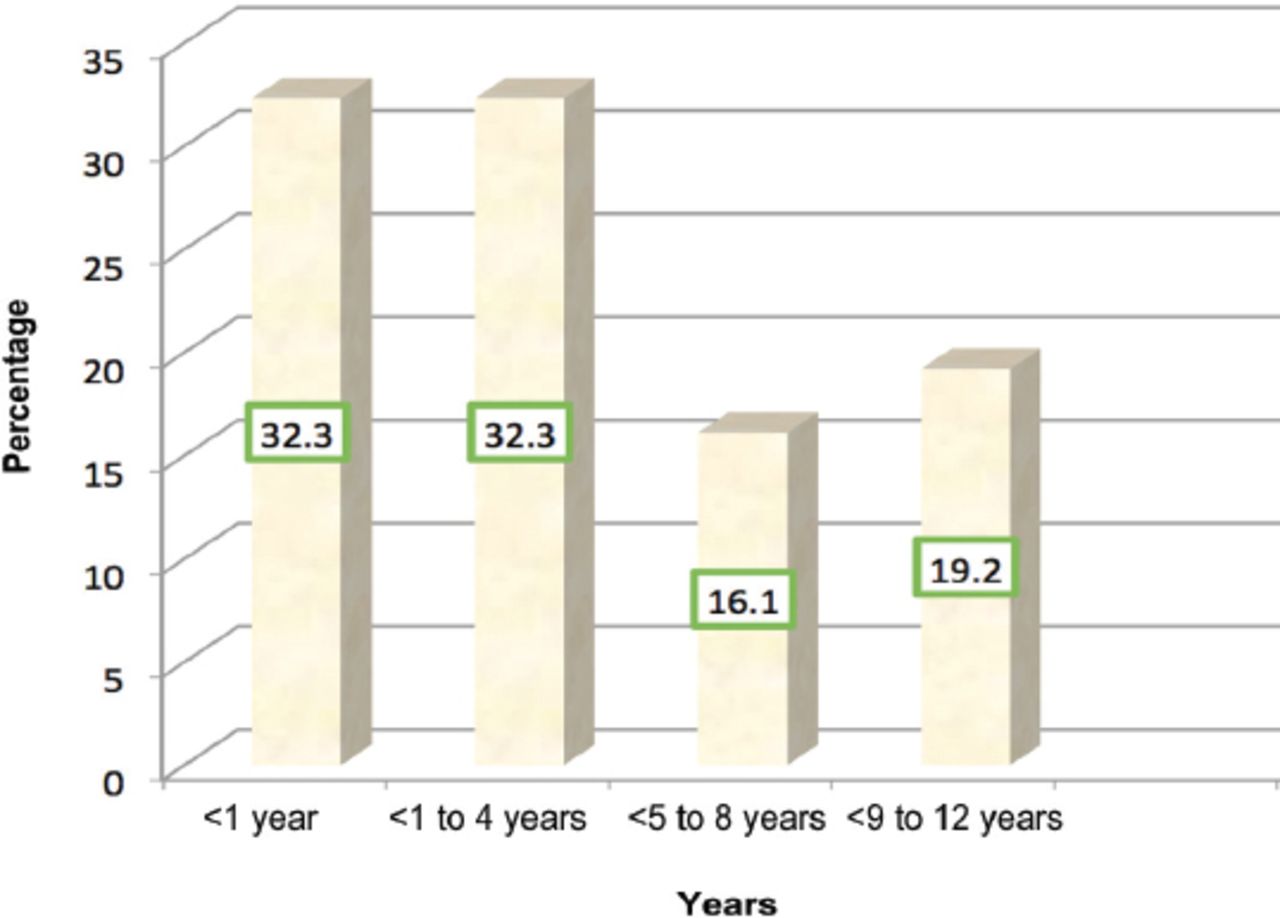
The prevalence of normal variation cases in our study was of 32.9% (764 of 2,321, confidence interval: 28.8-36). Most children (n=672 cases [88%]) were Saudis. The following epidemiological data were found: patients’ age at the first visit (mean ± SD) was 4.2 ± 3.6 years; 494 (64.6%) cases, representing two-thirds of all patients, were younger than 4 years at the first visit, while 123 (16.1%) were between 5-8 and 147 (19.2%) years were 9-12 years (Figure 1).
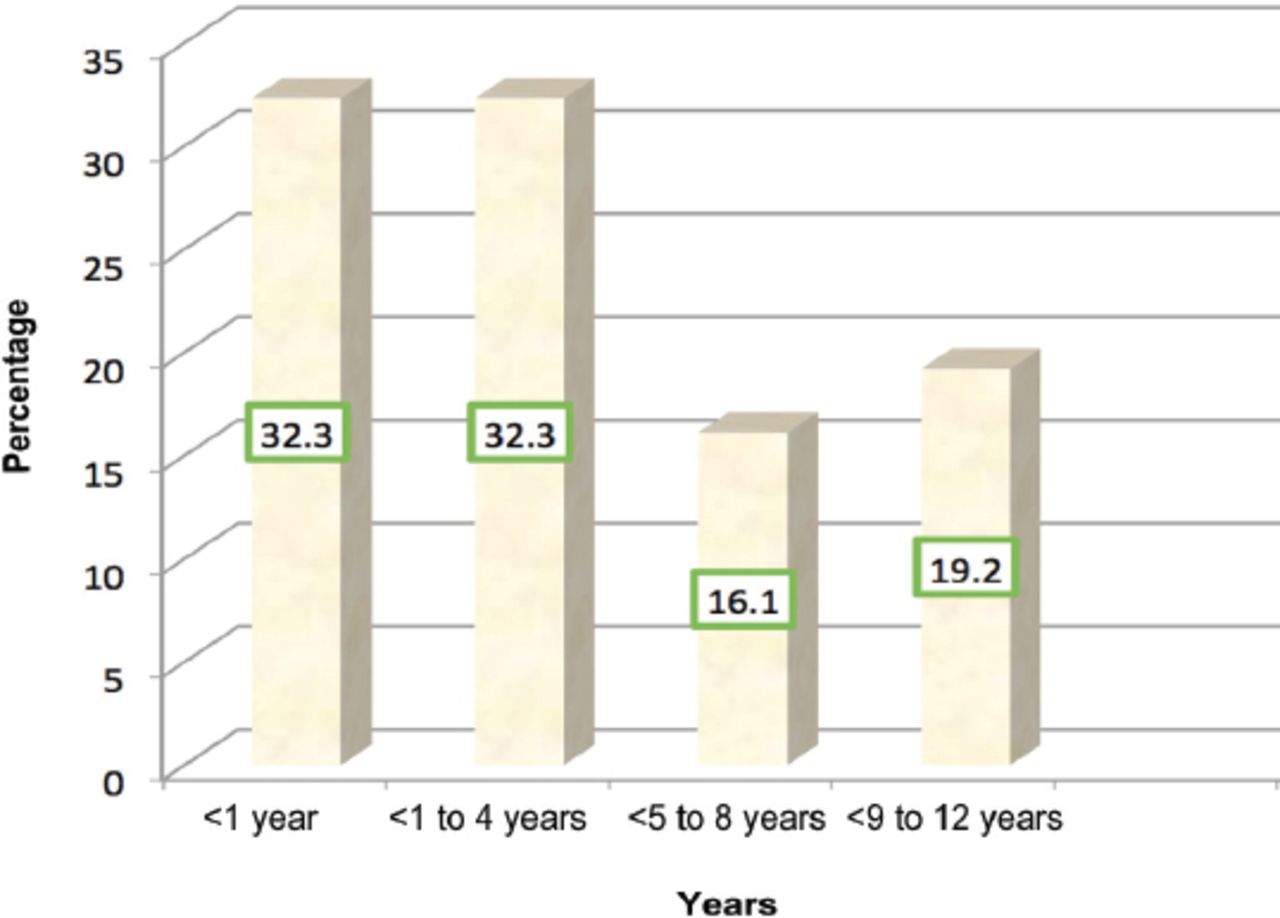
Percentages of age distribution of cases with musculoskeletal normal variations.
The average age of children at the first visit was different, depending on the type of normal variations: 2.3 years in children with knee varus and valgus, 3.8 for in-toeing and 5.9 years for flat foot. Table 1 shows that the average age of cases with normal variation (n=764) was significantly lower than the rest of the study population (n=1557)(p<0.001). We registered a gender rate of 0.69, with a slight predominance of girls. There was no significant association between gender and normal variation.
Association between patients’ gender and age, and musculoskeletal normal variations.
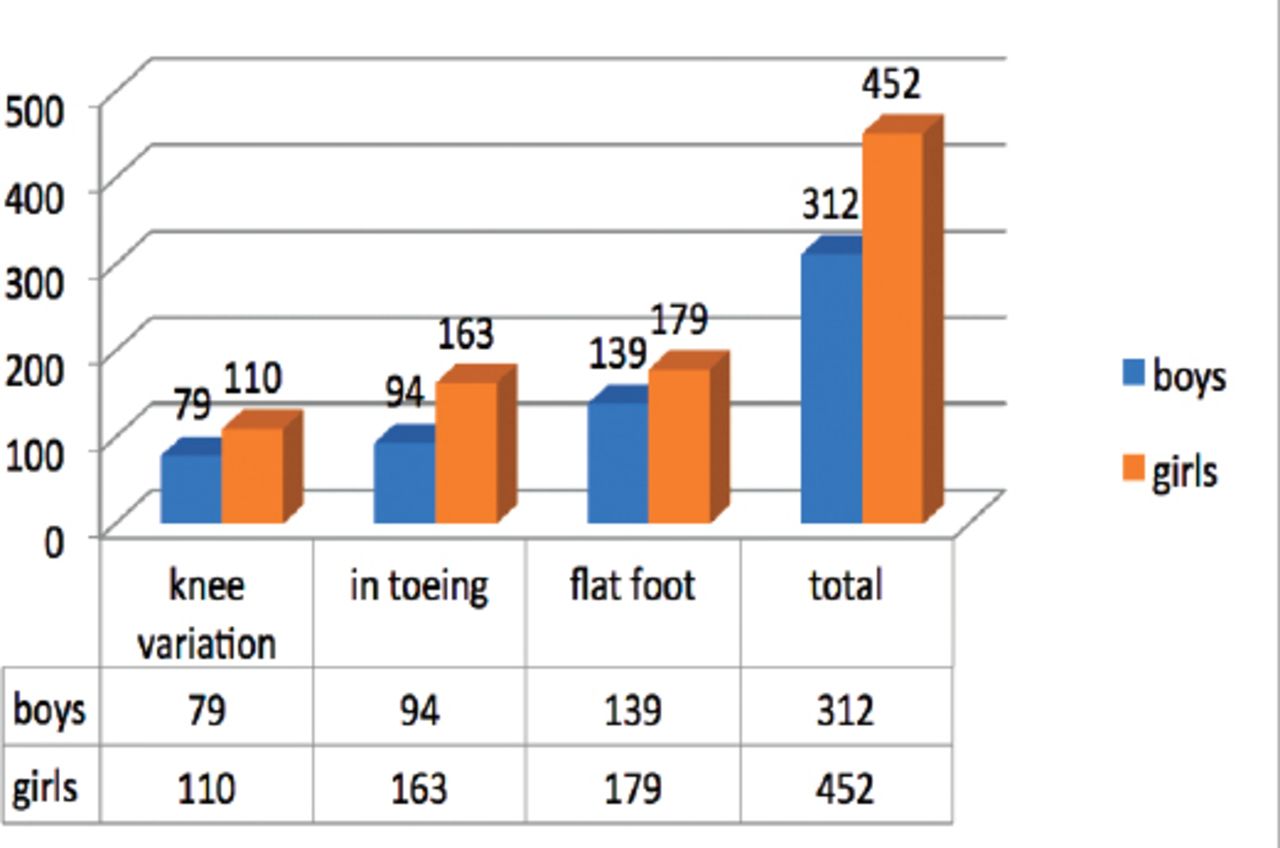
Figure 2 summarized the distribution of variation type by gender. Regarding the clinical symptoms or signs at the first visit or the reasons for referral for the whole study population, abnormal gait was the first presenting complaint in 740 (31.9%) cases, followed by pain secondary to trauma in 468 (20.2%) cases, foot deformity in 410 (17.7%) cases, and pain not due to trauma in 252 (10.9%) cases.
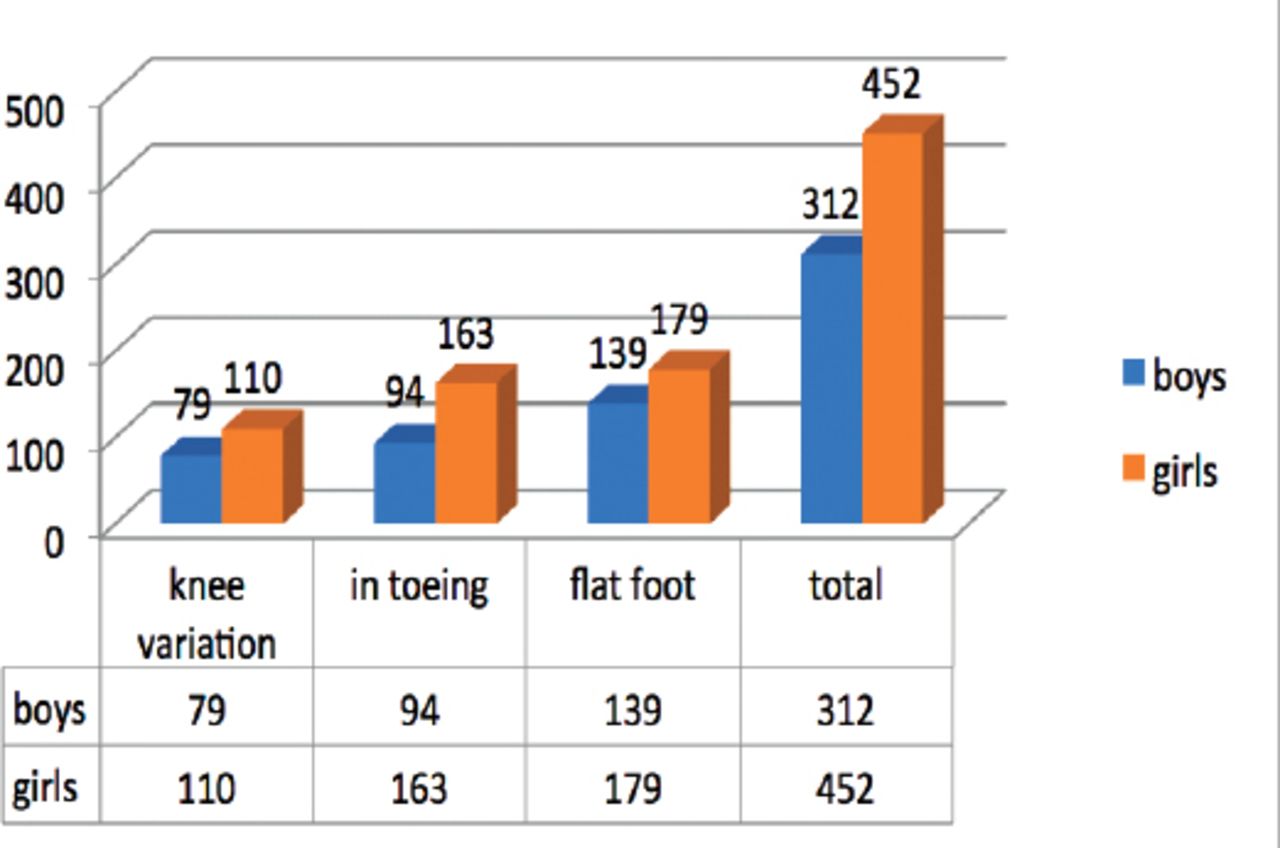
Distribution of musculoskeletal normal variations cases by gender.
X-ray test was requested at the first visit in 486 (63.6%) cases, as follows: in 248 (51%) cases for flat foot, in 175 (36%) cases for toeing gait, and in 63 (13%) cases for knee varus; in the rest of 278 (36.4%) cases, the x-ray test was considered as being not necessary and was not requested.
Regarding the final diagnosis, 737 (96.5%) patients were considered within the limits of the musculoskeletal normal variations (MSKNV) of the lower limbs at the first visit, and no treatment was needed. The following types of normal variation were registered: 178 (24.1%) knee varus or valgus, 250 (34%) in toe gait, and 309 (41.9%) flexible flat foot.
Of 764 cases with MSKNV, 27 (3.5%) proved to be pathological cases, with the following entities being identified (or diagnosed): knee varus (n=11), severe flexible flat foot (n=9), and in-toeing gait (n=7), representing 5.8% of the total cases of knee varus (n=189), 2.8% from total flat foot (n=318), and 2.7% from total in-toeing gait (n=257) diagnosed at the first visit on the whole group of studied patients (n=2321).
The treatment of pathological cases was a complex, using both conservative and/or surgical methods, with the therapeutic plan being established according to the type and severity of the disease, age and general status of the child and, of course, parents’ agreement and preferences. Three cases of pathological knee varus were treated conservatively by braces and improved without surgery. Eight cases required corrective osteotomy; half of them (4 cases) underwent surgery and improved, and the other half refused surgery and missed follow-up. Regarding pathological flexible flat foot, 9 cases required surgery, 4 cases underwent surgery (calcaneal osteotomy), and 5 cases refused the surgery. None of the in-toeing cases (n=7) accepted the surgical option (Figures 3 & 4).
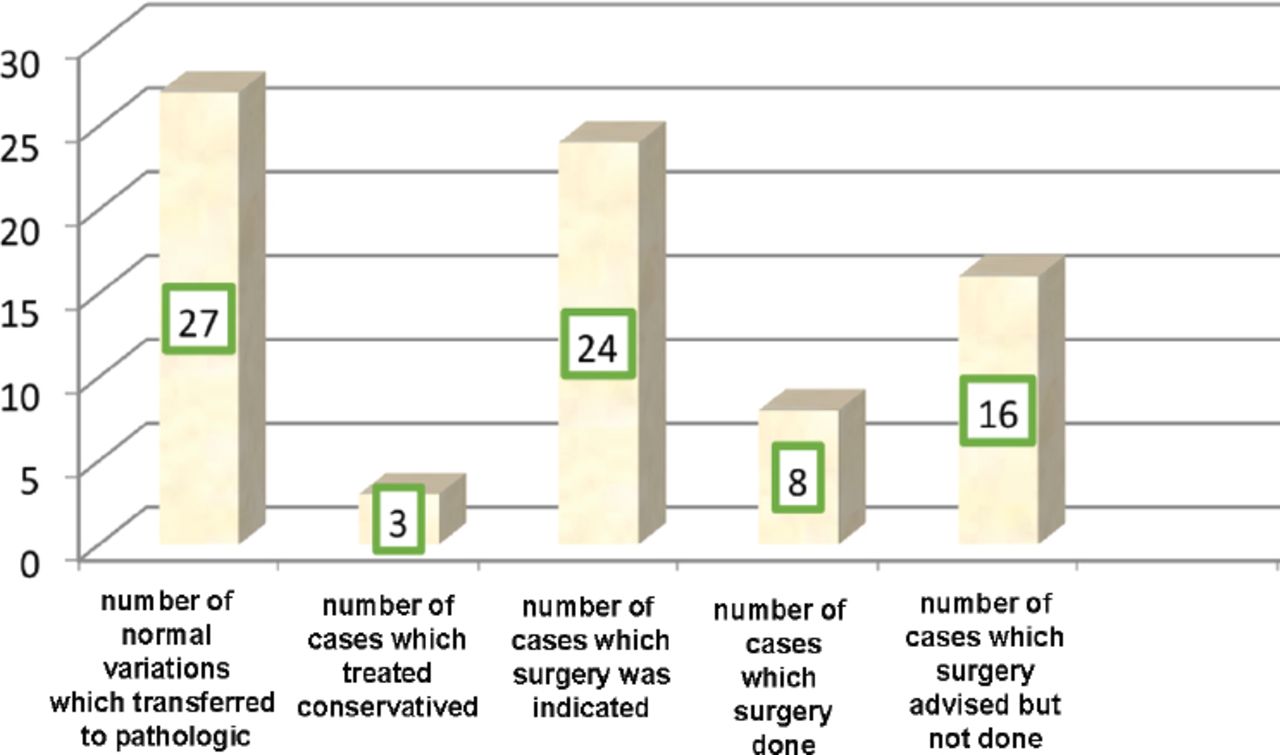
Pathological cases and treatment,
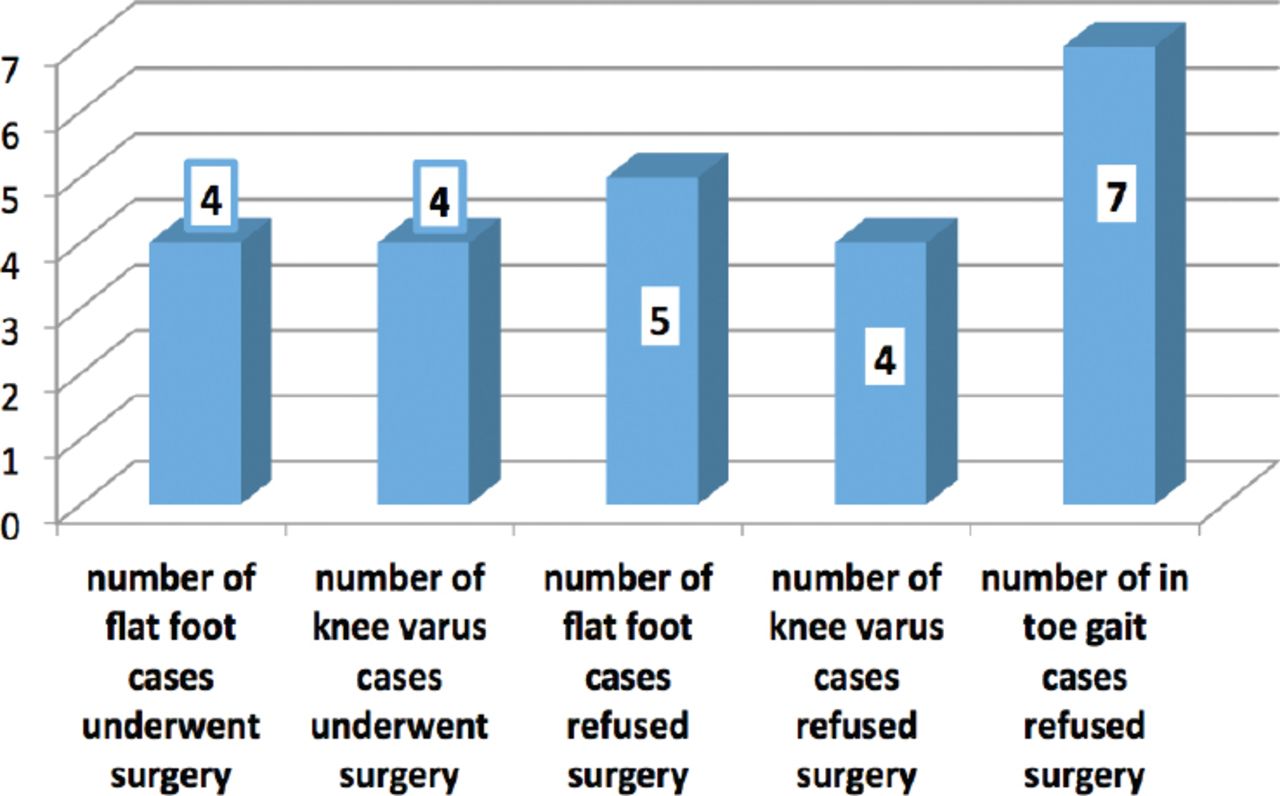
Pathological cases and surgical treatment.
Total visits number was 1083 including the first visit; 575 cases (75.3 %) showed once only in the first visit, 130 cases (17%) had 2 visits (first visit and one follow-up visit), while 59 cases (7.7%) were seen 3 times or more.
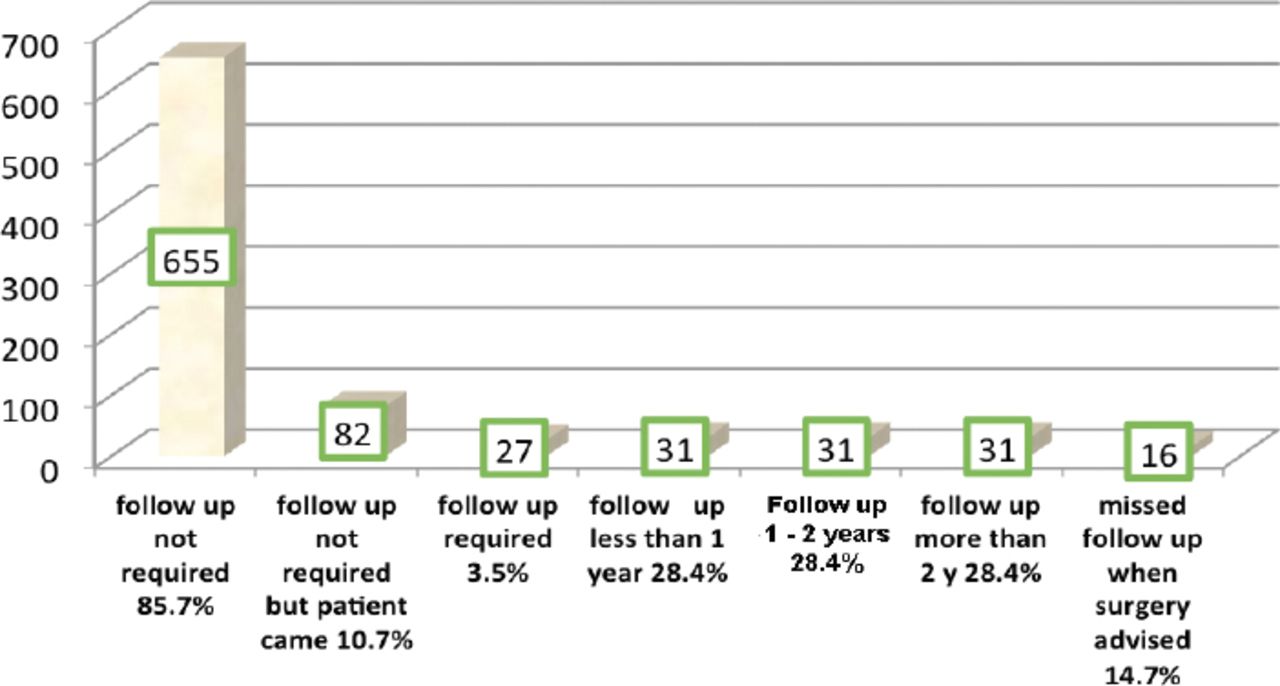
Regarding the follow-up requirement, most of the cases (n=655, 85.7%) did not require any follow-up, as they were within the limits of the musculoskeletal normal variations of the lower limbs. In 82 cases (10.7%), follow-up was not required, or the requirement was not mentioned in the patient files, and the patient came for further checkup. Follow up was requested, according to patients’ files, in only 27 cases (3.5%) that were pathological.
One-hundred and nine cases (14.3%) had actual follow up: 27 pathological cases and the 82 cases that came for follow-up without a clear requirement in the files. Those 109 cases made 428 visits, including their first visits; 16 pathological cases showed once only since they missed follow-up when surgery was advised. The remaining 93 cases, which included 11 pathological cases who continued follow-up and 82 within normal limits of the MSKNV and came for follow-up, made 412 visits, including their first visits. Of 62 cases with MSKNV from 82 cases seen in one follow-up visit within 2 years, 20 cases continued to have follow-up after more than 2 years, and even had more than one follow-up visit to be seen 2 to 3 times in follow-up. Of those patients seen in follow-up, 31 MSKNV cases continued follow-up for less than one year. The same number, 31 MSKNV cases, followed up for more than one year and less than 2 years, and in 31 cases (20 MSKNV, 11 pathological), the follow-up period was more than 2 years. The 11 pathological cases (7 cases knee varus, 4 cases flat foot) continued their follow up more than 2 years, with an average visit once every month during the first year of treatment, every other month in the second year, and 3 times a year after that. The maximum follow-up period was 6 years for knee varus patients who had corrective osteotomy. The remaining 16 pathological cases missed follow-up when surgery was advised (Figure 5).

Follow up period for musculoskeletal normal variations.
Discussion
Normal variants represent a significant proportion of secondary care referrals, and many children referred to pediatric orthopedic clinics are normal and have no specific disease or deformity. Demographic characteristics of the participants showed insignificant gender difference in children with normal variations. Both gender are affected equally; some studies showed that it is more common in females.7 The majority of cases (n=494, 64.6%) were younger than 4 years, representing two-thirds of all cases. The average age of presentation for in-toeing was 3.8, which is consistent with previous studies which showed that the maximum incidence age at presentation is mainly between 3 to 4 years of age. In cases of normal variations of the knee, usually from birth to 18 months of age, there is a normal physiological “varus” stage of development in which knee varus persists. From 24 months onward, children normally enter a stage of increasing valgus at the knees, and this generally persists until adolescence.8 In our study, the average age of knee varus condition was 2.3 years; in most literature, there is insignificance in gender distribution in knee varus,3 which is almost identical to our results.
Some report that the occurrence of flat feet is more prevalent in boys than girls;9 other studies reported a higher percentage among females than in males.10,11 The result of the current study was in between, there was insignificance in gender distribution in flat feet cases. There were 27 pathological cases of 764 (3.5%) in the general study population; only 11 cases of 189 (5.8%) of knee varus were pathological, which agrees with results of other studies.12 The most common form of pathological knee varus is Blount’s disease, which must be differentiated from physiologic knee varus.13-15 Variables such as walking age, race, weight, and gender have been suggested as risk factors for Blount’s disease. However, they have not been useful in differentiating between Blount’s pathology and physiologic knee varus.16,17 Seven cases of 257 (2.7%) of in-toeing were pathological and needed surgical correction. Our findings were in line with previous studies.18,19 Nine cases of 318 (2.8%) of flat foot did not resolve and did not improve during follow-up, required surgical intervention, and the findings were coherent with previous clinical reports.20,21
A high number of follow-up in our study could be because the treating clinician did not sufficiently reassure and educate the families of these children, or it may be required because the cases were suspicious and not clear as within the limits of the musculoskeletal normal variations of the lower limbs from the first presentation, which was determined in a follow-up visit. Another reason may be a common practice which could be called a regular review, as a practice in some clinics. Regular follow-up is detrimental, as it reinforces that the child with a normal variant has an abnormality.3 Routine follow-up for a child with normal variation must be avoided, as it serves to give the impression that the child with a normal variant has a pathological manifestation.
In addition, under-investigation may result in a missed or incorrect diagnosis, and over-investigation may upset the child, expose patients to excessive, unnecessary radiation, and result in misuse of resources.22,23 In our study, x-rays were requested in 63.6% of cases as delineated over the investigation. However, causes of over utilization of imaging were not identified and need further study; these reasons could include payment mechanisms in the private health care sector, treating physicians’ practice behavior, self-referral, defensive medicine, missed educational opportunities when inappropriate procedures are requested, and patient expectations.
Study limitations
The present study is a retrospective review and captured only cases of children with normal variations attending outpatient private orthopedic surgery clinic where the study was conducted. Parents had direct access to secondary health care, without visiting a primary health care provider first. In view of this noted shortcoming, the profile described here should be interpreted with caution.
In conclusion, normal variations represent the most common complaint in pediatric orthopedic private practice. Inappropriate referrals, useless follow-up visits, and excessive investigations were a common practice, overloading the health care system. None of the previous efforts made any notable improvement. Future studies are needed to explore barriers and solutions to address this problem in sub-specialized clinics.
Acknowledgment
We would like to thank Dr. Salah Fallatah, Associate Professor, Faculty of Medicine, Umm Al-Qura University, for his participation and support in editing of this manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 21, 2019.
- Accepted August 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.