


Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42844.
A 27-year-old male patient presented with generalized painless, non-pruritic skin rash. He had been diagnosed with metastatic germ cell tumor, for which he had undergone the first chemotherapy cycle consisting of cisplatin, etoposide, and bleomycin, one week prior to presentation. He had no history of alopecia and demonstrated no changes in the appearance of his nails, oral ulcers, or joint swelling. Moreover, he did not report any lifestyle change or travel or recent intake of mushroom. Physical examination revealed a rash involving the trunk and extremities, appearing as linear brown streaks with no erythema or excoriation marks (Figure 1).
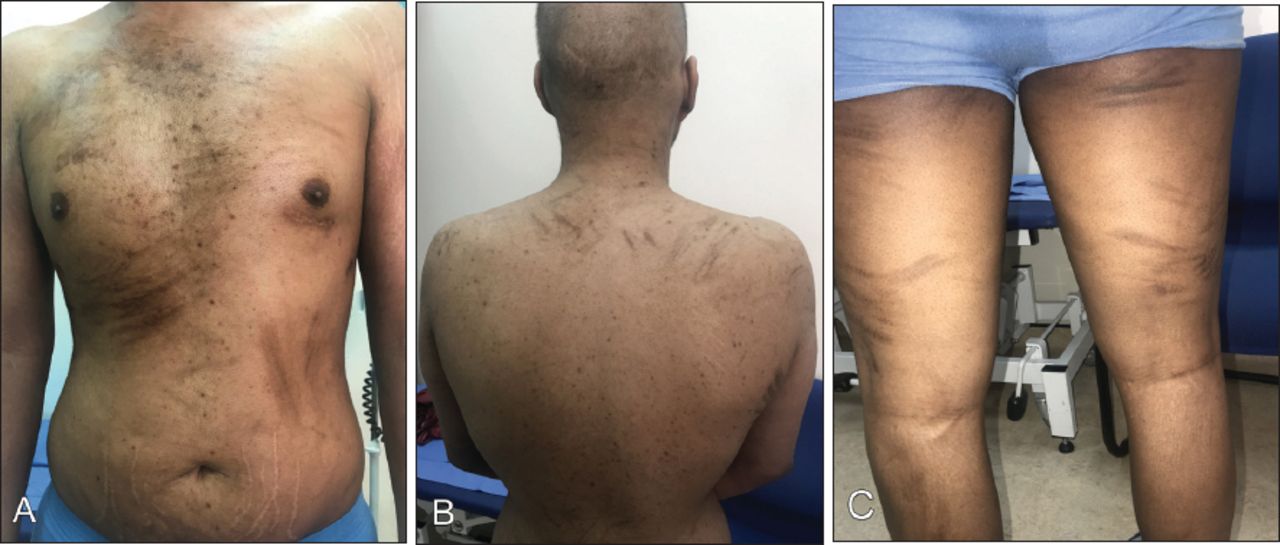
Multiple, brown patches in a linear configuration on A) the chest B) the back, and C) the lower limbs.
Question
What is the most likely diagnosis?
A. Contact dermatitis
B. Dermatitis artefecta
C. Flagellate hyperpigmentation
D. Shiitake dermatitis
Answer
C. Flagellate hyperpigmentation
Discussion
Based on the clinical presentation, a diagnosis of bleomycin-induced flagellate dermatitis was made. The patient required no treatment as he was completely asymptomatic, and the rash had started fading spontaneously. However, it flared up during the chemotherapy cycles. Given the classic appearance of the rash, biopsy was not needed.
Bleomycin, a glycopeptide, is an anti-neoplastic antibiotic that is generally used to treat various malignancies and to achieve chemical pleurodesis.1 The pulmonary adverse effects of bleomycin are well-established; however, its cutaneous manifestations are somewhat uncommon and vary among patients. Flagellate hyperpigmentation constitutes a unique cutaneous adverse effect of bleomycin, which has been reported to have an incidence of up to 10%; however, severe and widespread dissemination of the rash is rare.1 It is noteworthy that most cases of flagellate hyperpigmentation are associated with pruritus.2 However, it may also present as completely asymptomatic, as in our case.
Low bleomycin hydrolase levels in the skin and lungs are implicated as the basis of complications in these tissues. Moreover, minor skin trauma (namely from scratching) results in local bleomycin accumulation by increasing the cutaneous blood flow.1 Rash associated with shiitake dermatitis, which might be observed after ingesting raw or undercooked shiitake mushrooms, present with similar features.3 However, in the present case, the patient had no history of recent intake of shiitake mushrooms. Thus, this rare case of extensive non-pruritic rash following bleomycin administration was diagnosed as bleomycin-induced flagellate dermatitis based on the clinical characteristics.
Learning points
i) Flagellate hyperpigmentation constitutes a unique cutaneous adverse effect of bleomycin.ii) Although most cases of flagellate hyperpigmentation are associated with pruritus, it may also present as completely asymptomatic
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.