


Abstract
Objectives: To investigate the prognostic value of neutrophil-to-lymphocyte ratio (NLR) plus the lymphocyte-to-monocyte ratio (LMR) to predict survival outcomes in huge hepatocellular carcinoma (HCC) patients undergoing transarterial chemoembolization (TACE).
Methods: There were 180 huge HCC patients undergoing TACE between 2011 and 2017 were retrospectively analyzed. Patients who has an increased NLR (>3.94) and a decreased LMR (≤2.20) were assessed score 2 according to receiver operating characteristic (ROC) curve, and patients who were assigned with 1, with one of these characteristic or 0 with neither of these characteristics. We used univariate and multivariate analyses for evaluations of the predicative NLR, LMR and other values about overall survival (OS) using multivariate Cox’s regression.
Results: The liver function index such as aspartate transaminase, alanine transaminase, and total bilirubin, as well as inflammatory biomarkers like absolute neutrophil count, monocyte count, lymphocyte count, seemed much larger than the groups with an NLR-LMR score of 2 than in the other 2 groups (p<0.05 for all), including BCLC stage. Higher NLR plus a low level of LMR predicted a short median OS. Multivariate Cox’s regression revealed that an NLR-LMR score of 2 was a useful predictor of OS in huge HCC patients after TACE.
Conclusion: The pretreatment NLR plus LMR are effective for predicting survival outcomes in huge HCC patients after TACE.
As the sixth most frequent neoplasm as well as the third leading cause of cancer death worldwide, hepatocellular carcinoma (HCC) is one of the most common aggressive malignancies. Its incidence is expected to rise later.1 Huge HCC is defined as HCC with a nodule larger than 10 cm. Huge HCC is regularly combined with other prognostic factors such as macro/microvascular invasion or the presence of multiple tumors. Lots of treatments are not feasible, but transcatheter arterial chemoembolization (TACE) can improve the control of intrahepatic recurrence and prognosis.2,3 However, some patients with huge HCC gain benefits from TACE. Hence, differentiating the patients benefiting from TACE from patients not benefiting from it. Previous studies demonstrated that inflammation-based markers like the neutrophil-to-lymphocyte ratio (NLR), prognostic nutritional index (PNI), LMR and albumin-bilirubin grade (ALBI) do a good job in the progress of cancer in patients with HCC.4-7 Chu et al8 reported that the pretreatment NLR and PNI are convenient and helpful forecasters of overall survival (OS) in HCC patients after RFA therapy. Combining NLR and PLR was validated to predict recurrence and prediction of HCC in patients undergoing RFA.9 Recently, studies proved that LMR is a superior predictor of OS than established biomarkers.10,11 A high NLR was related to bad prognosis in patients with HCC underwent TACE.12 On the other hand, a high preoperative LMR predicted a favorable OS and progress-free survival (PFS).11 Yang et al10 showed that the LMR and NLR were useful inflammation-based forecasters in predicting of tumor recurrence in HCC patients undergoing hepatic resection. Recently, the combination of the NLR and the LMR for patients with HCC after TACE has not been developed. This study aim to determine whether a combination of NLR and LMR can help predict the outcomes of TACE-treated patients with huge HCC.
Methods
Between January 2011 and May 2017, 180 patients with huge HCC experiencing TACE in our hospital have been retrospectively included. This study was approved by the institutional review board (IRB) of The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China and was conducted according to the principles expressed in the Declaration of Helsinki and informed consent was obtained from all participants before TACE.
All patients with primary HCC according to the American Association for the Study of Liver Diseases (AASLD) guidelines,13 and TACE was recommended as the best treatment by a multidisciplinary team for patients not eligible for other treatments including aggressive surgery, liver transplantation, and tumor ablation. They must meet the requirements: i) nodules with a diameter larger than 10 cm. ii) no other simultaneous malignancies, and an iii) Eastern Cooperative Oncology Group (ECOG) Performance Status score of 0 or 1. They should not have any of the below symptoms: severe dysfunction of the lung, heart, kidney, and so forth; coagulation abnormity; acute inflammatory phase; and active concomitant infection. Patients who received percutaneous ablation, particle implantation, partial liver resection or other therapies before or after TACE treatment were excluded from this study as well.
Transcatheter arterial chemoembolization procedure
After a successful Seldinger puncture in the right groin, a 5-F introducer sheath was positioned. Selective catheterization of the target artery has been used to determine the supply of blood for tumors. Then, super selective catheterization of the feeding arteries was achieved using a microcatheter (Merit Maestro, Merit Medical System, Inc., USA). Subsequently, a mixture of ethiodized oil with pirarubicin (THP, 20-40 mg, Jiangsu, China) was administered as a chemoembolic material to occlude the feeding arteries of the tumor. The embolization endpoint was the stasis of blood flow; when this was not achieved, gelatin sponges were injected to obtain complete stasis. All the procedures in this study will be recorded.
Follow-up
Thirty days later after the experiment, participants were followed up by blood testing and imageological examination of contrast enhanced CT or enhanced MRI, with the aim of evaluating the tumor reaction and to decide individual treatment plans. Three months later, CT or MRI was carried out once more to judge tumor progression after TACE procedure. The number of treatments ranged from one to many based on multiple factors including the health of the patient, hepatic capacity, tumor reappearance and other blood testing. The data of participants were recorded until death occurred or the cutoff date (October 31, 2018). The endpoints of the study were tumor recurrence at 3 months after the first TACE procedure. The modified Response Evaluation Criteria in Solid Tumors (mRECIST)14 has been used to evaluate patients’ reaction after receiving the treatment. The OS time ranged from the first TACE to the death. Progression-free survival (PFS) refers to the time from the first TACE to that of disease progression or death.
Data collection and evaluation
One to 3 days before the TACE, blood testing were taken. Neutrophil-to-lymphocyte ratio has been considered as the total neutrophil calculation under the standard of lymphocyte calculation. Moreover, LMR has been assessed based on divided lymphocyte count and monocyte count. The ideal cutoff of NLR and PLR values were derived from the curve analysis of receiver operating characteristic (ROC).
Statistical analysis
The optimum preoperative NLR and LMR cutoff values were derived from a ROC curve. Mean ± standard deviation is used to present continuous variables and one-way analysis were compared between participants. Pearson x2 test or Fisher’s exact test were utilized to categorize data expressed as frequencies or proportions. The OS was obtained with the method of the Kaplan-Meier, and OS times were calculated by the test of log-rank. The factors of various dangers for OS have been figured out with multivariate Cox’s proportional hazard regression analysis. A p<0.05 displayed the significance of the statistics. Every analysis of statistics was finished by IBM SPSS Statistics for Windows, version 10 (IBM Corp., Armonk, NY., USA).
Results
Optimal cutoff values for the NLR and the LMR
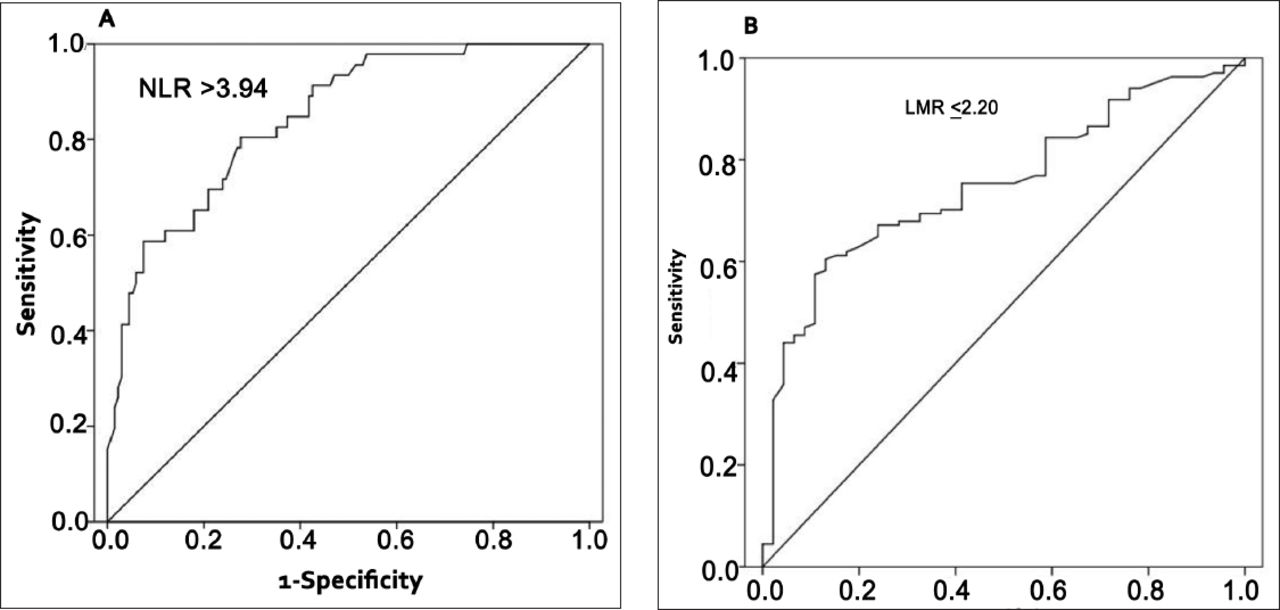
Tumor progression was assessed 3 months after the first TACE procedure, and we stratified each prognostic index based on the peak and cutoff points of ROC curve. Neutrophil-to-lymphocyte ratio ideal cutoff value should be 3.94 whose sensitivity was 0.804 and a specificity of 0.724 (AUROC curve: 0.845; 95% CI: 0.782-0.907; p<0.001) (Figure 1A). The ideal cutoff value for the LMR was 2.20 whose sensitivity was 0.604 and specificity 0.87 (AUROC curve: 0.751; 95%: 0.676-0.825; p<0.001) (Figure 1B). The purposes is to estimate the score of NLR-LMR individually using these values. Accordingly, the patients belong to 3 groups exhibited in Table 1.

Receiver operating characteristics curves to assess the best cutoff value of the neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) . A) receiver operating characteristic (ROC) curve of the NLR. B) ROC curve of the LMR.
The combination of the neutrophil-to-lymphocyte ratio (NLR) and the lymphocyte-to-monocyte ratio (LMR) as prognostic indices.
Baseline characteristics
The study group included 155 male and 25 female with an average age of 54.3 ± 9.3 years. The average size of tumors was 12.1 ± 1.9 (range 10.0-18.8 cm), and 103 (57.2%) patients had portal vein thrombosis. Overall, the mean TACE treatments times was 2.43 ± 1.13 (range: 1-7).
Associations between NLR-LMR grade and clinicopathologic characteristics of the HCC patients
Among the 180 included patients, 82 (45.6%) patients were assigned to the NLR-LMR 0 group, 29 (16.1%) patients were assigned to the NLR-LMR 1 group, and 69 (38.3%) patients were assigned to the NLR-LMR 2 group. These 3 groups did not show great differences regarding their genders, ages, and the sizes of tumors. The hepatic function, inflammatory biomarkers and BCLC stage were considerably elevated in the NLR-LMR group 2 than that of groups 1 or 3 (p<0.05 for all). Detailed information of the 3 groups are summarize in Table 2.
A comparison of the clinical characteristics of patients with different NLR-LMR scores.
Survival analysis
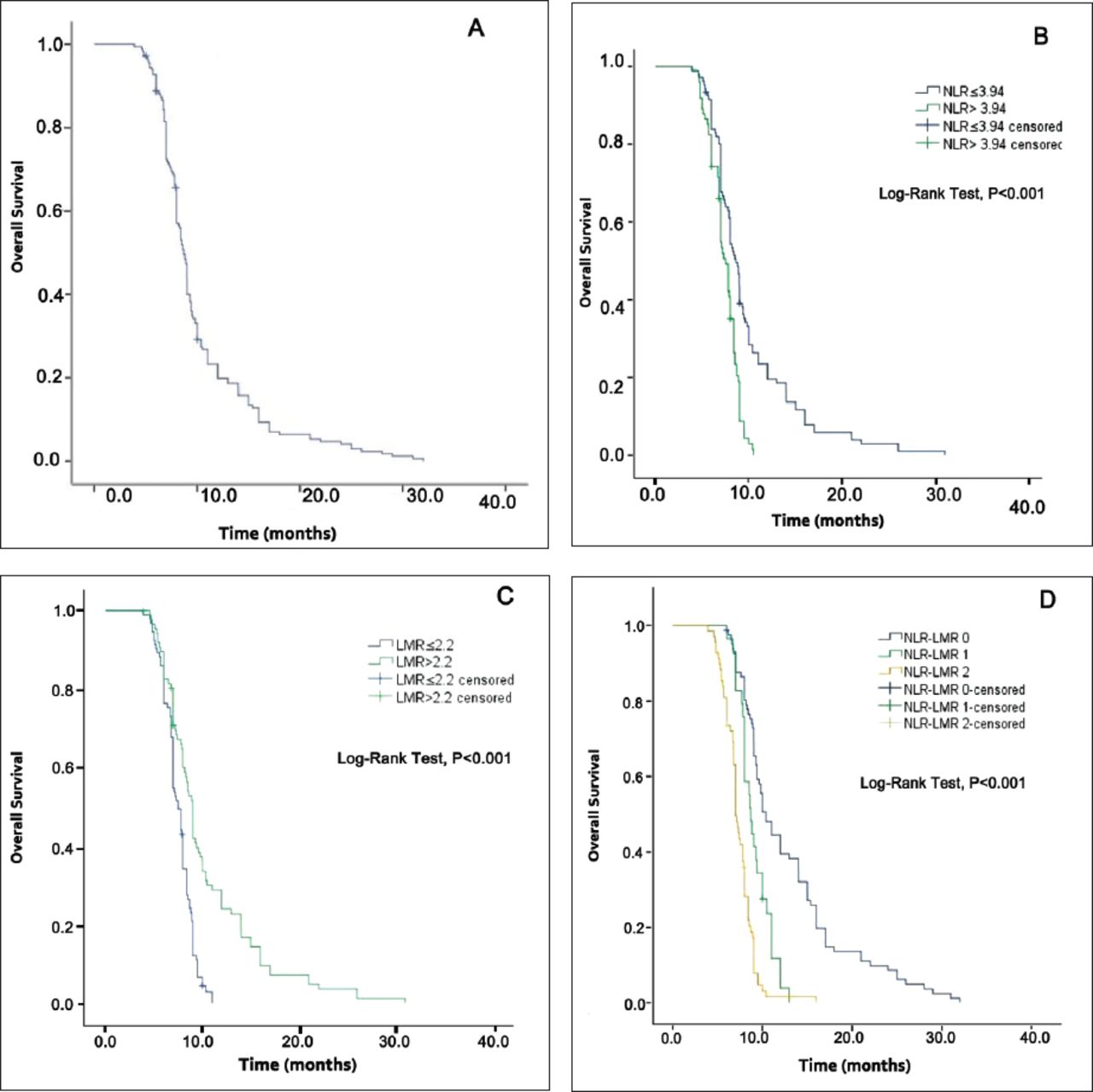
Among the patients, a total of 175 (97.2%) has been dead during the recording period. And the median OS has been 8.7 months (range, 3.9-32 months). Using the Kaplan-Meier analysis, it has been found that median OS for participants (NLR ≤3.94) was longer than that for participants (NLR >3.94) (8.6 months versus 7.5 months, p<0.001) (Figure 2B). The higher the NLR was, the lower the OS for patients would be. Likewise, median OS for participants with an LMR >2.2 has been registered higher than that for participants whose LMR was lower (Figure 2C). The higher the LMR was, the longer the OS in huge HCC patients after TACE treatment. Finally, patients with NLR-LMR scores of 2 had the worst outcomes as their median OS was only 7.0 months, compared with participants in the NLR-LMR 1 (median OS 8.7 months) and NLR-LMR 0 (median OS 10.4 months) groups (p<0.05) (Figure 2D).

Kaplan-Meier survival curves for overall survival in huge hepatocellular carcinoma patients who underwent transarterial chemoembolization. A) overall survival, B) the neutrophil-to-lymphocyte ratio (NLR), C) the lymphocyte-to-monocyte ratio (LRM) and D) the NLR-LMR score.
Risk factors for outcome after TACE
As shown in Table 3, tumor size, Child-pugh stage, PVTT, NLR, LMR, NLR-LMR score, and BCLC stage have much to do with a short OS. In addition, factors below can predict OS independently using multivariate analysis of Cox’s regression: Child-Pugh stage (p<0.001), tumor size (p=0.006), and an NLR-LMR score of 2 (p=0.014).
Prognostic factors related to overall survival (OS) .
Discussion
The NLR has been demonstrated as a prognostic serum biomarker for many malignancies.15-17 Larger HCC is often associated with a high NLR.18 Neutrophil-to-lymphocyte ratio cutoff values vary between different medical centers and different populations, so there is no optimal NLR for all patients.9,12,19 In this case, the best NLR cutoff value suitable for huge HCC patients were selected by ROC curve analysis. In this study, participants whose NLR is larger than 3.94 showed a considerably poorer OS than the others. These results were coincident in former findings, in which a high preoperative NLR had something to do with shorter OS in patients after TACE treatment for unresectable HCC.6,20 Lymphocytes are essential parts of human immune system. Fewer lymphocytes indicates an aberrant protected mechanism and a weakening in body immunity. For this reason, elevated levels of neutrophils or decreased levels of lymphocytes lead to an increased NLR and thus a worse prognosis in cancer patients. The LMR as a novel prognostic indicator has been proven to helpful to forecast the therapeutic effects for participant with HCC when experiencing the surgical resection.11 Additionally, there is no unified, standard optimal cutoff value for the LMR. The curve analysis of ROC was applied in order to examine the ideal LMR cutoff value in this research. It has been mentioned that those with NLR >2.2 displayed OS of longer time than those having LMR ≤2.2 in terms of univariate analysis. These results shared some similarities with what have been found before, in which a high preoperative LMR score was related to long OS in HCC patients.11,21 The mechanism by which a decreased LMR indicates short survival time is not very clear, but some studies have provided some possible interpretations. Lymphocytes and monocytes are the fundamental constituents of human antitumor immunity. However, monocytosis weakens the antitumor functioning of the system of immunity and promotes how the tumors come up and develop.22 Hence, a decreased LMR reflects the impairment of host immune surveillance. In our study, we found that a high preoperative NLR and a low LMR (NLR-LMR 2) were closely related to some factors: a high AST level, high ALT level, high total bilirubin (TBIL) concentration, elevated neutrophil count, elevated monocyte count, decreased lymphocyte count, portal vein tumor thrombus (PVTT), large tumor as well as a late BCLC stage. The predictive NLR-LMR value for huge HCC participants who underwent TACE was confirmed. A high NLR-LMR score were related to a short OS in patients with HCC. These findings are in accordance with the results of an accumulating number of studies.8,10,21 In combined with the results of this study, huge HCC patients may benefit from the preoperative NLR-LMR score as a valuable prognostic indicator in the near future. Some undeniable restricts are shown in this research. To begin with, the nature of the study is retrospective, and there may have been selective bias in data selection and analysis. Second, the number of patients is not much. Therefore, it is urgent to carry out prospective multicenter studies to prove the forecast value of the NLR plus LMR.
In conclusion, our single-center study revealed that pretreatment NLR-LMR score was important to predict OS patients with huge HCC receiving TACE treatment. The NLR-LMR score can be a new inflammatory biomarker for predicting the outcomes of participants whose HCC was huge with TACE.
Acknowledgment
We would like to thanks the American Journal Experts for English editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 31, 2019.
- Accepted January 6, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.