


Abstract
Objectives: To assess bone mineral density (BMD) of children with short stature using quantitative ultrasound (QUS) and compare it to children with normal height.
Methods: We conducted a descriptive, cross-sectional controlled study between May 2018 and February 2019 at various pediatric clinics in Jeddah, Saudi Arabia. In total, 219 children were included: 100 had short stature, and 119 were of normal height. Data were collected from one-on-one interviews, and BMD was measured using quantitative ultrasound.
Results: Children with short stature had significantly lower BMD z-scores than children with normal height (p<0.05). The use of vitamin D supplements was related to higher BMD z-scores in children with short stature (p<0.05). A significant association was found between higher BMD z-scores, and both age (p=0.05) and height (p=0.02). Through a further division of children with short stature into those with and those without growth hormone deficiencies, we show that growth hormone deficiency was positively associated with lower BMD z-scores; however, the p-value was 0.06.
Conclusions: Compared with children of normal height, those with short stature had lower BMD. Height, vitamin D supplementation, and age were all significantly correlated with higher BMD, while growth hormone deficiency was correlated with lower BMD.
Bone health is determined by many anthropological and physiological factors. These factors, especially those among children, have been of interest in many researchers during the past decade because of their effects on bone health impact health status in both child- and adult-hood.1-3 Normal height is among the factors that show a good correlation with higher bone-mineral density (BMD), whereas short stature is correlated with low BMD even in children with familial short stature.3 There are multiple ways to assess BMD; however, dual-energy x-ray absorptiometry (DXA) is the most common.4,5 Although DXA is precise and reliable for assessing BMD, it is also expensive and involves a small amount of radiation.4 An emerging approach for measuring BMD uses quantitative ultrasound (QUS) for screening patients at risk for osteoporosis. Quantitative ultrasound uses high-frequency sound waves to evaluate bone quality. It operates by determining the speed of sound waves regulated by multiple factors, including height, pubertal status, bone architecture, and soft tissue thickness.6 Quantitative ultrasound can be used on the distal radius, tibial shaft, calcaneus, and patella. Given its accessibility, affordability, portability, and immediate results, QUS is easier to apply on a wide scale than that of other BMD measuring techniques.6
In this study, we assessed the BMD of children with short stature using QUS, and compared them to children with normal height. Furthermore, we also analyzed additional factors associated with both low and high BMD.
Methods
We performed a descriptive, cross-sectional study between May 2018 and February 2019 at various pediatric clinics in Jeddah, Saudi Arabia. Before the commencement of this study, ethical approval was obtained from the research ethical committee at King Abdulaziz University and all procedures were conducted in compliance with the Declaration of Helsinki. Written-informed consent was obtained from the parents or guardians of the children. A private room was prepared at the pediatric clinics to interview the patients in the company of their parents or legal guardians.
All children with normal height and those with short stature (defined as a height minus 2 standard deviations from the mean height) of the same age and gender were recruited for the study. After getting their verbal consent to participate, data were collected by interviewing all children and their parents or guardians regarding modifiable factors known to affect BMD, including sun exposure, physical activity, daily milk consumption, dairy product consumption, vitamin D supplementation, consumption of formula milk during the first 2 years of life, and all medications actively used by the participant. Height and anthropometric measurements were performed, and BMD was assessed using QUS. The results were collected as z-scores and were explained to the participant’ parents/guardians.
Only children between the ages of 2 and 18 years were included in this study. The short stature group included children with different causes of short stature, including growth hormone (GH) deficiency (characterized by the inadequate secretion of GH from the anterior pituitary gland), low GH peak levels (<10 ng/mL after stimulation),7 familial short stature (defined as bone-age appropriate for chronologic age, normal growth, and predicted adult height appropriate for the familial pattern),8 idiopathic short stature (defined as having no identifiable disorder of the GH/insulin-like growth factor axis and no other endocrine, genetic, or organ system disorder),9 hypothyroidism (defined as thyroid-stimulating hormone concentrations above the reference range and free thyroxine concentrations below the reference range),10 and girls with early puberty (attributable to gonadotropin-releasing hormone (GnRH) agonist). All children had their Tanner stage measured by their parent using a Tanner stage graph provided by the clinic.
The exclusion criteria comprised the presence of metabolic disorders, chronic medical diseases, inflammatory bowel disease, diabetes, and congenital adrenal hyperplasia. Additionally, children who were not able to provide consistent results throughout the QUS screening were excluded. In total, 400 of 500 recruited children were accepted and participated in our study. However, 181 children were removed after applying our exclusion criteria, leaving a total of 219 participants in our study. We divided the cohort into 2 groups, those with short stature (n=100) and those with normal height (n=119).
Data entry and statistical analysis was performed using IBM Statistical Package for Social Sciences version 24 (IBM Corp, Armonk, NY, USA). Categorical variables were expressed either in frequency or in proportion. Continuous variables were expressed in range, mean, and standard deviation. Descriptive analysis and frequency assessments were carried out to display the characteristics of the sample such as: age, height, weight, and gender. The relationship between mean BMD z-scores and each categorical variable (gender, Tanner stage, short stature) was assessed using one-way analysis of variance (ANOVA). The relationship between mean BMD z-scores and other continuing variables was studied using Pearson’s bivariate correlation, which was used to determine the presence or absence of a significant correlation. Calculated p-values less than 0.05 were interpreted to be significant.
Results
The gender distribution of the children in both groups was almost equal, with the normal height group comprised of 63% females and the short stature group comprising 55% males (Table 1). The mean ages for the normal height group was 9.4 and the short stature group was 10.4 years. The mean BMD measurements for the normal height group was -1.51 and the short stature group was -1.56. The mean height for the short stature group was 126 cm (standard deviation: -2 to -6.4 cm), while that for the normal height group was 129 cm (standard deviation: -1.8 to 2.6 cm).
Descriptive statistics.
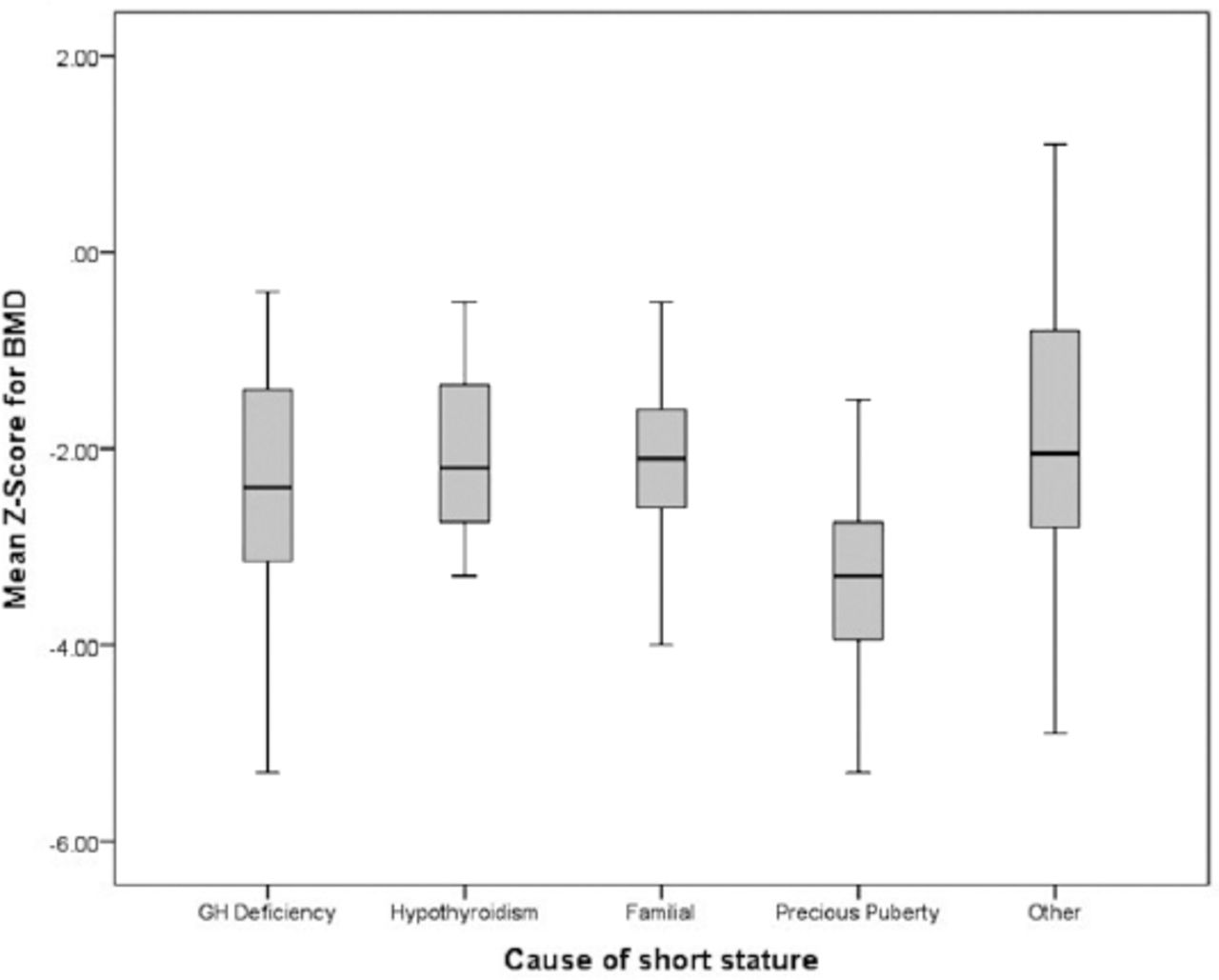
A significant association was found between short stature and lower BMD (p=0.000). Furthermore, the use of vitamin D supplementation was common to those with short stature and showed a significant correlation with higher BMD z-scores when compared to those not taking the supplements (p=0.000). Additional analyses of the short stature group revealed a positive association between higher BMD z-scores and both older age (p=0.05) and taller height (p=0.02). Children with short stature due to GH deficiency showed an association between GH deficiency and lower BMD z-scores when compared to those resulting from other causes; however, the p-value was 0.06 (Figure 1).
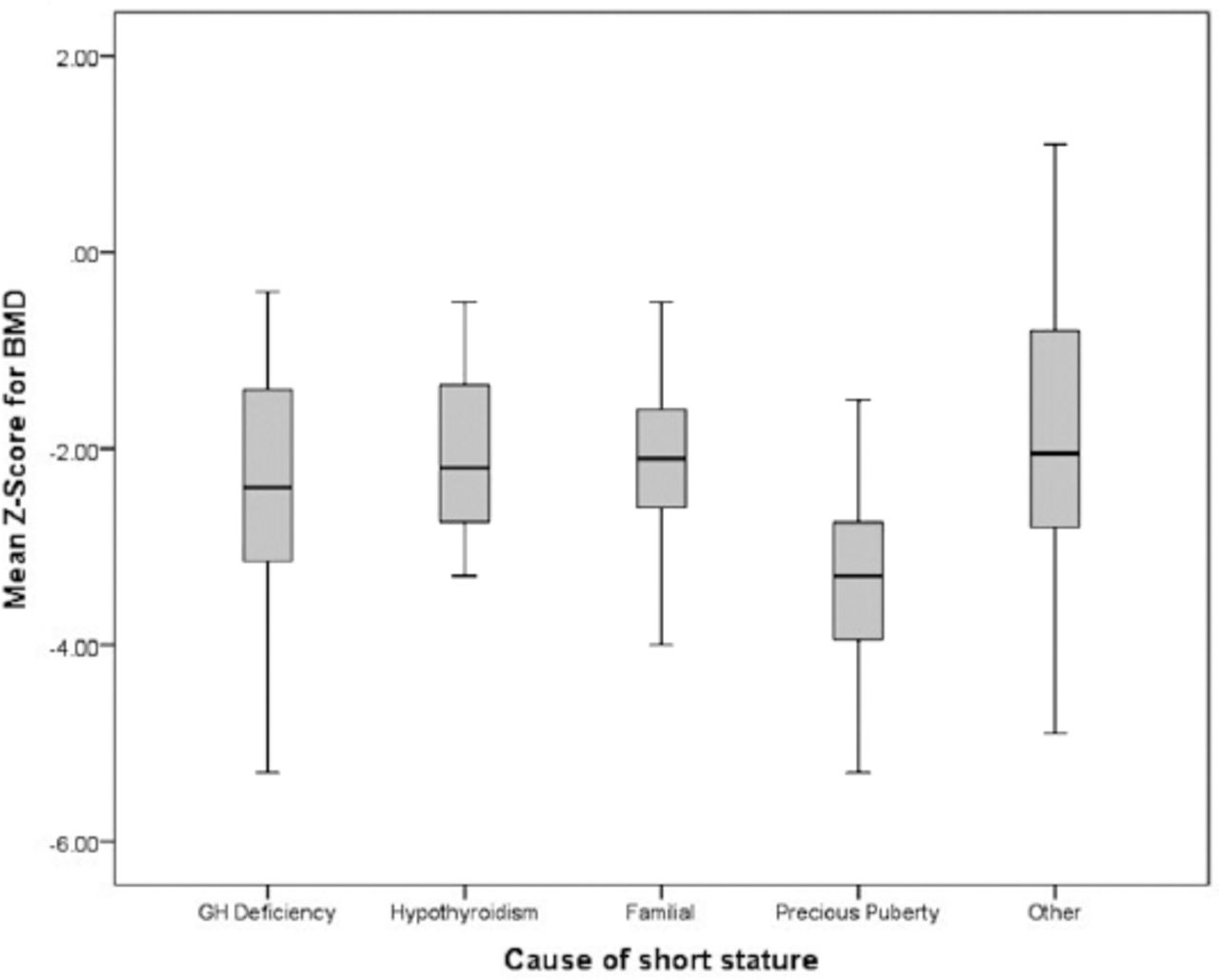
Mean z-scores for different causes of short stature plotted as a boxplot.
Discussion
We have shown that children with short stature have lower BMD z-scores than children of normal height, highlighting the need of BMD screening in children with short stature. Additional factors found to contribute to the abnormal BMD in children with short stature included height, GH deficiency, and pubertal stage. Furthermore, GH deficiency and the use of GnRH agonists was associated with the lowest BMD among children with short stature, and can therefore be considered as risk factors. Growth hormone has a major role in the process of bone formation.11 The absence or deficiency of GH result inhibits the remodeling process; thereby, leading to the gradual loss of BMD, as well as short stature, and slow bone maturation.
Children who have experienced early puberty and are using a GnRH agonist are at risk for lower BMD z-scores than their peers. A review performed in the United States found that these subjects have low BMD scores. Furthermore, the data from this study suggested that BMD should be carefully monitored in adolescents taking GnRH agonists,12 In our study, those who were receiving GnRH agonist treatment had lower BMD z-scores than those with other causes for short stature. This can be attributed to the suppressing effect on gender hormones, which slows the bone-remodeling process.13 The sample recruited for our study included children with short stature due to causes other than GH deficiency. These diseases also contributed to low BMD. With hypothyroidism, bone metabolism and mineral metabolism are accelerated by thyroid hormones. Therefore, hormone replacement therapy can cause decreased bone density. However, synthetic thyroid hormone use for longer than a year is required to achieve a significant effect.14,15 Previous results have shown that with adequate thyroxin replacement and effective vitamin D treatment, the effects on bone can be avoided.16
Familial short stature can be the result of genetic factors. Furthermore, bone density has been reported to be linked with family history. A study involving 2812 Korean adolescents found significant associations between the BMD values of offspring and the BMD of their parents. Recent genome-wide association studies have made great advances in identifying 62 significant genome-wide loci associated with low bone mass and osteoporotic fractures.17
Pubertal gender hormones (estradiol in females and testosterone in males) play important roles in bone mass acquisition. They also have a profound influence on longitudinal bone growth and bone-mineral build-up because they are essential for normal skeletal development and the achievement of peak-bone mass with appropriate timing.18 In healthy individuals, particularly females, pubertal levels of estradiol increase cortical bone thickness by directly increasing bone density and regulating bone remodeling.19 Moreover, androgens (either directly or by aromatization to estrogen) have a huge impact on bone strength because they regulate osteoblast activity through a faster, non-genomic mechanism using their receptors on the osteoblast cell surface.20 Our findings revealed higher BMD scores with higher Tanner stages, indicating that longer exposure to pubertal hormones is significantly associated with greater BMD z-scores and therefore, higher BMD. Similarly, a previous study performed in Lebanon on 335 healthy school children reported significant increases in bone mass parameters across different Tanner stages. This might have been because of effects of gender hormones throughout the more mature Tanner stages.21
A European multicenter study performed on a cohort of 371 children (aged 6 to 23 years) found that short children have lower BMD than their age-matched peers, even if their smaller bones are completely normal.11 Indeed, a smaller study performed in Venezuela found that body size and maturation were major determinants of BMD.22 Furthermore, a large Egyptian study of 4002 adolescents concluded that BMD is significantly lower among short stature individuals compared with those of normal height.23 Our findings are in agreement with previous studies, showing a significant association between short stature and lower BMD. In addition, we also found a positive association between height and higher BMD z-scores in short stature individuals.
Utilizing QUS as a measurement of BMD has been an established modality of BMD measurements. Although this method is well studied and has a clear role in adults, its use in pediatrics is still in need for further studies in order to refine the best methods for assessing bone strength in children.24
Study limitations
The paucity of studies investigating BMD using QUS screening in healthy populations of children within the gulf and middle-east regions makes it difficult to comparatively analyze our data. There is also a paucity of recent worldwide studies investigating BMD with QUS in healthy populations. A previous study using DXA to measure BMD in short stature children found that after 4 years most participants with previously abnormal results moved to within the normal range. The research team concluded that these children are often small for their age and therefore a low bone density may simply reflect a small body size.25 In future studies, it will be important to perform longitudinal studies using QUS to assess BMD over time in short stature individuals. Furthermore, as not all of the children in this previous study regained normal BMD, it is essential to carry out follow up studies specifically in these children.
In conclusion, our results show that quantitative ultrasound can be used for screening purposes and for easier assessment in children of high risk for low BMD. Further studies are necessary to identify these high risk children in order to provide early screening and management approaches. In addition, modifiable factors, such as nutritional status and vitamin D supplementation, require further study to confirm if they can improve BMD and bone health among children with short stature.
Acknowledgment
The research team would like to thank Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 28, 2020.
- Accepted May 19, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.