


Abstract
Objectives: To assess and enhance the efficiency of transfusion services in maternity hospitals.
Methods: A case control study was conducted from January to December 2016. A corrective policy of replacing preoperative type and hold step with blood transfusion request (BTR) hold was used only on healthy patients undergoing elective cesarean sections (c-section). The crossmatch/transfusion (C:T) ratio and a cost comparison were the evaluating factors. Data were analyzed using an Excel spreadsheet and SPSS statistical software.
Results: A total of 1,200 BTRs were analyzed, comprising 659 before implementation of the corrective policy and 541 blood transfusion requests after implementation of the corrective policy. From January to March, the C:T ratio of c-sections was nearly 7 times the American Association of Blood Banks recommended limit of 2.5. Most of the blood units (94%) were damaged due to repeated booking. After implementation, the cost-effectiveness of erythrocyte transfusion was greatly enhanced as all the ordered blood units were used and the C:T ratio was reduced to the ideal limit of one. The number of destroyed units was drastically decreased from 450 units to zero; as a result, 83% of the transfusion costs were saved.
Conclusion: The policy enhances the cost-effectiveness of erythrocyte transfusion and laboratory testing, and saves on additional, unnecessary costs.
Blood transfusion services are one of the most important treatment services in daily clinical practice, but are not without cost. Laboratory and blood transfusion testing consumes more than $65 billion per annum in the United States.1 One cause of this is excessive preoperative ordering of blood components; such as blood units for patients undergoing surgical operations.2 This can lead to shortages in blood bank inventories, waste of reagents, and therefore financial burdens on transfusion services.3-5 Additionally, a stock of reserved crossmatched units are held on standby for a period of time, after which they may expire and be discarded, further increasing the waste.6 This was recently observed in obstetric hemorrhage cases where nearly half of the erythrocyte units ordered for transfusion were not used and were returned to the blood bank.7 For this reason, transfusion service providers have implemented strategies to improve transfusion services. The maximum surgical blood order schedule has been proposed to limit the crossmatched to transfused units ratio (C:T) to lower than 2.5.8 Other strategies were also used, such as increasing transfusion policy awareness among the medical staff, and implementing the lean 6 sigma methodology.6,9 One of the more effective strategies of reducing unnecessary use involved limiting the blood transfusion request (BTR) received by the blood bank to typing and screening of a blood unit, rather than typing and crossmatching. Alghamdi et al10 recommended the use of type and screen approach on preoperative requests for cardiac operations to improve the C:T ratio by 66%. This also suggests that there is some latitude for improving the preoperative blood ordering and blood testing by reviewing the indications for transfusion and limiting unnecessary testing.
It has been reported that elective cesarean sections (c-section) are less risky than vaginal deliveries; however, the orders and crossmatching for blood transfusion for elective procedures can be excessive.5,11,12 A study revealed that only a small number of the blood units reserved for elective c-sections are used (0.5%, n=7809).5 This suggests that blood banks have to provide excessive units for elective c-sections and can be exposed to shortages. Some hospital facilities, such as surgical teams, and anesthesiologists seek to improve their practical performance without considering the burden on blood bank resources caused by unnecessary BTRs.9 In Saudi Arabia, blood transfusion services are hospital-based blood banking systems that are financially supported by the government. Frequent blood grouping and reservation of blood units, which are never used, results in a waste of blood bank resources. Previous studies of blood transfusions for c-sections either considered or recommended policies to limit the utilization of blood units to the type and hold step to reduce waste.5,13 However, they did not address the effects of holding the BTR for healthy patients on the increased consumption of costly reagents in blood typing and compatibility testing.
The aim of this study was to reduce the judicious usage of transfusion services by evaluating a new corrective policy designed to replace the “type and save” step. For healthy patients undergoing elective c-sections, this policy is to consist of only holding the BTR (no testing). Findings will be compared before and after the implementation of this corrective policy.
Methods
The study was conducted at Abha Maternity and Children’s Hospital (AMCH), Abha, Saudi Arabia. A paper-based, referral, and educational hospital with a capacity of 240 beds; and, is in the Southern region of Saudi Arabia. Informed consent to access blood bank records and data from the maternity hospital patients was conducted by the referring hospital. We obtained approval from the referring hospital to use these data and ethical approval from the Research Review Committee at the Faculty of Applied Medical Sciences (no. 64886/37). Patient data were anonymized before analysis, according to the Saudi Ministry of Health regulations and the principles of the Declaration of Helsinki.
Abha Maternity and Children’s Hospital, Abha, Saudi Arabia was selected due to inefficient blood unit utilization caused by the unnecessary reservation of blood units for c-sections. These blood units are commonly not used and are sometimes discarded due to passing the expiration dates. This study aimed to optimize the usage of blood units in order to improve blood bank inventory and efficiency by reducing unnecessary ordering for patients who may not need erythrocyte transfusions.5 The design of the study was based on a review of all the documents related to the work policies of the blood bank: both the internal policies, and the policies which regulate relationships with other departments. Data collection depended on the classification of blood transfusion requests according to the patient’s health status as well as the number of required units. This study took almost 3 months due to the absence of a computer system in the hospital. The sources of information were paper records and archived blood transfusion forms.
A retrospective cohort study from January 2016 to March 2016 was used to analyze routinely collected maternity BTRs at the blood bank laboratory archive. Preoperative maternity BTRs (n=1198), including 659 BTRs for elective c-sections, were reviewed and classified; and, hemoglobin concentrations or placental issues, and the total number of crossmatched and transfused blood units were recorded.
The findings of all collected data were summarized and explored. The retrospective C:T ratio for elective c-sections was used as a control and compared to the C:T ratio after the implementation of the “save and type” policy.
Prospective analysis after the newly implemented corrective policy on c-section BTRs
The prospective analysis (from April 2016 to December 2016) was a more comprehensive assessment of BTRs (n=541) as per the instructions of the anesthesia department, which dictated blood unit reservations as a condition for patient inclusion in the schedule of operations. Prior to policy implementation, AMCH policy required that all preoperative BTRs must be typed, screened, crossmatched, and reserved for a maximum of 3 days prior to c-sections. The new policy classified the maternity BTRs into 2 types based on the hemoglobin concentration and the expected risk during or after operation. Preoperative BTRs for patients with a hemoglobin of ≤12 g/dl or a diagnosis of risk factors such as placenta previa or accreta, a previous abortion, acute hemorrhage, or multiple pregnancies were excluded from the corrective policy and considered at risk. Vaginal births and emergency cases were also excluded from the study. Blood transfusion requests included in the corrective policy were those for patients undergoing elective c-sections, with a hemoglobin concentration of >12 g/dl and no or low risk factors such as umbilical cord prolapse, or small maternal pelvis. The requested units for healthy and uncomplicated cases (depending on retrospective findings, those who rarely received blood) were excluded from the “type and save” protocol. Alternatively, BTRs were received and put on hold without typing of the erythrocyte unit(s), known as a “receive and hold”. If a blood transfusion was required intra- or post-operatively, the BTRs was treated as an emergency and the blood unit(s) crossmatched by immediate spin depending on the 28th-week of pregnancy results of allo-antibody screening. This type of BTR was excluded. Bleeding BTRs were treated according to the emergency hemorrhage protocol, and subsequently massively transfused with uncrossmatched units. This new policy was implemented to improve the cost-effectiveness of the blood bank by reducing the costly consumption of reagents and erythrocyte unit waste caused by preoperative non-risky c-section BTRs. Auditing of reagent consumption, transfusion costs, and the number of crossmatched, transfused units was performed continuously to assess improvements in efficiency.
Patients with a hemoglobin of ≤12 g/dl or a diagnosis of risk factors such as placenta previa or accreta, a previous abortion, acute hemorrhage, or multiple pregnancies were excluded from the corrective policy and considered at risk. Vaginal births emergency cases were also excluded from the policy. Patients undergoing elective c-sections, with a hemoglobin concentration of >12 g/dl or have no or low risk factors such as small maternal pelvis and umbilical cord prolapse were included in this policy.
Statistical analysis
Data were analyzed via Excel® 2010 (Microsoft®, Redmond, Washington, U.S.A.) spreadsheets or the Statistics Package for Social Sciences for Windows, version 22 (IBM Corp, Armonk, NY, USA). The C:T ratio was used as transfusion services efficiency indicator. A 2-tailed Chi-squared test (1 degree of freedom [df.]) was used to examine whether there was no difference between the total number of maternity and c-section operations patients before and after the implementation of the corrective policy. The test was also used to examine whether there was no difference between the total number of risky and non-risky patients before and after implementation. A one-tailed McNemars’ Chi-squared test (df. 1) for paired data with Yates correction was used to examine whether the BTR holding policy significantly reduced the number of crossmatched units in comparison to the period before implementation. A similar test was also used to examine whether the BTR holding policy significantly reduced the number of expired units. A p-value of <0.05 was statistically significant.
Cost estimation
The financial value of the total number of ID gel cards and reagents (DiaCell I-II-III, ABO/RhD + Reverse Grouping, Liss/Coombs) used for each BTR was calculated according to the price quotation submitted by the manufacturers. All reagents used for ABO typing, and antibody screening and identification were obtained from BioRad (BioRad, Hercules, California, USA).
Calculation of blood unit cost. [Total number of (crossmatched, or transfused or expired) blood units x cost of a single unit ($133)]
Calculation of crossmatch and group and hold cost. The total cost of type and hold calculation: [Total number of patients + total transfused + un-transfused + wasted blood units) X (cost of ID gel cards + reagents of DiaCell I-II-III, ABO/Rh+ reverse grouping ($2.65)]
Crossmatch calculation: [Total number of patients + total transfused + un-transfused + wasted blood units) X (cost of ID gel cards + reagents of Liss/Coombs ($0.98 +$0.37))]
Results
Patients demographics are shown in Table 1. The blood bank laboratory received BTRs for 1,200 patients undergoing c-section operations from January to December 2016. The patients’ ages ranged from 21 to 37 years with a mean hemoglobin concentration of 12 g/dl (normal range = 12 to 15.5 g/dl). Overall, there was no significant difference in the total number of maternity and c-section patients before and after the implementation of the study (χ2(1) = 3.65, p=0.056). Of these patients, approximately 55% underwent c-sections from January to March 2016. Before the implementation policy, all of the c-section patients reserved erythrocyte transfusions. After the implementation of the BTR sorting policy, 81.9% of c-sections were healthy and their BTRs were held without further testing.
Demographics of patients in the study from January to December 2016.
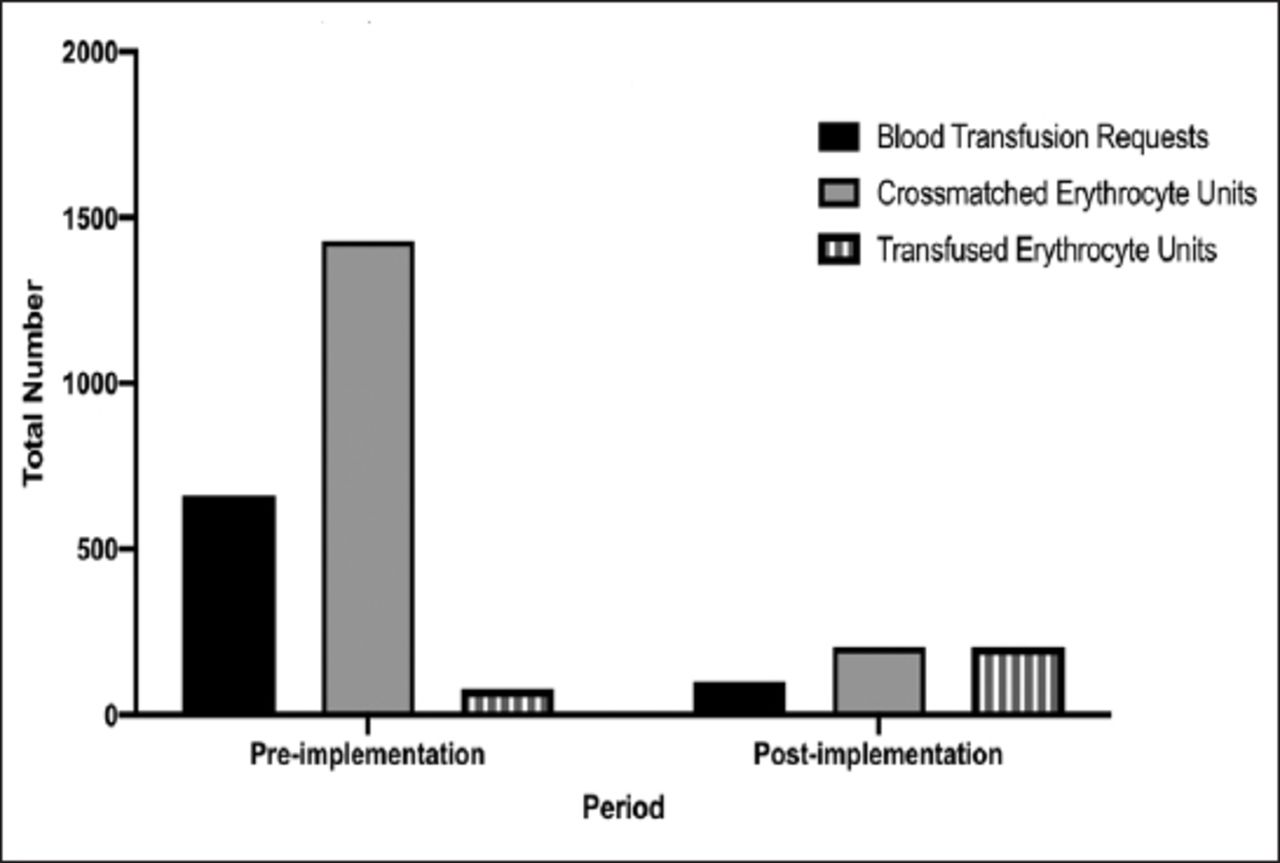
Figure 1 shows the number of BTRs, crossmatched, and transfused units during the 3 months before the implementation of the corrective policy. Of all BTRs received by the blood bank, 55% were for patients admitted for a c-section. The BTRs for c-section patients reserved the majority (76.4 %) of crossmatched units for all maternity operations, but only 5.4% were actually transfused. Sorting of BTRs according to patients’ hemoglobin concentration excluded the BTRs of healthy women undergoing elective c-section from routine compatibility tests. Consequently, a significant reduction in blood utilization was observed, and 100% of crossmatched blood units were transfused unlike before implementation (McNemars’ χ2(1)=55.408, p<0.001) (Figure 2). Hence, the C:T ratio was significantly reduced to 18 times that of before the implementation, reducing the overall C:T ratio for all maternity operations to nearly the ideal value of one.

The utilization of erythrocyte units for maternity operations at Abha Maternity and Children’s Hospital (AMCH), Abha, Saudi Arabia in the pre-implementation period. Includes cesarean section (c-section) operations before the implementation of blood transfusion request (BTR) holding policy, and the omission of the type and hold step at AMCH (January to March 2016). A total of 1,198 BTRs were received in the AMCH blood bank which reserved 1871 crossmatched units. Of all the maternity operations BTRs, 659 BTRs were for c-section operations which reserved 1429 crossmatched units of all maternity operations at AMCH. However, only 78 of these erythrocyte units were actually transfused to elective c-section patients.

The cost-effectiveness of erythrocyte transfusion units for cesarean section (c-section) operations pre- and post- implementation of the corrective policy at Abha Maternity and Children’s Hospital, Abha, Saudi Arabia (January - December 2016). The corrective policy excluded BTRs of healthy women from routine compatibility tests. The crossmatch/transfusion ratio for c-section operations was 18 fold the recommended C:T limit indicating that overall 94.5% of the crossmatched units were not transfused. The corrective sorting of BTRs according to the expected need for transfusions significantly increased the efficiency of blood utilization to 100%. Hence, all crossmatched blood units were transfused (McNemars’ χ2(1) = 55.408, p<0.001).
Table 2 displays the impact of the new policy on the estimated total costs of the crossmatched, transfused, and expired units as well as the total cost of routine testing pre- and post-correction. In view of the pre-correction cost of the crossmatched and transfused units, a difference of $179,683 between the 2 totals was observed. The total cost of 450 units that expired due to re-reservation exceeded the cost of the pre-correction transfused units by more than 5 times. After implementation of the corrective policy, the number of expired units was significantly reduced to 0 in comparison to the pre-correction period (McNemars’ χ2(1) = 91.781, p<0.001). Consequently, the total financial cost of all units and tests were decreased after the implementation of the corrective policy. The financial value of testing of the reserved units which were not transfused together with the value of expired units constituted 79% of the total cost of reagent and materials necessary for routine compatibility testing (antibody screening, ABO typing, and crossmatching).
Total cost of erythrocyte transfusions before and after the implementation of the corrective blood transfusion request holding policy.
Discussion
Blood transfusion plays a major role in the management of both hematological disorders and surgical procedures. This widespread need has created a growing demand for blood units; however, not all blood units are pre-emptively ordered for surgery are utilized.2 The costs of typing, antibody identification and crossmatching also contribute to the direct expenses of blood banks, especially when the blood is not transfused.5 Since 1967, different policies and low cost measures have been used to improve the cost-effectiveness of blood transfusions.6,14,15 These measures limited BTRs to one of 3 steps: 1) type and crossmatch; 2) type, screen and hold; 3) or type and save.8,10 Some countries such as the United Kingdom use the electronic crossmatch as an approach to improve patients’ safety as well as the cost-effectiveness of erythrocyte transfusions.16 However, this system requires regular blood donors with known history. In other countries, such as Saudi Arabia, the donation pool is mainly compromised of replacement donors which adds more stress to blood banks. The need to prepare blood units for c-section has been a subject for debate. Typing and holding BTRs for healthy elective c-section patients lead to reagents waste and erythrocyte units. Approximately half of the BTRs reviewed in this study were for maternity cases; however, very few of the crossmatched units were utilized. This is because most of the women who undergo elective surgery were in good health and tolerated the amount of blood lost (which does not typically exceed one litre according to some studies) especially with an average hematocrit level not less than 20%.3-5 In addition, BTRs for elective c-sections of healthy, non-high-risk patients do not require routine testing.3 This is in concordance with a previous study that found most patients who undergo an elective c-section do not require a blood transfusion.5,17 Therefore, the requesting of blood units should be rationalized, so that blood is saved for emergencies. Some studies have examined the practice of type and hold, and the controlled reservation of blood units and have concluded that the practice leads to an increase in the number of typing, screening, and crossmatching tests.18,19 Accordingly, the unnecessary pre-correction costs of testing increased as shown in Table 2, because the majority of the elective c-section patients did not require blood transfusion. This study points out that the type and hold technique might not be an effective strategy to limit the reservation of units from routine testing for elective c-sections. Therefore, a new policy may be used to improve the cost-effectiveness of erythrocyte transfusion. In this study, the policy of preoperative type and hold was replaced by BTR hold without further testing only for patients undergoing elective c-sections without anemia, placental complications, or emergency transfusions.
A recent study advocated the use of “Deming Plan, Do, Check, and Act cycle” in the management of blood units. This strategy had a positive effect of decreasing the blood unit waste that resulted from the reservation of units, however, it also had the negative impact of increasing the consumption of reagents during the type and screen step.20 Reagent waste places a great burden on hospitals, especially those in countries that import reagents.21,22 Our approach sorts the BTRs of c-section patients according to health status and improves the efficiency of blood services. The type and hold step was not implemented for elective c-section cases but was kept only for complicated cases, an approach highly recommended in previous studies.5 The ideal C:T ratio should be 1.0, but a ratio below 2.5 indicates an acceptably efficient utilization.22 In this study, replacing the type and hold protocol with holding the BTRs for healthy elective c-sections has dramatically improved the C:T ratio to one. Other policies reported in previous studies reduced the C:T ratio to between 1.5 and 2.5.7,10 The implementation of cost-effective policies may be affected by hospital size, type of operations conducted within the hospitals, and number of admitted patients.23 In this study, 50% to 60% of healthy pregnant women may choose elective c-sections instead of vaginal delivery. Reaching the C:T ratio of one was possible due to the implementation of the corrective policy on the BTRs for healthy women. Other hospitals may adopt this policy after reviewing the indications for transfusions and the patients’ demographics. It might be argued that the healthy c-section patients may require a blood transfusion intraoperatively or post-operatively and that this policy may compromise patients’ safety. Patients that meet these criteria would follow the emergency protocol of the hospital and would not be affected by the BTR holding policy. Additionally, no adverse outcomes due to the unavailability of blood units were recorded in this study, and most of the patients left the hospital within 24 hours of the operation. The financial cost assessment indicates the success of these measures. The reduction from the previous costs were significant. Importantly, the number of non-transfused units reserved for c-sections were significantly reduced. This reduction may have a positive effect on all blood groups in general including O-negative erythrocyte units. Some blood transfusion organizations recommend that O-negative units used should not exceed 10%.20 Eliminating reservation increased the possibility of units being transfused, and reduced wasting of units which may include the rare O-negative units. It is worthwhile to emphasise the large number of units wasted pre-implementation of the study compared to the period after the policy implementation.
Study limitations
The preoperative erythrocyte transfusion requests for healthy patients undergoing elective c-sections in a maternity hospital did not consider intraoperative or post-operative erythrocyte transfusion. During the study, we noticed a gap in the interface between the surgeons, and the blood bank, which is theorized to also be a reason for the over-ordering of blood units. For this limitation, ways to bridge this gap are needed to be investigated with new ethical approval. Studying the implementation of this policy on other maternity hospitals may highlights other variables contributing to erythrocyte waste; however, this was not possible to conduct due to time and logistical restrictions. The impact of this policy on individual erythrocyte blood groups and other blood components should be thoroughly studied. Future comparative studies on the erythrocyte transfusion policies in maternity and other specialist hospitals may be useful to introduce new transfusion policies improving the transfusion service. For this type of study, a national electronic database for blood donors and patients is useful for managing the transfusion service and the patients’ needs for transfusion. A national transfusion service may also invest in the recruitment of regular blood donors to use electronic crossmatching to improve the safety and reduce the cost of the transfusion service.
In conclusion, the corrective policy of omitting the type and hold step for healthy patients undergoing elective c-sections has greatly improved the utilization of erythrocyte transfusion and reduced the costly consumption of reagents in the blood bank of a maternity hospital. This policy can be adopted in maternity hospital blood banks where which inventory in mainly supplied by replacement blood donors.
Acknowledgment
We would like to thank Oxbridge proofreading (https://oxbridgeproofreading.co.uk) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 3, 2019.
- Accepted April 19, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.