


Abstract
Objectives: To demonstrate the correction of overhanging alar with the vestibular triangular excision technique using preoperative and postoperative photographs.
Methods: This descriptive retrospective study was conducted at King Abdulaziz University Hospital, Riyadh, Saudi Arabia. Fifty patients who underwent open rhinoplasty with the vestibular triangular excision technique were retrospectively assessed. Preoperative and postoperative photographs were examined to evaluate the alar-columellar relationship. Patients included had undergone either primary or revision rhinoplasties between January 2013 and March 2018 and had a thick hanging alar with a grade IV Gunter’s rating for alar-columellar discrepancies. Patient outcomes and satisfaction were subjectively assessed using the rhinoplasty outcome evaluation (ROE) scale and visual analog scale (VAS) by independent analysis of the right lateral, left lateral, and frontal view photographs by 2 rhinoplasty surgeons, both preoperatively and 1-year postoperatively. Statistical significance was calculated by Wilcoxon signed-rank tests.
Results: Patients’ ages ranged from 18 to 37 years (mean, 26.34). The study included 22 men (44%) and 28 women (56%). Mean preoperative and postoperative ROE scores were 10.12 and 19.3 and VAS scores 5.14 and 7.94. P-values for preoperative and postoperative comparison of both ROE and VAS were statistically significant (p=0.001).
Conclusion: Caring of alar soft tissue during rhinoplasty is important to correct overhanging alar to improve nasal appearance and patient satisfaction. The sail excision technique is reliable and simple and provides good patient satisfaction.
Rhinoplasty surgery is one of the most difficult facial plastic surgeries and satisfactory results are obtained when millimeter-sized defects are surgically resolved. A favorable postoperative relationship between the alar rim and columella as well as the nostril proportions is crucial to achieve good aesthetic results. If ala and soft tissue are not addressed well during rhinoplasty, due to the risk of changing the nasal shape.
Use of alar soft tissue excision techniques with good operative skill yields a better result and improves patient satisfaction.1 The main goals of operating on the alar soft tissue is to achieve an aesthetic balance and natural appearance, to retain a natural nasal shape, and avoid the need for revision surgery.1-3 Most surgeons focus only on the major bony and soft tissue abnormalities and overlook minor alar-columellar discrepancies. However, careful preoperative analysis and intraoperative address of minor alar-columellar abnormalities, such as hanging ala may improve postoperative patient aesthetics and surgeon satisfaction. Hanging ala can be corrected with multiple surgical techniques. In Saudi Arabia, many patients have very thick skin and hanging ala.
Hanging ala correction has been studied previously by other doctors.1,2,4 However, studies assessing patient satisfaction post correction of hanging ala in patients with thick nasal skin are lacking, and some studies have not completely analyzed their results, for example by missing the comparison of some variables. Our study was designed to study the effect of sail excision on overhanging alar in thick nasal skin on patient satisfaction.
The present study demonstrates our recent experiences with the correction of overhanging thick ala using the vestibular triangular excision technique in Saudi Arabia. Postoperative outcomes were measured by comparing the preoperative and postoperative patient photograps.
Our study aimed to improve patient satisfaction post rhinoplasty, which may have contributed to the increase in awareness of alar soft tissue, especially in cases of thick nasal skin.
Methods
This was a descriptive retrospective study, and patients were retrospectively recruited from King Abdulaziz University Hospital, Riyadh, Saudi Arabia. Patients who simultaneously undergoing open rhinoplasty and vestibular triangular excisions were included. Patients’ alar-columellar relationship was carefully analyzed using preoperative and postoperative frontal, right, and left lateral view photographs. The study patients had undergone primary or revision rhinoplasty between January 2013 and March 2018. Only patients with thick hanging alar skin with grade IV Gunter’s rating for alar-columellar discrepancy were included.4
The inclusion criteria were: i) patients who underwent rhinoplasty by the vestibular triangular excision technique, ii) patients with follow up more than a year, and iii) age ≥18 years. The exclusion criteria for patients were: a) patient with follow up less than a year, age <18 years, and rhinoplasty technique other than vestibular triangle excision. A single senior consultant at King Abdulaziz University Hospital, Riyadh, performed all of the surgeries.
Surgical results and satisfaction were assessed subjectively and objectively by the 2 rhinoplasty surgeons and patients. Patient satisfaction was measured with the rhinoplasty outcome evaluation (ROE) score (range, 0 to 24, with 0 representing the lowest level of satisfaction).5 For a more objective assessment, 2 rhinoplasty surgeons assessed the preoperative and postoperative 1-year patient photographs taken from 3 different views (right, left, and front profiles), which allowed for the assessment of the alar-columellar relationship. The surgeons then rated the postoperative results by visual analog scale (VAS), which ranges from 0 to 10, where 0 represents the worst results and 10 represents the most normal alar-columellar relationship.
For search for prior related research, specific medical search engines, namely, PubMed, Medline, Science Direct, Scopus, and Google scholar, were used. The study was approved by the Institutional Review Board at the College of Medicine Research Center, King Saud University (reference number 20/0352/IRB) and was completed in accordance with the Declaration of Helsinki. Informed consent was obtained from all patients who participated in the study.
Statistical analysis
Data were analyzed using IBM SPSS version 21 (IBM corp. Armonk, NY, USA). Descriptive statistics for the continuous variables were interpreted as mean ± standard deviation and categorical variables were reported as frequencies and percentages. We considered demographic and preoperative results, measured by the ROE and VAS, variables as correlates and post-operative ROE and VAS variables as outcomes. Wilcoxon signed-rank test was used to calculate significance. A p value <0.05 was considered statistically significant.
Surgical technique
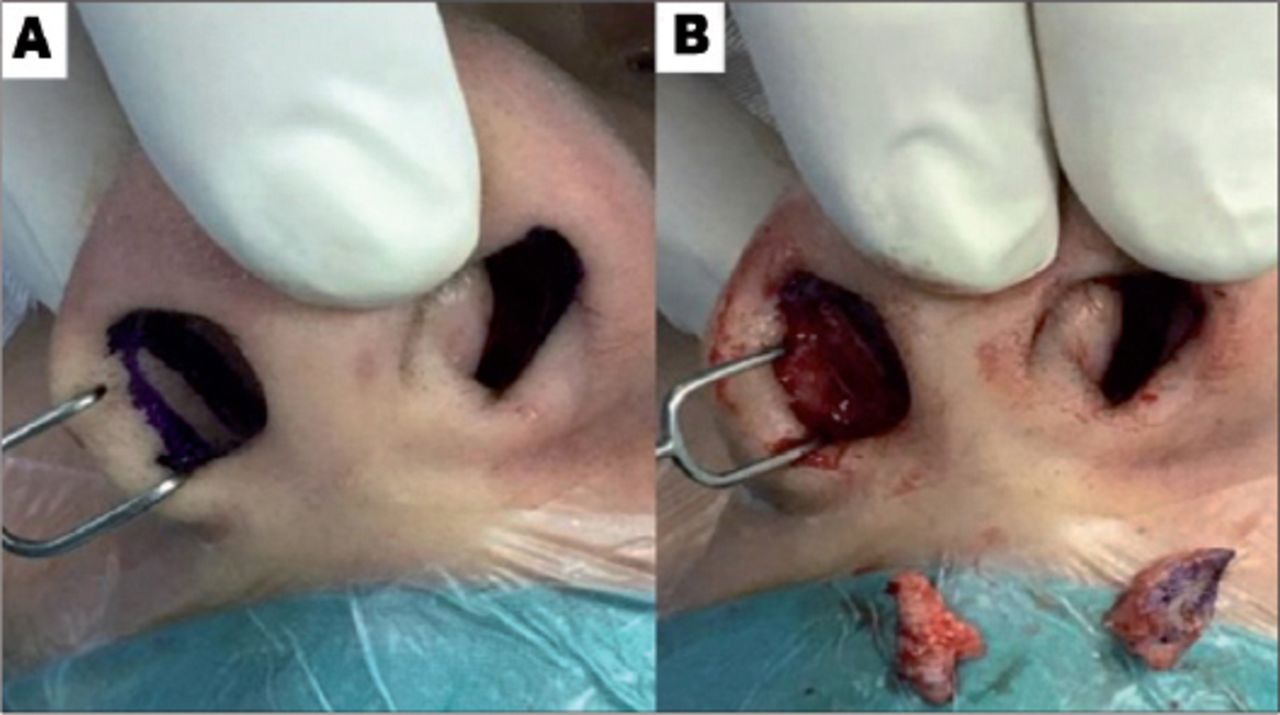
First, a full and detailed assessment of alar in relation to columella was performed, and the degree of overhanging ala was estimated on lateral view. The distance from the long axis of the nostril to alar rim or columella should range between 1 to 2 mm (Figure 1). Thereafter, a triangular-shaped sail was marked on the vestibular side of the ala. The top of the excised part of the sail was located at the highest point of the alar-columellar line, the anterior edge was located just above the alar rim, and the posterior edge was located at the vestibular groove (Figure 2). The marked area was then injected with 2% lidocaine and epinephrine 1:100,000. Next, the vestibular skin was incised along with the underlying subcutaneous tissue, while ensuring extreme caution to prevent injury to the overlying skin (Figure 3). The incision was closed with a single layer of 6 to 0 polydioxanone (PDS) suture. This procedure can be completed either at the beginning or at the end of rhinoplasty. We find it better to complete this procedure as the first step, before any other incisions were made, to allow easy and full manipulation of alar rim.

Ideal alar-columellar relationship. The greatest distance from top of the nostril to either the alar rim or the columella should be 1 to 2 mm or AB = AC = 1 to 2 mm.

Schematic illustration of the sail excision technique. A) Anterior edge was located just above the alar rim. B) Posterior edge was located at the vestibular groove. C) Top of the excision part of sail was located at the highest point of the alar-columellar line. D) Base of the excision part of sail was a connection point between anterior and posterior edge.

Intra operative view showing the sail A) incision marking and B) sail triangular excision.
Results
Fifty patients were included in the present study (22 men and 28 women). Patients’ ages ranged from 18 to 37 years, with a mean age of 26.34 years. All patients had undergone surgery at least one year ago, and had preoperative and postoperative 1-year pictures available for review.
Visual analog scale
Preoperative VAS scores ranged from 3 to 7, with a mean score of 5.14, while postoperative scores ranged from 5 to 9, with a mean score of 7.94. Postoperative scores were significantly higher than the preoperative ones (p=0.001) (Table 1).
Preoperative and postoperative patient (rhinoplasty outcome evaluation and surgeon (visual analog scale) satisfaction.
Rhinoplasty outcome evaluation scores for preoperative satisfaction ranged from 5 to 15, with a mean score of 10.12, while postoperative scores ranged from 14 to 23, with a mean score of 19.3. Postoperative scores were significant (p=0.001) (Table 1).
Discussion
Considering the complexities of plastic surgery, many surgeons focus only on the major bony and soft tissue abnormalities and mostly overlook the minor alar-columellar discrepancies. However, surgical rectification of these discrepancies can significantly influence patient and surgeon satisfaction. The alar-columellar relationship was first described in 1996 by Gunter et al,4 who categorized these relationships into 6 distinct subtypes and defined the related abnormalities, including overhanging and retracted alar. To assess the alar-columellar relationship, a line is drawn between the alar-cheek and tip. Normal columellar show should be 2 mm to 4 mm, with less “hooding” or overhang, also termed “columella”.4 Alar-columellar discrepancies, when surgically corrected, should appear normally shaped with normal natural contours, drawing a line from the top of the nostril to the floor of nostril at the ala crease on lateral view, if ala is within 1.5 to 2 mm of this line, that means the ala is normally located and subsequent revision surgeries are not required.4 Moreover, surgery would only incur scars that are invisible or of acceptable size.1
The current literature describes many ways of correcting an overhanging ala, but lacks detailed descriptions of the ideal way to deal with overhanging ala associated with thick skin without excision of the skin. This is particularly challenging in Saudi Arabia, where many individuals might have thicker skin. The use of the traditional alar lift technique depends on skin thickness. Therefore, for a hanging columella associated with thick skin, surgeons remove part of the alar lining along with the subcutaneous tissue, as first proposed by Gunter.6 In contrast, for a hanging columella associated with thin skin, surgeons often resect part of the lateral crus without removal of the lining, as suggested by McKinney.7 Additional surgical methods exist to correct overhanging alar. For instance, Millard managed overhanging ala by shaping and decreasing the width of the alar base.8 This technique was later changed by excising 3-mm of the vestibular skin. However, direct external skin excisions in patients with thick skin have been associated with noticeable scarring.8 In 2010, Baladiang et al9 modified the alar lift technique to the sail excision technique, in which the hanging ala is managed by removal of the vestibular lining. This was later changed by removing the skin, creating a new alar rim by folding the skin of alar rim and suturing it to the vestibule defect. The advantage of this technique is that the incision was carried out on the vestibule, so a smaller scar was formed.9
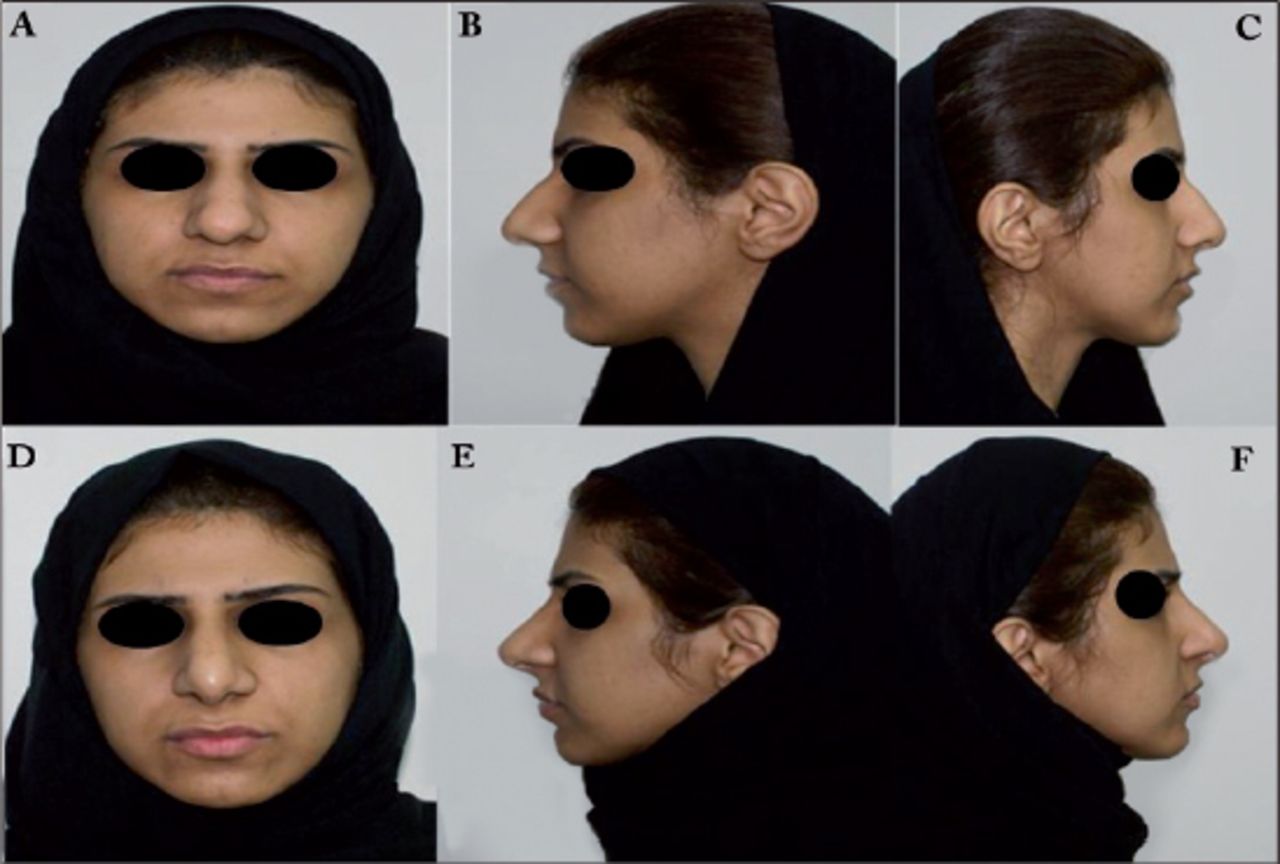
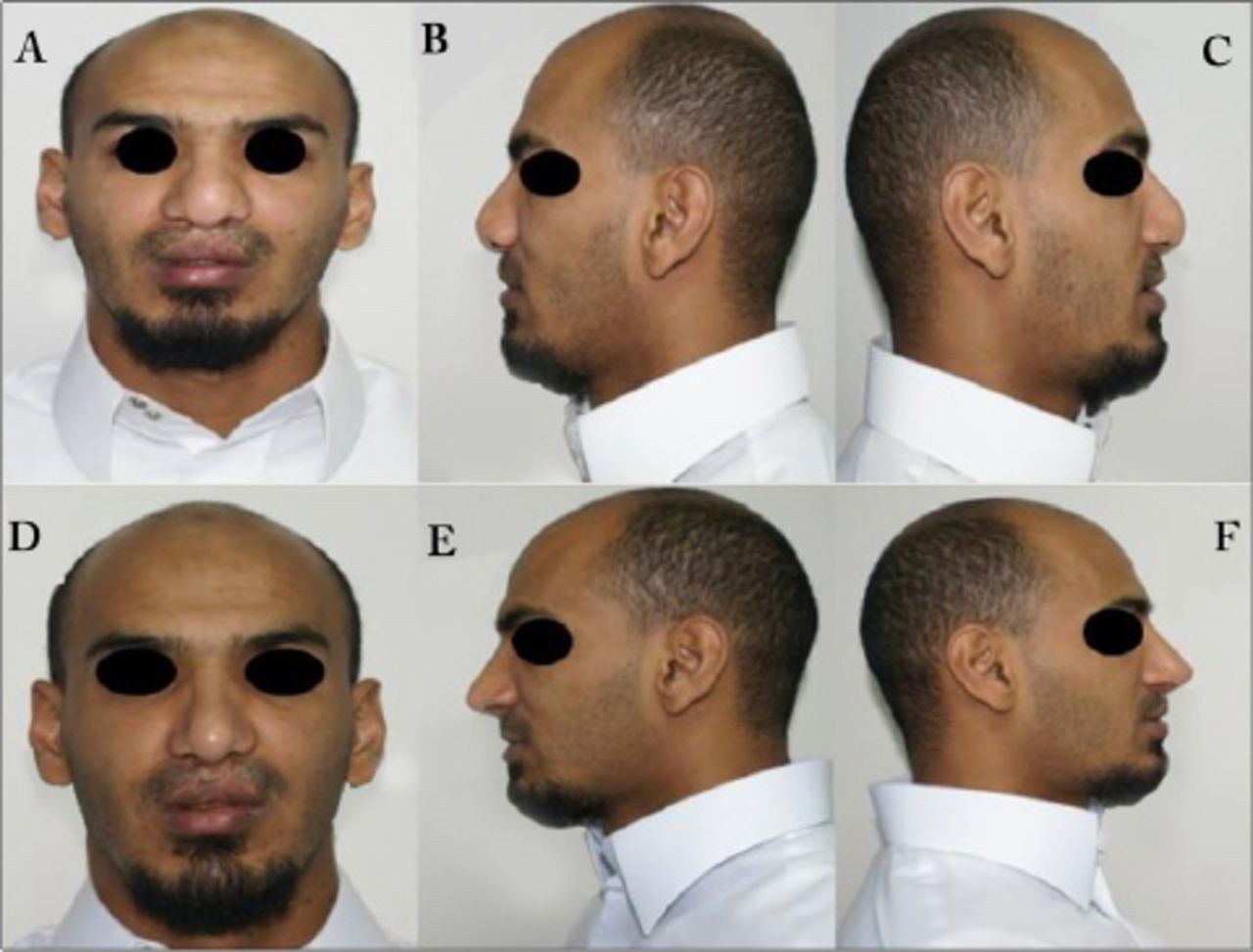
Using the rhinoplasty and vestibular/sail triangle excision technique in the present study, we achieved excellent patient satisfaction rates (Figures 4-6). We did not encounter cases of hypertrophic scars, vestibular stenosis, or scar contractures, as discussed by Baladiang.9 Furthermore, with the use of absorbable PDS sutures instead of nylon sutures, we eliminated the need for suture removal. Polydioxanone was thus superior for skin ligation and more delicate than nylon, decreasing the risk of skin injury. A decreased rate of revision surgery and postoperative dissatisfaction were observed when the overhanging ala was corrected using the vestibular triangular excision technique during rhinoplasty

Pre and post-operative view A) pre-operative frontal view, B) pre-operative left lateral view, C) pre-operative right lateral view, D) post-operative frontal view, E) post-operative left lateral view, and F) post-operative right lateral view.

Pre and post-operative view A) pre-operative frontal view, B) pre-operative left lateral view, C) pre-operative right lateral view, D) post-operative frontal view, E) post-operative left lateral view, and F) post-operative right lateral view.

Pre and post-operative view A) pre-operative frontal view, B) pre-operative left lateral view, C) pre-operative right lateral view, D) post-operative frontal view, E) post-operative left lateral view, and F) post-operative right lateral view.
This study was limited by its single-center and retrospective design. Future studies in the form of multi-center studies, with a larger multiethnic patient population and more tools of evaluation of outcomes, are warranted.
In conclusion, in the present study, patient satisfaction improved after vestibular triangular excision for overhanging ala. Finally, we report a reliable and simple surgical technique with a reasonable learning curve and good patient satisfaction for postoperative results.
Acknowledgment
We gratefully acknowledge Prof. Sameer Bafaqeeh, who has shared his experience with us; also, we would like to thank Norjanah Dimatunday who helped us in drawing the illustrations. We would also like to thank Editage (ww.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 4, 2020.
- Accepted May 11, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.