


Abstract
Objectives: To examine the association of several psychosocial disorders with quality of life (QoL) among chronic hemodialysis patients.
Methods: A cross-sectional observational study was conducted in 2018 and recruited chronic hemodialysis patients from 3 major hemodialysis centers in Riyadh, Kingdom of Saudi Arabia (KSA). Quality of life was assessed using a previously validated Arabic version of the dialysis version-III of the QoL index.
Results: A total of 101 patients (56 males and 45 females) were included. The mean age was 54.0±12.3 years. The overall mean of QoL was 88.8/100 points (out of 100). The family (95.0%) and psychological/spiritual (94.7%) domains had the highest scores. The prevalence of psychosocial disorders was 24.8% for depressive symptoms, 15.8% for anxiety symptoms, 88.1% for cognitive impairment, 76.8% for insecure attachment style, and 38.6% for medium/high severity of somatic symptoms. All psychosocial disorders and higher cognition level were negatively correlated with QoL (Spearman correlation r ranged between -0.228- -0.468). After adjusting for sociodemographic and clinical characteristics, anxiety symptoms and higher cognition level were independent predictors of poor QoL, while marital status (married) was an independent predictor of good QoL.
Conclusion: We report higher QoL and relatively better psychosocial profiles among current chronic hemodialysis patients than reported before. Psychosocial disorders specially anxiety can negatively impact QoL. Patients who were not cognitively impaired were more negatively affected in QOL. The findings re-emphasize the importance of the early detection and management of psychosocial disorders to improve QoL in chronic hemodialysis patients.
Hemodialysis is a lifesaving chronic therapy for an increasing number of patients with end-stage renal disease (ESRD).1 Researchers estimate that approximately 2 million patients worldwide receive chronic hemodialysis.2 The use of hemodialysis has been increasing and is expected to increase even more in the next decades, mainly due to aging of the population and increasing burden of contributing diseases such as diabetes and hypertension.2,3 This is expected to considerably increase the financial burden on the healthcare system, especially in developing countries.4 In Kingdom of Saudi Arabia (KSA), the prevalence and incidence of ESRD have been steadily increasing in recent decades.5 Similarly, the number of patients receiving hemodialysis increased from approximately 4,000 in 1995 to nearly 18,000 in 2017.6
In addition to the pathophysiological effects of ESRD and hemodialysis, patients also face significant lifestyle challenges that can increase the risk of developing depression, anxiety, cognitive impairment, and other psychosocial problems.7-9 The presence of these psychosocial disorders can negatively impact the course of the disease, including mortality and hospitalization.10,11 Additionally, several studies have suggested the negative impact of psychosocial disorders on different domains of quality of life (QoL) among chronic dialysis patients.12-14
As expected, chronic hemodialysis patients in KSA have poor QoL and a higher prevalence of depression and anxiety.15-18 Nevertheless, the high level of religiosity and spiritual coping among these patients may positively impact QoL.19 Additionally, it has been suggested that depression among these patients could be lower than similar patients in other parts of the world.20 Although psychological symptoms have been examined in relation to hemodialysis adaptation, no studies examined the impact of psychosocial disorders on QoL among chronic hemodialysis patients in KSA.21 This is especially interesting in KSA, which has a unique conservative culture with a profound role of religion and family support. The current study aimed to examine the association of psychosocial disorders, including depression, anxiety, cognitive impairment, insecure attachment style, and severe somatic symptoms, with QoL among chronic hemodialysis patients.
Methods
Official statistics points to the presence of 270 hemodialysis centers in KSA, with approximately 50% of them directly funded by the Ministry of Health.6 The current study was conducted among patients receiving maintenance hemodialysis at 3 major centers in Riyadh, KSA (King Saud University Medical City, Prince Sultan Military Medical City, and King Salman Center for Kidney Diseases). Approximately 700 patients are regularly receiving free hemodialysis at the 3 centers.
Study design
A cross-sectional observational study was conducted between January and July 2018. All required ethical approvals were obtained from the institutional review board at the Faculty of Medicine at King Saud University in Riyadh, KSA. Additionally, administrative approvals were obtained from the administrations of the 3 centers.
Population
Patients were recruited using convenience sampling technique. Therefore, consecutive chronic hemodialysis patients at the 3 included centers were invited to join the study. Only those who were receiving hemodialysis for at least 3 years were included. Patients who were able to give informed consent irrespective of their gender were asked to fill a structured study questionnaire and to complete multiple psychosocial tools. Patients under 18 years of age and those who were not able to answer the questionnaire or psychosocial tools (such as those with blindness, deafness, or severe dementia) were excluded. Out of 165 invited, 101 completed the study (response rate 61.2%).
Data collection
A structured study questionnaire was used in data collection covering sociodemographic characteristics, hemodialysis-related characteristics, comorbidity, and psychiatric history (supplementary material-1). Additionally, a number of validated psychological tools has been used to assess exposures and outcomes of the study (supplementary material-2).
Exposure and outcome definitions
Exposure measures included psychological tools: the 9-item patient health questionnaire (PHQ-9), hospital anxiety and depression (HAD) scale, experience in close relationships scale (ECR-M16), Montreal cognitive assessment (MoCA), and the patient health questionnaire-physical symptoms (PHQ-15).22-29 The outcome was assessed by QoL index covering 4 domains: health and functioning, socioeconomic, psychological/spiritual, and family domains.30,31 The details of each tool including the cut points for the diagnosis are shown in supplementary material.
Statistical analysis
The data was presented as frequencies and percentages for categorical variables and means and standard deviations (SDs) for continuous variables. Significant differences in QoL index between groups defined by demographics, clinical characteristics, comorbidity, and psychosocial tools were tested using the Mann-Whitney test (for 2-level variables) and Kruskal-Wallis test (for variables with more than 2 levels). Correlations between QoL index and the continuous version of the psychological measures were tested using Spearman correlation. Multivariate stepwise linear regression model was run to detect potential predictors for higher level of QoL index. The model included all variables associated with the overall QoL index (p<0.05 or p<0.010) in univariate analysis. All p-values were 2-tailed. A p-value<0.05 was considered significant. The Statistical Package for the Social Science (SPSS), version 23.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
Results
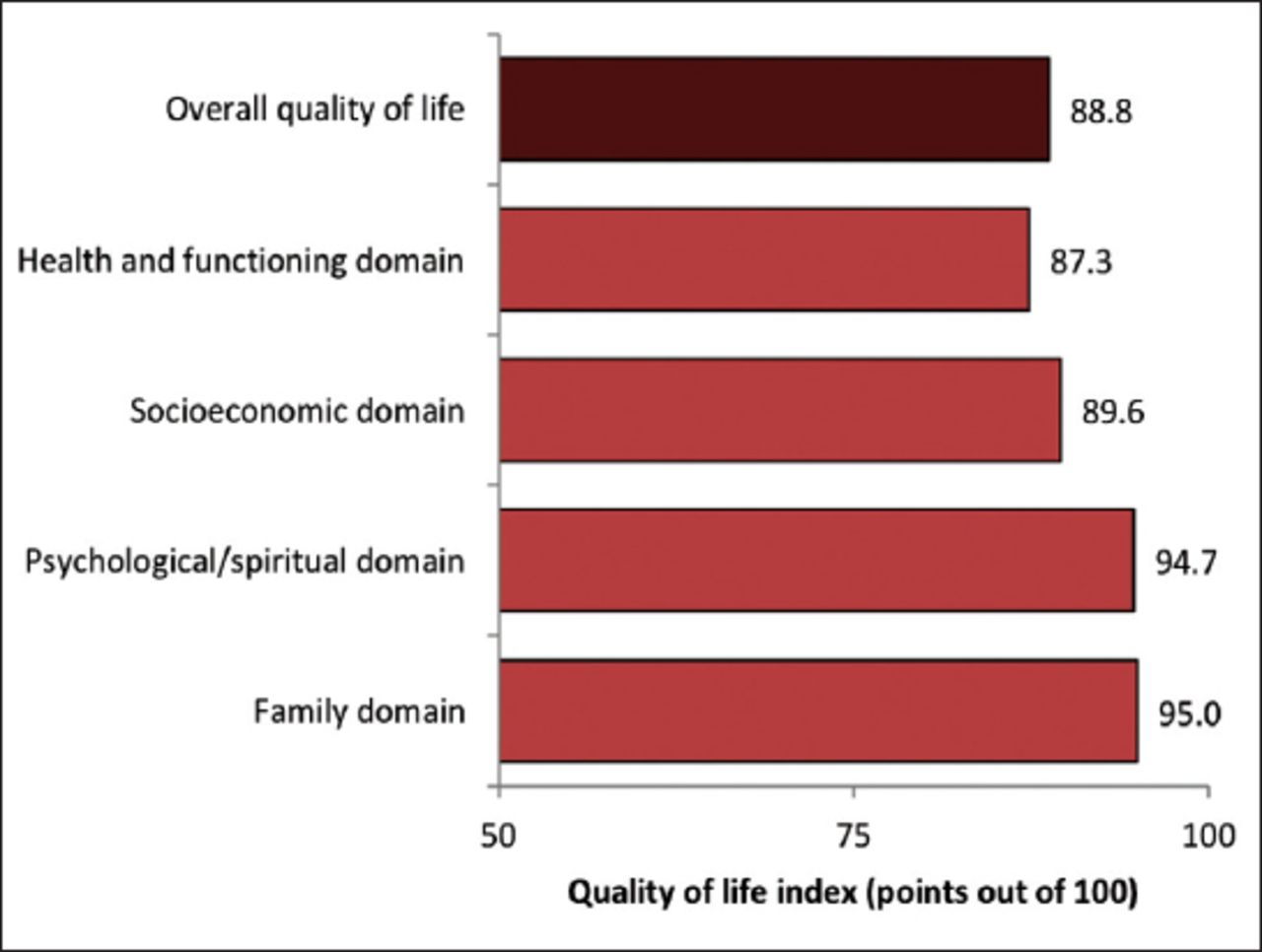
The current analysis included a total of 101 patients (56 males and 45 females). The overall mean QoL index was 88.8/100 points (out of 100). More details about the scores of different domains of QoL are shown in Figure 1. The mean age was 54.0±12.3 years, and 55.4% were males. Two-thirds (67.3%) of patients were currently married, and they had a mean of 5.2±3.1 children. The majority (96.0%) of the patients were Saudi, 59.4% had less than secondary education, 26.0% were working, and only 15.2% had a family income greater than SR10,000. Of the demographic characteristics, being older ≥60 years (p=0.020), being married (p=0.036), and being housewives (p=0.009) were significantly associated with higher level of overall QoL index. More details about demographic characteristics are shown in Table 1.

Overall and domains of quality of life among chronic hemodialysis patients using the quality of life index (dialysis version-III).
Demographic characteristics of the chronic hemodialysis patients by the quality of life index.
Approximately 62.4% of the patients were aware of the medical causes of their renal failure. Some patients believed that psychological stress (20.8%) and nonmedical causes such as evil eye/possession/black magic (30.7%) could be a reason for their renal failure. The mean duration of hemodialysis was 9.9±6.8 years. Approximately one-fourth (26.7%) of the patients were using alternative medicine, such as herbs (63%), religious ruqyah (55.6%), and cauterization (7.4%). The vast majority of the patients were satisfied with hemodialysis services provided by their center. The majority (73.7%) of the patients reported receiving support from their families or friends, and only 23.8% had problems getting to the hemodialysis unit. Of the dialysis-related characteristics, only longer duration of hemodialysis was significantly associated with lower level of overall QoL index (p=0.027). More details about dialysis-related characteristics are shown in Table 2.
Hemodialysis-related characteristics of the study participants by the quality of life index.
The majority (90.1%) of the patients had comorbidity; with 38.5% of them suffer from 3 or more diseases. Only 3.0% of the patients reported having psychiatric disorders before the diagnosis of renal failure. Only 6.9% were regularly seeing a psychiatrist. Approximately 10.9% of the patients received a diagnosis of psychiatric disorders after the diagnosis of renal failure. Higher numbers of comorbidities (p=0.004), specifically cardiovascular disease (p=0.041) and hepatitis B (p=0.030) and hepatitis C (p=0.014), were significantly associated with lower level of overall QoL index. More details about medical and psychological comorbidities are shown in Table 3.
Medical and psychological comorbidity of the chronic hemodialysis patients by the quality of life index.
The mean PHQ-9 score was 6.30±5.50, with 24.8% of the patients having depressive symptoms. The mean HAD anxiety score was 3.28±3.97 and depression score was 4.06±3.91, with 15.8% of the patients having anxiety and 19.8% of them having depressive symptoms. The mean ECR-M16 score was 3.38±1.42 for anxiety and 2.73±1.21 for avoidance, with 76.8% of the patients considered insecure. The mean MoCA cognitive function was 16.84±7.63, with 88.1% of the patients having cognitive impairment (that is MoCA is less than 26 out of 30). The mean PHQ-15 score was 7.97±5.33, with 38.6% of the patients having medium/high severity of somatic symptoms. All the above scores were significantly and negatively correlated with the level of overall QoL index (r ranged between -0.228- -0.468). Patients who were not cognitively impaired were more negatively affected in QOL. More details about psychosocial examinations by the QoL index are shown in Table 4.
Psychiatric examinations among the chronic hemodialysis patients by the quality of life index.
After adjusting for all the variables associated with overall QoL index, only the HAD anxiety score, MoCA score, and marital status were independent predictors of overall QoL index (Table 5). For each increase of one standard deviation in the HAD anxiety score and MoCA score (that is better cognition), there was an overall QoL index decrease of HAD anxiety score 0.425 and MoCA score 0.301 standard deviations. On the other hand, overall QoL index was 0.309 standard deviations higher in married patients than in non-married patients.
Multivariate linear regression analysis for potential predictors of a higher quality of life index* among chronic hemodialysis patients.
Discussion
The current study showed high levels of overall QoL among patients receiving hemodialysis at 3 centers in Riyadh, KSA. The QoL index tool used in the current study measured patient-perceived subjective QoL, while most of the previous studies among chronic dialysis patients focused on health-related QoL.13 While it is challenging to compare QoL measured using different tools in populations with different demographic and clinical characteristics, the current level of QoL appeared to be higher than those previously reported for chronic hemodialysis patients in KSA.15,16 Additionally, the current level of QoL was generally higher (88%) than those previously reported using the same tool with chronic hemodialysis patients in the United Arab Emirates (77%), Jordan (67%), and Iran (68%).32-34 Interestingly, the results of these studies followed the same pattern observed in the current study, where family and psychological/spiritual domains received the highest domain scores. Researchers have reported that the conservative culture in KSA, characterized by strong family bonds, social support, and religious beliefs, positively impacts QoL in chronic dialysis patients.16,35
The burden of ESRD disease and its management reportedly increase the risk of stress and psychosocial disorders.36 The chronic hemodialysis patients in the current study generally had a better than expected psychosocial profile, which may have contributed to the high QoL level observed in the current study. Approximately 20-25% of these patients had depressive symptoms, and 16% had anxiety symptoms. These figures are considerably lower than those previously reported for chronic hemodialysis patients in KSA.18,37,38 For example, using HAD scores of ≥8, 45-52% of chronic hemodialysis patients in Makkah and Al-Madinah, KSA, had depressive symptoms, and 40-42% had anxiety symptoms.18,37 Actually, the current figures for depressive and anxiety symptoms are similar to the levels described in primary care patients in KSA.39,40 The majority of current patients were very satisfied with both the hemodialysis care provided and the social and logistic support received. Additionally, religious and cultural beliefs among chronic hemodialysis patients in KSA positively impact overall psychological functioning.35 These beliefs can change the way the patient perceives the suffering and hardship associated with the disease and the commitment to its management.41
Although most of the current patients had impaired cognitive function, it is still better than previously reported.20,42 For example, the chronic hemodialysis patients examined in Jeddah, KSA, had >35 out of 36 points on the blessed dementia information memory concentration test, with almost all patients having cognitive impairment.42 Cognitive impairment has been linked to aging, depression, and stroke.43,44 Current patients were relatively young, had a very low stroke burden (2%) and had a lower than expected level of depressive symptoms. Almost three-fourths of the current patients had an insecure attachment style. This was probably a result of higher anxiety symptoms (3.4 points) rather than avoidance (2.7 points). It is difficult to compare this finding, as we could not identify local or international studies estimating attachment style in chronic hemodialysis patients. Finally, approximately 40% of the current patients reported medium to high severity of somatic symptoms. While this result is probably expected in chronic hemodialysis patients with multiple comorbidities, we could not identify local studies estimating the severity of somatic symptoms in chronic hemodialysis patients in KSA. Consistent with this finding, the lowest QoL score for the current patients was in the health and functioning domain. Nevertheless, the severity of somatic symptoms in the current study was very similar to that for Saudi patients with diabetes.45
With exception of cognitive impairment, the scores of all psychosocial disorders examined in the current study were negatively correlated with QoL in univariate analysis. These included depressive and anxiety symptoms, insecure attachment style, and severe somatic symptoms. Other studies report similar findings for chronic dialysis patients internationally, especially for depression, anxiety, and stress.12-14 We could not identify any local studies focusing on the impact of psychosocial disorders on QoL among chronic hemodialysis patients in KSA. However, psychosocial disorders, especially depressive and anxiety symptoms, were associated with poor QoL among patients with diabetes, skin disease, and sickle cell disease.45-47
Anxiety symptoms and cognition level (better cognition) in the current study remained negatively associated with QoL in multivariate analysis. Consistently, in a review of 5 studies that examined the role of both anxiety and depression on QoL, anxiety alone was an independent predictor of QoL in 2 studies, both anxiety and depression were independent predictors in 2 studies, and depression alone was an independent predictor in one study.12 The disappearance of depressive symptoms in the multivariate analysis in the current study may be related to its strong correlation with anxiety symptoms (r=0.577, p<0.001). Several studies pointed to the negative impact of anxiety on psychosocial functioning in several functional domains.48 Additionally, anxiety is prone to affect the mental health dimensions of health-related QoL.12 Unlike the majority of the studies, patients who were not cognitively impaired were more negatively affected in QOL.13,48 Consistent with this finding, some studies found that normal cognition may increase the negative impact of comorbidity on QOL.49 It is not clear why the presence of cognitive impairment was associated with less negative impact on QOL, despite, it would be expected that given better cognition is associated with better self-care, however there is a possibility that cognitive impairment may reduce insight.
With the exception of marital status, the sociodemographic and clinical characteristics of the current patients did not play a major role in QoL. The positive role of marital status could relate to the caregiver role of the partner. Additionally, married chronic hemodialysis patients tend to perform better in physical QoL scores.50 However, local studies among chronic hemodialysis patients could not detect any significant impact of marital status.15,16 Studies that examined the role of psychosocial factors in QoL using multivariate analysis could not detect major roles for sociodemographic and clinical characteristics.32,51,52
The current study examined the associations of psychosocial predictors with QoL in chronic hemodialysis patients. The study methodology involved the examination of patients from 3 centers using multiple validated psychosocial tools, and the use of multivariate analysis.
Study limitations
A number of limitations can be recognized. The cross-sectional design cannot confirm causal association between psychosocial predictors and QoL. The convenience sampling may hinder the generalization of the current findings to all chronic hemodialysis patients in KSA. The lack of local studies compromised the ability to compare some findings such as attachment style and severity of somatic symptoms. However, the findings provide an opportunity for researchers to confirm or reject them in the future. The use of multiple psychological tools may negatively impact the enthusiasm and accuracy of the patient response. However, as they have been adjusted for in the multivariate analysis, the impact on the findings should be minimal.
In conclusion, we report a high overall QoL and relatively better psychosocial profiles among patients receiving hemodialysis in Riyadh, KSA. Psychosocial disorders were negatively correlated with QoL in univariate analysis. Also, patients who were not cognitively impaired were more negatively affected in QOL. Anxiety symptoms and better cognition level remained negatively associated with QoL in multivariate analysis. The findings of the current study re-emphasize the importance of the early detection and management of psychosocial disorders in chronic hemodialysis patients to improve QoL.
Acknowledgment
The authors gratefully acknowledge the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia for supporting this study. Furthermore, the authors express their gratitude to Dr. Aiman El-Saed for his assistance in data analysis.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 22, 2020.
- Accepted July 23, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.