


Abstract
Objectives: To describe radiographic imaging findings and disease course in admitted Coronavirus disease 2019 (COVID-19) patients.
Methods: This retrospective study was carried in the Radiology Department, King Fahad Military Medical Complex, Dhahran between March to August 2020 (6 months). All laboratory confirmed COVID-19 admitted cases were evaluated for their symptoms, duration of hospital stays (in a ward or intensive care unit [ICU]), and imaging findings (ground-glass opacity [GGO], air-space shadowing/consolidation, and others such as atelectasis, reticulation, peribronchovascular thickening, lymphadenopathy and pleural effusion) on chest radiograph (CXR) and computed tomography (CT) studies. Cavitation, nodularity, bronchiectasis, and embolism detected on CT scans were considered as complications. Disease course in terms of recovery (radiographic regression or resolution of findings), worsening (shifting from ward to ICU), and unfavorable outcome (persistent ICU stay or death) were recorded. Imaging findings were interpreted by 2 experienced radiologists and consensus reporting was made. Chi-square test was used to determine association.
Results: Out of 106 patients, majority were males (n=82, 77.4%). Forty-six patients (43.3%) had abnormal imaging with mostly peripheral GGO (56.5%), followed by consolidations (34.7%), and others (26%). Complications were detected in 6 ICU patients. All patients with unfavorable outcomes were above 60 years having comorbidities or complications (p<0.0005). Fatality rate was calculated as 2.8.
Conclusion: Coronavirus disease 2019 is seen mostly affecting males, with peripheral opacities as common imaging findings. Elderly patients with co-morbidities may show unfavorable outcomes.
Coronavirus disease 2019 (COVID-19), a global pandemic declared by the World Health Organization (WHO) in March 11, 2020, for a lower respiratory tract illness of unknown origin that started as an outbreak in Wuhan City, China in December 2019, was found to be a novel strain of corona virus as determined on bronchoalveolar lavage of the affected patients.1,2 The disease is still prevalent in many parts of the world, greatly affecting not only the healthcare systems but also severely impacting on world’s economy and behaviors of mankind. A low to moderate (estimated 2-5%) mortality rate and incubation period between 2-14 days, statistics show variable epidemiology, individual response and severity of infection in different regions of world.1,3-5
Rapid detection and early laboratory diagnosis of COVID-19 remain crucial for both control and treatment of disease. Real-time reverse transcription-polymerase chain reaction assay is the choice of molecular test for confirmation of COVID-19, but serological tests (ELISA) are widely used to identify higher risk population.6,7 COVID-19 patients have high virus loads in their upper and lower respiratory tracts. Therefore, swabs from nasopharynx or oropharynx are recommended for screening or detection of disease. Sputum sampling or bronchoalveolar lavage can also be used for collecting lower respiratory tract specimens. However, adequate sample at correct time and correct site is necessary for prompt diagnosis, and tests can be falsely negative if swabs or samples are not properly taken. Molecular testing can also be affected by improper sample storage and transport media.7 Immunoassays have also been developed; however, antigen detection may be missed in cases due to timing (tested too soon), low infectious burden or sampling variability. Once infected and cured or recovered, herd immunity can develop in population, and serological and PCR tests can remain positive.8-10
Pulmonary manifestations for other strains of coronavirus family namely the SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome) have been recognized; however, imaging features were variable and non-specific.11 Although COVID-19 has shown to have better genome sequence identity with SARS-CoV compared to MERS-CoV, imaging features of COVID-19 were also initially reported as non-specific.12 However, chest computed tomography (CT) has shown to have moderate sensitivity and high specificity in differentiating COVID-19 pneumonia from other viral pneumonia.13 Radiologists from all parts of the world are sharing their experiences and trying to characterize the imaging features to better understand disease course and severity in combating the outbreak.12-15 We also aim to describe chest x-ray (CXR) and CT findings with disease course in COVID-19 positive hospitalized patients requiring intensive care unit (ICU) admissions at our hospital.
Methods
All adult laboratory confirmed COVID-19 patients who were admitted (with categories mild to moderate, severe or critical based on clinical and laboratory criteria) under guidelines set by Ministry of Health, Saudi Arabia and Saudi Centre of Disease Prevention and Control through out-patient departments, employee health clinics, and emergency during a period of 6 months between March to August 2020 were enrolled in the study. Pregnant patients, pediatric age group and patients (who were asymptomatic or with mild symptoms) referred for quarantine centers or home isolations were excluded. Age, gender, nationalities (Saudi, non-Saudi), and socioeconomic statuses were recorded. Presence of any co-morbidities (like diabetes, hypertension, heart disease, obesity, asthma) were documented. Clinical information was obtained from patients’ files or charts using hospital information system and magnetic resonance imaging findings were retrieved from radiology information system/picture archiving and communication system. Research protocol was approved from the Hospital Ethic Committee and need for informed written consents for the study was waived off considering retrospective nature of the study, and non-disclosure of patients’ information. All information was kept strictly confidential. The research was conducted in accordance with the Helsinki Declaration.
Chest radiographic findings at the time of Hospital admissions, during their hospital stays (in wards and ICU) and CT findings (if performed) were documented. Chest radiographic appearance (either normal or abnormal) at the time of admissions, and duration of illnesses (from onset of symptoms to radiographic abnormalities) were also recorded. Any central, perihilar or peripheral upper, mid or lower zone patchy shadowing, infiltrate or consolidations were considered under abnormal chest radiographs. Additional (or other) findings like increased reticulation, peribronchovascular thickening, pleural effusion/pleural thickening and lymphadenopathy were documented. Cavitation or pleural effusions were also noted. Computed tomography findings were recorded as single, multifocal, or diffuse air-space opacities (ground-glass opacity/GGO, consolidation or both), unilateral or bilateral lung involvement, zonal distributions (upper, mid, or lower zone) and other findings (like atelectasis, increased reticulation, peribronchovascular thickening, lymphadenopathy, pleural effusion) were also documented. Cavitation, bronchiectasis, nodule or mass, and pulmonary embolism as detected on CT scans were considered as complications. Disease course and outcomes in terms of regression or resolution (leading to recovery), persistence or progressive worsening of disease (leading to death) were also recorded, in addition to duration of ICU stays for these patients. Two radiologists interpreted radiographic findings, and consensus reporting was made for final documentation. Radiographic (chest radiographic or CT) findings were compared with disease course, ward outcome (either recovered and discharged, or shifted to ICU due to worsening of condition) or ICU outcome (such as, recovery or persistent stay/death).
Statistical analysis
The statistical analysis was carried out using Statistical Package for Social Sciences for Windows, version 22 (IBM Corp, Armonk, NY, USA). Chi square test was used to determine association. A p-value less than 0.05 was considered significant.
Results
A total of 166 laboratory confirmed COVID-19 positive patients were admitted in our hospital in 6 months interval, with mean age of 50.62 (33 to 71 years, standard diviation [SD]=10.7). Out of 106 patients, majority were males (n=82, 77.4%) while rest (n=24, 22.6%) were females. Nearly half of the patients presented with fever, cough, or sore throat (n=52, 49%) while remaining half by shortness of breath, body aches/myalgias or other abdominal symptoms. Mean duration between symptoms and presentation/admission was approximately 3.5 days (range, 1-6, SD, 1.2). Forty six patients (46/106, 43.3%) had abnormal chest radiographs on admissions or developed during the course of stay in the ward, with mostly unilateral or bilateral peripheral opacities (26/46, 56.5%), followed by consolidations (16/46, 34.7%) and others (12/46, 26%) (Figures 1 & 2).
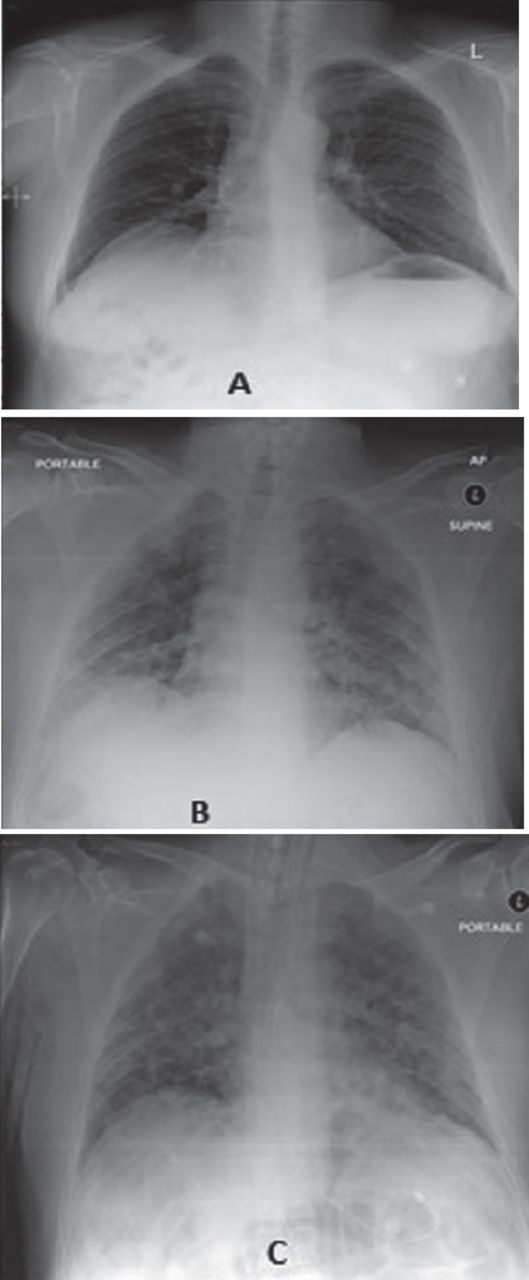
Radiographic disease course as seen on serial chest radiographs of a COVID-19 admitted patient in the ward. A) Initial and B & C) subsequent chest radiographs of COVID-19 patient showing subtle peripheral opacities and increased reticulation that became more prominent during ward stay. Duration between chest x-ray A and B is 9 days and between B and C is 4 days.

Chest radiographic findings in a COVID-19 patient with ward and subsequent ICU stays and recovery. A) Initial and B-D) serial chest radiographs showed mixed changes of peripheral opacities and consolidations affecting both the C) lungs at mid and lower zones that regressed and D) improved during ICU stay.
Most of patients (42/54) who presented with shortness of breath or body aches were having abnormal chest radiographs at presentations/admissions, while most of patients with fever, cough or sore-throats (48/52) had normal chest radiographs (χ2=26.49, p=0.0005). Similarly, patients with shortness of breath and abnormal initial or serial chest radiographs/CTs (46/54) had ICU admissions, with p-value 0.0005 (χ2=25.88).
Age, gender, nationalities, and socioeconomic statuses were not seen having statistically significant associations with chest or CT abnormalities. However, advancing age (60 years and above) was seen associated with ICU outcome, with 6 out of 18 had unfavorable outcome versus all remaining under 60 years had recoveries (χ2=14.58, p=0.0054).
Nearly a third of patients (34/106, 32%) were shifted to ICU for worsening clinical, laboratory or chest radiographic findings. Out of these, 24 patients showed improvement and later shifted to wards with an average ICU stay of approximately 7 days (5-12 days). Thirty-six patients (36/106, 34%) were having comorbidities. Comorbidities were seen associated with ICU outcomes (Table 1). Six patients with comorbids and immunocompromised statuses had complications (pulmonary embolism, cavitation, and bronchiectasis) that remained intubated with persistent stays in the ICU. Three deaths were recorded during the study period.
Comorbidities and outcomes.
Computed tomography of the chests (contrast enhanced studies or high resolution computed tomography/ HRCT) were performed between 3 to 7 days of admissions (mean=5.4 days) in nearly half of patients (n=22/46) having abnormal chest radiographs. In addition to presence of GGO or consolidations in all CT studies, other findings included atelectases (n=6), increased reticulation or peribronchovascular thickening (n=5), pleural effusion (n=3), lymphadenopathy (n=2) and complications (n=6). Abnormalities on serial radiographs and CTs were mostly found to be unilateral or bilateral, peripheral, mid or lower lobe ground-glass opacities (36/56, 64.2%), with mixed changes (of GGO and consolidations) in 14 patients (25%), and perihilar consolidations in 6 patients (Table 2). Eight patients with initial normal radiographs were having unilateral lower lobe peripheral GGOs. Worsening radiographic findings (Figure 3) were seen to be significantly associated with both ward and ICU outcomes (Table 3), with p=0.0005 (χ2=24.10).
Radiographic findings during ward and intensive care unit admissions.
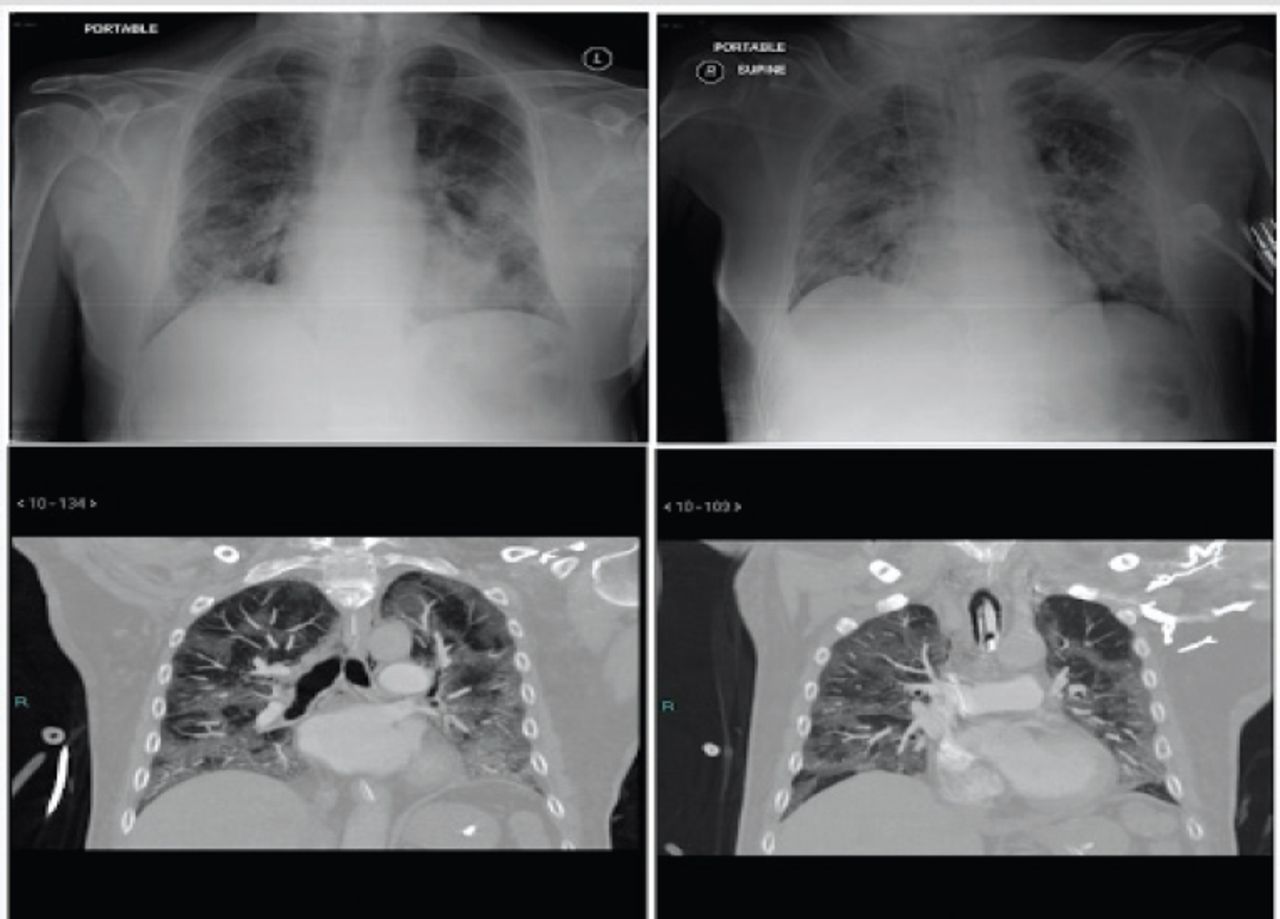
Worsening disease course and imaging findings in a complicated case of COVID-19. Chest radiographs (upper row) showed dense opacities at mid and lower zones in both lungs. Selected coronal CT chest images (bottom row) showed extensive bilateral GGOs with interlobular septal thickening. Patient developed pulmonary embolism and remained in ICU with unfavorable outcome.
Radiographic findings and outcomes.
Discussion
Most of our study results pertaining to patterns of radiographic findings on both chest radiographs and CTs matched with international observations.13-16 We found patterns of single or multiple single lobar GGO with or without consolidations on serial CXRs and CTs in most of the patients at the time of admission and during their ward stays, that later became multi-lobar, mixed, and bilateral during worsening disease course leading to ICU admissions. These patterns were seen associated with increased reticulation and pleural effusions probably because of element of respiratory failure or superimposed cardiac decompensation. Patients who recovered from ICU and shifted back to ward (and later on discharged), ICU stays were approximately 5-12 days, while for the 6 patients who had prolonged ICU stays 3 died and 3 remained intubated with unknown outcome till end of study. On chest x-rays, single or multiple unilateral or bilateral opacities were seen at the time of ICU admissions in some patients, mainly at mid and lower zones. Shi et al14 categorized 81 admitted COVID-19 positive patients in 4 groups according to duration of onset of symptoms and timings of CTs, with consolidations and mixed patterns more frequent in group 3 (>1 week to 2 weeks) and group 4 (>2 weeks to 3 weeks). In our study, most of the patients fall in the group 3 category as patients who needed ICU stays developed worsening of symptoms or appearance of chest radiographic findings in a short period, warranting CTs to be performed in less than 2 weeks intervals. Lomoro et al15 found typical CT features of bilateral multi-lobar GGO with peripheral distribution in approximately 60% of 58 laboratory confirmed COVID-19 cases in their single-center retrospective study. Although we did not include pregnant patients, such kind of mixed or complete consolidations were also observed by Liu et al12 while observing data of 16 COVID-19 positive pregnant patients and comparing these with 14 non-pregnant positive patients. Bai et al13 found that while considering CT findings of peripherally distributed GGOs, fine reticular opacity, and vascular thickenings in a study that reviewed 424 CT interpretations of 205 patients from 7 Chinese hospitals, radiologists were able to distinguish COVID-19 from other viral pneumonias with high specificity and moderate sensitivity.
Another important aspect to highlight in our study were patients’ characteristics, the age and gender. We found males to be more affected than females, and middle-aged group (40-60 years) showing variable and at times devastating worsening of symptoms or chest radiographic abnormalities leading to ICU admissions. However, this group recovered from ICU care. Although, advanced age (of 60 years and above) and with co-morbidities or immunocompromised statues were the ones who had prolonged ICU stays and unknown outcomes (with persistent intubations and no favorable signs of recoveries). These are the patients who are amongst the vulnerable group of any pandemic, other being the paediatric population that was not included in our study.6 Concept of ‘herd immunity’ stems from the effects of individual immunity scaled to the level of the population (referring to the indirect protection from infection conferred to susceptible individuals when a sufficiently large proportion of immune individuals exist in a population). Therefore, vaccination programs aim to establish this herd immunity so that those who cannot be vaccinated, including the young and immunocompromised, are still protected against disease.8,9 One important measure to evaluate the impact of disease spread is the case fatality rate (CFR), that is the proportion of deaths attributed to a certain disease among all individuals diagnosed with that disease over a specified period. Although fatality rate in our study measured 2.8%; however, it seems not an accurate figure as some death cases might be left unchecked or might not get hospital admissions. It is worth noting that there is still significant uncertainty in the CFR for COVID-19 due to variation in the testing capacity of each country, selection bias for individual testing, and officially attributed deaths to COVID-19. Case fatality rate is also sensitive to variation in age and presence of comorbidities among populations. Consequently, CFRs may differ considerably over time and between countries. Like many other infectious diseases, a non-uniform COVID-19 CFR has been reported across age groups, with many deaths occurring among individuals 60 years old or greater.9,10
We also found that more than half of the patients were non-Saudis (expatriates) and those too amongst the low socioeconomic statuses (workers; drivers, mechanics, housekeeping). This finding though not statistically significant however, emphasizes on clinical relevance of such group being affected more or earlier probably due to their shared livings or accommodations, social lifestyles and close contacts or environmental interactions because of job requirements. Corona virus typically spreads via droplets when people are in sustained, proximity to someone sick.17 Studies have shown that factors that increase risk of catching the corona virus are enclosed or congested spaces, crowds, close contact with others, and difficulty social distancing.18,19 It is wise to suggest that more close interactions with others, the longer the interactions, and greater the number of people involved in interactions, the higher the risk of COVID-19 spread. Three Cs, referring to closed spaces, crowded places, and close-contact settings need to be avoided.
It is also worth mentioning that although CT chest has high sensitivity to detect Covid-19 lung changes.20,21 However, its role as a screening tool is still debated and is usually reserved for documentation of complications (cavitation, bronchiectasis, pulmonary embolism, and pneumothoraces) if clinically suspected. Routine chest radiographs can provide useful information to check for disease course particularly with mild disease or resolving changes. Also, portable radiography of the chest may be considered for serious patients at bedside rather engaging them for CT scans that require both meticulous care for patient shifting as well as preparation at the scanner and fumigation after the scanning, thereby interrupting diagnostic assessments for other scheduled or booked cases in limited machine settings and hospitals. In our study, we also reserved CT chests for only patients with unfavorable clinical course or worsening of symptoms and to document any complications. We did not include paediatric patients in our study, however, it is also worth stating that CT features may be have different common pattern in paediatric age group like consolidation with surrounding halo sign as presented by Xia et al.22 Other limitations of our study included lack of documentation of clinical and laboratory variables (like oxygen saturation, C-reactive protein, lactic acid dehydrogenase levels, D-dimers, lymphopenia), and ongoing medications (or treatment options) that could have detected or predicted the course of disease or complications.
In our single-center short-duration study, we focused on certain demographic information of patients and radiographic findings/patterns to look for clinical course of disease and its outcome. No quantitative lobe score was obtained for imaging findings.Patients with initial presentations as shortness of breaths, comorbidities, abnormal chest radiographs (on admissions and during ward stays), and mixed radiographic findings on CT studies required ICU admissions (highlighting CT utilization during course of infection).23 However, larger scale and longer duration multi-center studies are required to validate such findings with special consideration of prognostic relevance of certain clinical and laboratory parameters (and even certain blood groups). Further research is needed to evaluate for duration of acquired immunity after natural infection in such patients, and clinical utility of antibodies (in plasmas of affected cases) for the treatment of unaffected population and for the vaccine preparation.24 Also, follow-up of COVID-19 recovered ICU patients (who required intubations during their stays) should not be overlooked and dealt with great clinical concern. Proper evaluation and attention needs to be considered in future studies, as COVID-related lung fibrosis (idiopathic pulmonary fibrosis) can develop in such patients due to increased vulnerability towards alveolar injury because of both viral affects and barotrauma leading to even life-time dependency for oxygen. Future considerations in terms of assessment of risk factors and treatment options (antiviral, immunomodulatory, and anti-inflammatory drugs) to avoid such complications need to be emphasized.
With no vaccine yet available for general masses and many countries are striving to develop promising vaccine results for prevention of COVID-19, herd immunity largely depends upon contracting the disease and developing antibodies (natural immunization) which itself is a slow process considering worldwide lockdowns or curfews, restricted travel, and limited social gatherings.2,8,9 Using personal protective measures (like face masks, face-shields, gloves and gowns), practicing frequent hand hygiene (hand washing or hand-rub using use of hand sanitizers) and social distancing (avoiding close contacts, social gatherings or crowded places) remain the choices to limit widespread human-to-human transmission (through droplets, contaminated hands or surfaces) and disease-spread, meanwhile moving forward and adopting to a new-normal.5 With its variable clinical course and disease presentation, COVID-19 remains an unanticipated threat lurking in communities and hospitals, clogging the healthcare systems in nearly all over the world.8
Although many of our study observations are similar to international studies, presenting local data and results is important to add information to global network. This does not only help to identify any regional variability in disease presentation or course due to possible emergence of different virus strains affecting different populations (as more recent studies are indicating emergence of genetic drift and mutations in genome of virus that may affect surges in infected population and also can hinder or limit effectiveness of vaccine),25 but also provides an opportunity to establish unified or consensus-based international guidelines and policies (once similar virus trend across the globe has been found and documented through world-wide studies).
In conclusion, COVID-19 is seen mostly affecting males, with less than half of symptomatic admitted patients showing abnormal chest radiographic findings as peripheral opacities on chest radiographs at or during their admissions while demonstrating mostly GGOs (with or without consolidations) on CT studies. Most of the young and middle aged patients requiring ICU admissions recover however elderly patients with co-morbidities or immunocompromised statuses, worsening radiographic findings or complications may show unfavorable outcomes (such as, prolonged ICU stays or deaths).
Acknowledgment
We gratefully acknowledge Dr. Muhammad Z. Ul Hassan for providing his assistance in reviewing the submitted figures for clarity and correctness. We would like to thank American Manuscript Editors for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 7, 2020.
- Accepted December 14, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.