


Abstract
Objectives: To assessed the current practices for the management of thyroid nodules in the Gulf Cooperation Council (GCC) Countries.
Methods: We conducted a descriptive web-based survey to physicians and surgeons involved in the management of thyroid nodules. The survey included questions on referral, ultrasound (US) reporting, fine needle aspiration (FNA), management of thyroid nodules including the approach for indeterminate FNA results, and usage of molecular testing.
Results: A total of 311 responders, 155 (49.8%) were endocrinologists. Results showed that referrals and US report lack a number of valuable information including family history (84.9%) and high-risk US features (92.9%). Approximately 263 (84.6%) preferred to include a scoring system or protocol to assess the nodule risk in US report. Approximately 193 (62.1%) sent the patient to interventional radiologists for FNA. Almost half (n=147, 47.3%) repeat the FNA in 2-3 months if the FNA result was a follicular lesion or atypia of undetermined significance and 142 (45.7%) opted for lobectomy for follicular neoplasm or suspicious of follicular neoplasm result. Only 44 (14.1%) performed molecular testing; however, 174 (55.9%) preferred it available. Significant variations in the approach were seen between endocrinologists versus non-endocrinologists.
Conclusion: Practices variation in the management of thyroid nodules mandate a common practical guideline. Molecular testing is a preferable test for indeterminate FNA results by most of the responders though it is not widely available.
Thyroid nodules are common and many patients are seen, referred and managed worldwide.1,2 What concerns endocrinologists is the propensity of thyroid nodules to become malignant. There was an increase in the incidence of thyroid cancer because of the advancement in diagnostic modalities which include the use of neck ultrasound, fine needle aspiration (FNA), and other anatomic imaging modalities.3-5 These diagnostic modalities became more available and more sensitive in detecting even small thyroid nodules. In addition, the molecular profiling of cytologically indeterminate thyroid nodules has made the diagnosis of thyroid nodules far more better.6-10 In 2012, thyroid cancer represented 13.2% of cancers among women in Saudi Arabia, next to breast cancer.11
In 2015, the American Thyroid Association (ATA) published the updated clinical practice guidelines for the management of thyroid nodules; however, it was not clear on how this clinical practice guidelines differed from what doctors actually practice.12-14 Several reports have noted that the 2015 guideline has a restricted approach to tissue sampling while others had distinguished its benefit in terms of quality, cost, and availability.11,15,16
The management of thyroid nodules starts with a referral from a general practitioner to a family medicine practitioner, an internal medicine specialist, or an endocrinologist, and sometimes to an ear, nose, and throat (ENT) specialist or a general or endocrine surgeon. If the patient is less than 12 years old, the referral goes to an endocrine pediatrician. Along this course, the referral may encounter some problems, including insufficient information, incomplete laboratory and radiology tests, differences between hospitals in FNA results, and many others. In this regard, we wanted to identify issues and problems encountered by physicians involved in the management of thyroid nodules, with the hope of creating a management protocol and finding solutions to improve not only the referral system but the entire management process. Therefore, this study was conducted to determine current practices regarding FNA and management of indeterminant FNA results, assess the referral system for a thyroid nodule finding and the interdisciplinary approach, and provide recommendations, including the use of molecular testing.
Methods
We conducted a web-based survey sent electronically as a Google document to all physicians and surgeons in Gulf Cooperation Council (GCC) countries who were involved in the management of thyroid nodules between June and July 2020. All physicians and surgeons who were involved in the management of thyroid nodules were included in the study. Those who refused to participate in the study were excluded. The study was conducted at King Saud University Medical City, Riyadh, Saudi Arabia, as the base setting and was approved by the Institutional Review Board of the College of Medicine, King Saud University, Riyadh. All participants provided their informed consent on the use of the data of their input to the questionnaire.
We searched the web including Google Scholar and Pubmed for prior literatures related to the research to frame our survey form. The survey form included 20 questions divided into 5 sections: i) demographic information (specialty, gender, age, and years of experience), ii) referral of thyroid nodules, iii) questions on the use of FNA and its performance, iv) current approach to indeterminate FNA results and the need for molecular testing, and v) referral to surgery and preferred specialties. The survey questionnaire was developed by the author and was validated among 15 respondents where the questionnaire was administered to the same 15 participants after 1 week. Test-retest correlation coefficient (r) was good at 0.85.
The sample size of survey participants was calculated by the formula
ss = Z2 * (p) * (1-p)/c2
where Z = Z value (for example 1.96 for 95% confidence level), p = percentage picking a choice (15%), and c is the confidence interval (0.5). The calculated sample size was 196 participants. Data were presented as mean and standard deviation for continuous variables and percentage distribution for categorical variables. An independent t-test was used to determine the significance of differences between continuous, normally distributed variables, and the Chi-square test was used for categorical data. The significance of differences in the proportion of responses between endocrinologists and non-endocrinologists was determined using the Z test of proportions. A p-value <0.05 was considered to indicate statistical significance. The data were analyzed using the Statistical Package for Social Sciences (SPSS) version 23.0 for Windows (IBM Corp., SPSS, Armonk, NY, USA).
Results
The survey was sent electronically to 450 physicians and surgeons who were involved in the management of thyroid nodules. A total of 311 physicians responded to the survey; 178 (57.2%) were men and 133 (42.8%) were women, and 155 (49.8%) of respondents were endocrinologists. Response rate was 69.1%. Table 1 shows the detailed demographic profiles of the respondents.
Demographic profiles of survey respondents.
A large percentage of the respondents (n=264, 84.9%) thought that the referrals lacked information on family history of thyroid cancer, and 229 (73.6%) thought that the referrals lacked details on the growth rate (progression) of the nodule. Majority of the respondents (n=289, 92.9%) thought that the thyroid and neck US report should include the high-risk features of the thyroid nodule (Table 2).
Important information to be included in the referral form and the ultrasound report requested by the respondents.
Endocrinologists significantly use the ATA guideline for thyroid/neck US risk assessment and scoring system more than non-endocrinologists (35.5% versus 21.8%, p=0.008), whereas non-endocrinologists significantly follow the opinion of radiologists in evaluating thyroid nodules (2.6% versus 14.1%, p=0.001). More endocrinologists significantly repeat the FNA for high-risk nodules when they receive a patient from peripheral hospitals than non-endocrinologists (37.4% versus 26.9%, p=0.048). There were significantly larger proportion of endocrinologists who will perform FNA in the clinic with US guidance, and were more satisfied with a US-guided FNA carried out by fellow endocrinologist (p=0.021 and p=0.002). A significant proportion of endocrinologists will repeat the FNA for AUS/FLUS than non-endocrinologists (67.1% versus 27.6%, p<0.001), whereas non-endocrinologists will refer the patient most likely to a thyroidologist compared to endocrinologists (37.2% versus 7.1%, p<0.001). For thyroid nodules that are completely or mostly cystic with a benign FNA result, 79.2% of non-endocrinologists preferred to refer to surgery for management compared to only 51.5% of endocrinologists (p<0.001). A more detailed comparison regarding the clinical approach to the management of thyroid nodules is shown in Table 3.
Responses of endocrinologists and non-endocrinologists regarding clinical approach to the management of thyroid nodules.
If a solid thyroid nodule was benign and the patient complained of pressure symptoms, 94% of respondents would opt for surgery. If a cystic nodule was benign on FNA, 60.1% would opt for surgery, 17% would choose alcohol injection, and 10% would choose radio frequency ablation. If the nodule was benign without pressure symptoms, 53.1% would follow the patient up for 2 to 3 years. If the nodule turned out to be malignant or suspicious for malignancy, 58.2% would send the patient to an endocrine surgeon, 13.8% would send the patient to an ENT specialist or a head and neck surgeon, and 19% would send the patient to a surgeon with good experience regardless of his or her specialty (Figure 1).
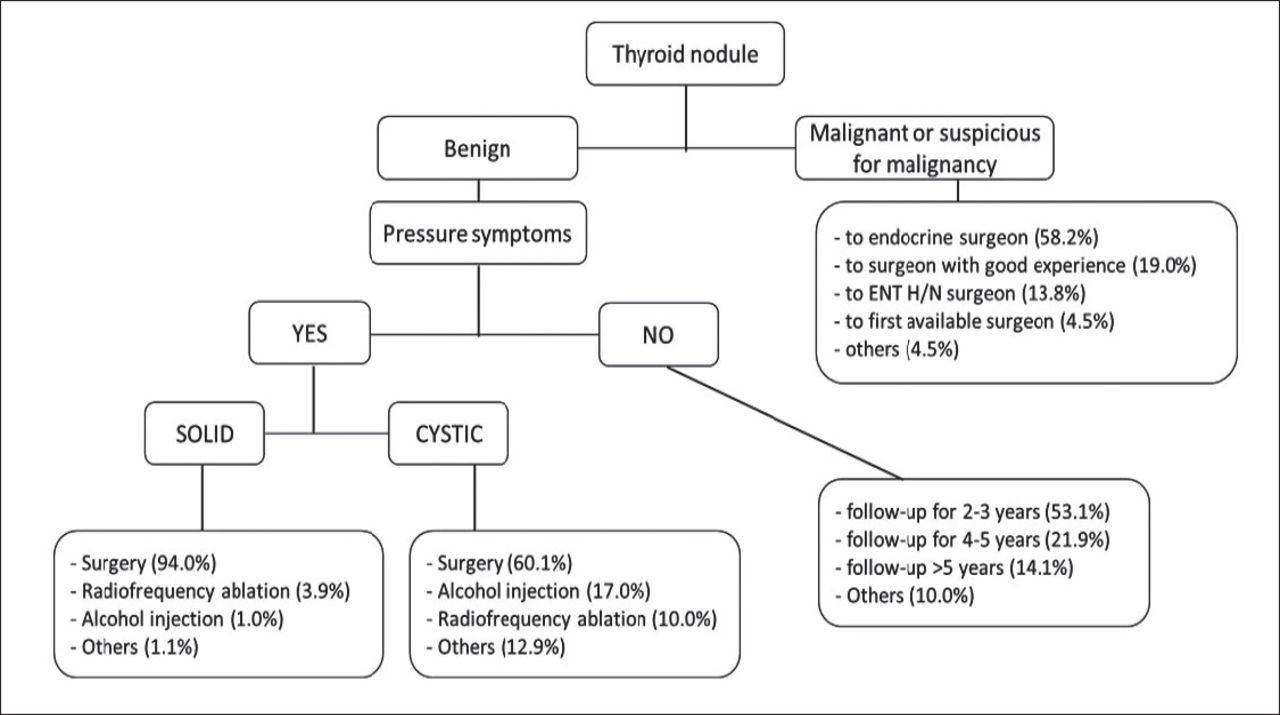
Respondent’s management based on fine needle aspiration (FNA) results for a benign nodule and a malignant or suspicious for malignancy nodule. ENT: ear, nose, and throat, H/N: head and neck
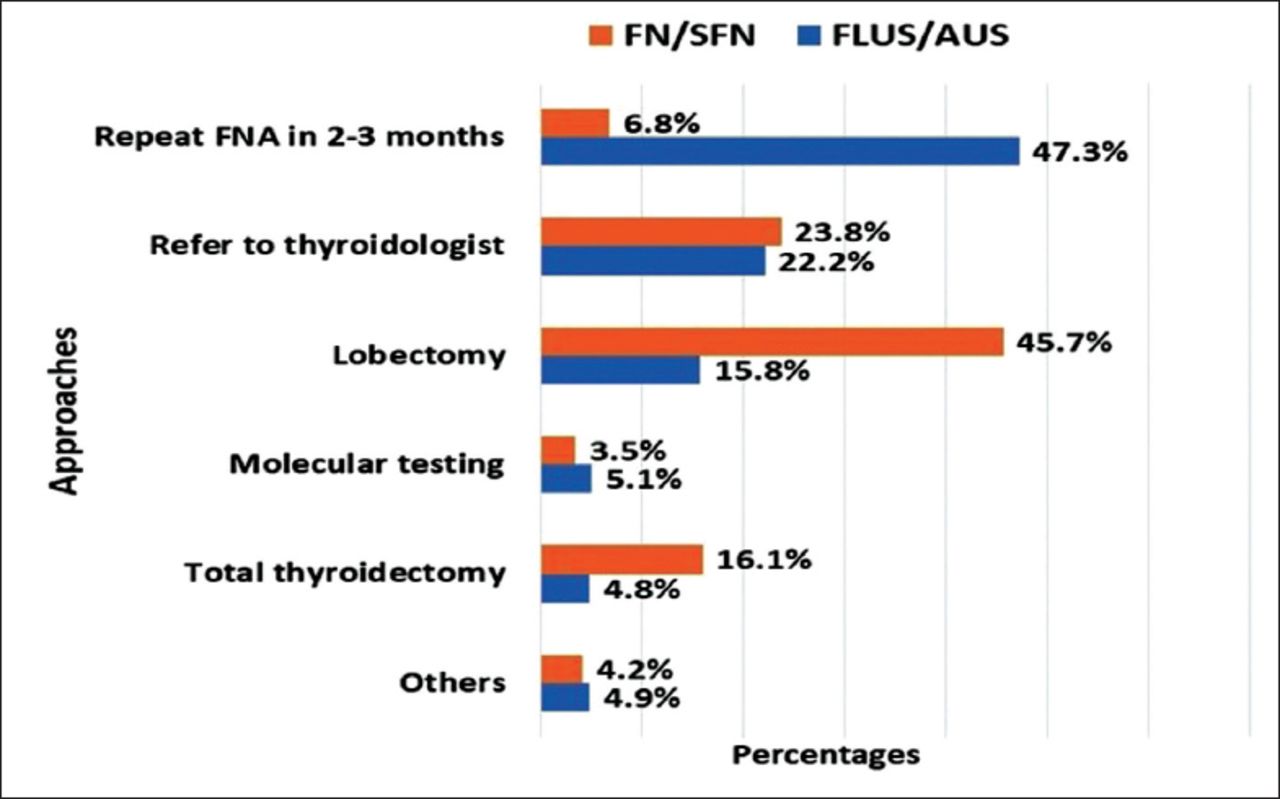
A larger percentage of respondents (n=137, 44.1%) believed that the percentage of indeterminate results in their hospital was higher than it should be (defined in the survey as >10% of all FNA cytology results). One hundred forty-seven respondents (47.3%) would repeat the FNA in 2 to 3 months if the FNA result was AUS/FLUS. If the FNA result was a follicular neoplasm or suspicious for follicular neoplasm (FN/SFN), 142 (45.7%) of respondents would opt for a lobectomy (Figure 2). Due to unavailability of the test in the region, only 27 (8.6%) would send for molecular testing. However, 174 (55.9%) would prefer to have molecular testing available for an indeterminate FNA result. Of those who preferred to use molecular testing for indeterminate AUS/FLUS or FN/SFN results, 11.3% preferred Afirma Xpression Atlas, 8% preferred ThyroSeq v3, 2.6% preferred ThyGeNEXT/ThyraMIR, 62% preferred to have them all available, and 14% would accept any one of these tests.

Respondent’s approach to fine needle aspiration (FNA) result of atypia of undetermined significance or follicular lesion of undetermined significance (AUs/FLUS) and follicular neoplasm or suspicious for follicular neoplasm (FN/SFN).
The responses to questions pertaining to their preferred US reporting. More than a quarter of respondents preferred the ATA Guideline Thyroid/Neck US Risk Assessment (n=89, 28.6%) or the American Thyroid Imaging Reporting and Data System (TIRADS) (n=83, 26.7%), 18 (5.8%) preferred the European TIRADS, and 73 (23.5%) expressed no preference for any of the US scoring systems. Twenty-four respondents (8%) would follow the radiologist’s opinion, and only 19 (6%) would check the US images by themselves. However, most of the respondents (n=263, 84.6%) preferred to have any one of the available US scoring systems or standard protocols to evaluate the risk of thyroid nodules.
Compared with respondents who had ≤10 years of experience, a significantly larger proportion of respondents who had >10 years of experience were concerned about a history of enlarged lymph nodes (p<0.001), pressure symptoms (p=0.002), and voice changes (p=0.047). A significantly larger proportion of female respondents than male respondents would repeat the FNA when they received an FNA report from another hospital, whereas male respondents would only review the slides with their pathologists (p=0.006).
There was high concordance of the participants’ responses with the 2015 ATA Guideline Thyroid/Neck US Risk Assessment, except for utilizing molecular testing for indeterminant FNA results (R13), which showed 5.1% concordance for AUS/FLUS and 3.5% concordance for FN/SFN.
Discussion
This study aimed to identify issues and problems encountered by physicians, particularly with regard to patient referral systems and management protocols that are aligned or not aligned with established guidelines or recommendations, and highlights the current practice of physicians managing cases of thyroid nodules in GCC countries. In the GCC countries, we did not find any published paper about the clinical practice of managing thyroid nodules. This web-designed survey highlighted the current practices of our respondents who are currently managing cases of thyroid nodules and gave us an idea on how all these practices were aligned with the established guidelines.
Thyroid nodules are very common, with high incidence and prevalence. Each patient goes through a series of referrals from a general practitioner to more subspecialized physicians, interventional radiologists, and/or surgeons. These referrals include history taking, examination findings, and workups including laboratory tests, radiology and imaging, and FNA. Problems in referrals that delay or hamper diagnosis and proper management of cases include insufficient information from the history and examination, incomplete laboratory and radiology tests, inappropriate FNAs, and even the experience of pathologists and cytologists in giving an accurate cytopathological diagnosis.8,14 This paves the way for surgical and non-surgical management of benign cases indeterminate malignancy, and unnecessary surgeries will expose patients to surgical risks and complications. Molecular testing has become the current standard of care in most developed countries and has a huge advantage in reducing unnecessary thyroid surgeries and avoiding surgical complications, particularly in cases with indeterminate cytology results.17-19
This study has clearly shown that there is a wide variation in many aspects of our studied variables. For instance, physicians have different perceptions of what referrals should contain based on their gender, age, specialty, and years of experience. A study by Jiang et al20 reported that great variations exist in thyroid nodule evaluations, which result from deviations from guidelines, particularly in stratification of nodules, obtaining TSH values, and obtaining US reports. The authors found that despite the availability of US reports, only 12.3% of reports contained information on nodule size in 3 dimensions, structure, echogenicity, and lymph nodes, which are considered components of a high-quality US. Our respondents’ statements around what a referral lacks and should contain may indicate the variation in protocols and guidelines used by the respondents. Most respondents preferred to have any one of the available US scoring systems of thyroid nodules to be incorporated in all of the reports of thyroid and neck US to facilitate the decision whether to perform FNA. Most respondents prefer the ATA Guideline Thyroid/Neck US Risk Assessment, 9 followed by the American TIRADS and then the European TIRADS.21,22 Some respondents preferred to follow the radiologist’s opinion, and few would check the US images by themselves.
Most of the respondents would reevaluate FNA reports received from other hospitals by either reviewing the slides or repeating the FNA in their hospital. Most respondents preferred to refer their patients who needed FNA to an interventional radiologist or to an endocrinologist who was performing US-guided FNA. However, there were few of these specialists in the peripheral hospital area, which may decrease the use of US guidance during the procedure and thus affect the accuracy and safety of the FNA.16 Furthermore, few endocrinologists in our area perform US-guided FNA in their offices due to the lack of training or the limited time available during their clinics.
Most patients, especially those who need surgery either because of non-benign FNA results or for pressure symptoms, are referred to endocrine surgeons, followed by ENT specialists or head and neck surgeons and surgeons with good experience. However, referrals depend on the availability of the surgical specialties and the protocols of their hospitals. Few respondents referred benign nodules for alcohol injection or radiofrequency ablation, although these are well-recognized and proven beneficial procedures. Possible reasons for this are the small numbers of physicians specializing in these procedures and of centers that offer them.
A considerable number of respondents believed that there was a large number of indeterminate FNA results, including AUS/FLUS and FN/SFN. This makes the next step of management more complicated and uncertain. This problem must be considered, and the quality of the FNA reporting must be assessed in each hospital and the results shared with the pathologists.23 An assessment of FNA technique, sampling quality, sufficiency, and cytologic diagnosis of thyroid FNA should be compared with the standards, which will definitely improve the delivery of service and patient satisfaction.
The 2015 ATA guidelines on the management of thyroid nodules, which include evaluations of TSH level, thyroid/neck US pattern, US-guided FNA, FNA cytology, and management, including the use of molecular marker tests, are one of the most acceptable guidelines among endocrinologists.7-10 They were the closest available guidelines to our respondents’ answers and choices. The concordance of our respondents with most of the ATA recommendations was between 60.1% and 98.4%, except for R13, which refers to the use of molecular testing for FNA results of AUS/FLUS, for which the concordance was only 5.1%. This low concordance was due to the unavailability of molecular testing in the region. There are very few hospital-based molecular pathology laboratories in the region.23 Most of the endocrinologists preferred to have the molecular test available, and they believed that it was going to change the practice of management of thyroid nodules in the area. A large number of respondents recommended surgery for indeterminant FNA results, which would result in more unnecessary surgeries and preventable complications. The survey clearly indicates the importance of making molecular testing available to physicians and surgeons treating patients with thyroid nodules, regardless of the type of test. The other incompatibility we found was that few respondents referred benign cystic nodules for alcohol injection (R28), which may be explained by the shortage of physicians and interventional radiologists performing this procedure.
Some published regional guidelines have variations from the ATA guidelines or other universally published guidelines, which may be explained by differences in population characteristics, referral systems, and the availability of certain subspecialties, facilities, and investigational methodologies.25, 0 This also may explain the differences between our respondents in the management of thyroid nodules.
Our study implies that the current system of referrals of thyroid nodules in the GCC countries is not optimal and may lack some crucial information from the patients’ history and physical examination. The initial investigations of patients with thyroid nodules before referral needs to be improved. Additionally, ultrasound reports by radiologists needs to follow standards including measurement, recording the high-risk features of the nodules and lymph nodes, following up changes in nodule features and size, and following one of the protocols or scoring systems used to assess nodule risk. This will benefit our patients with thyroid nodules and save significant time, money, and effort. Moreover, performance of FNA varies from one institution to the other, and in some places, it is not performed according to standards. There is a need for future studies to investigate what are the probable reasons for the non-optimal referral system apart from its alignment to established management guidelines for thyroid nodule management and assess the practice of thyroid cancer management to come up with a comprehensive regional guideline for thyroid nodule and thyroid cancer management.
Study limitation
This study was conducted through a web-based survey. Inasmuch as we wanted to conduct a face-to-face interview, the wide distance of targeted respondents limited us to do so. Furthermore, an online interview through web applications would have been ideal, but there were problems encountered with setting up the meeting because of differing work schedules. We also did not ask about some details in thyroid nodule management and we limited our questions in the survey to important practical problems that faced commonly on daily basis.
In conclusion, despite the survey nature of this study, which acted as a limitation, this study was able to highlight for the first time the variation in practices with regard to the management of thyroid nodules in the GCC countries. Our results suggest a demand for a consensus based on common grounds of good clinical practice that should be established based on available local data and accessibility of certain facilities, to smooth its implementation. A regional guideline, which we believe our study will aid, to be built on agreed-on recommendations by most of the involved caregivers, is needed to improve initial assessment and referrals, initial workup, radiology and cytology reports, and clinical and surgical management. The results of this survey also support the need for molecular testing and recommend its implementation in our regional health system.
Acknowledgment
We would like to thank the Researchers Support and Services Unit, Deanship of Scientific Research of King Saud University, Riyadh, Saudi Arabia and Enago Crimson Interactive Inc. of Kent, Delaware, USA for English language editing services.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 8, 2020.
- Accepted November 25, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.