


Abstract
Objectives: To compare the efficacy of interspace between the popliteal artery and the capsule of the posterior knee (iPACK) block with periarticular local infiltration analgesia (LIA) to assess postoperative pain control and enhanced recovery after total knee arthroplasty (TKA).
Methods: This research was carried out at King Saud University Medical City, Riyadh, Saudi Arabia, from September 2020 to March 2021. Eighty Patients scheduled for elective unilateral TKA were randomized to receive either iPACK or periarticular LIA along with adductor canal block under spinal anesthesia. The primary outcome was postoperative pain score, and secondary outcomes included physical rehabilitation, duration of surgery, length of post-anesthesia care unit stay, hemodynamics, and length of hospital stay.
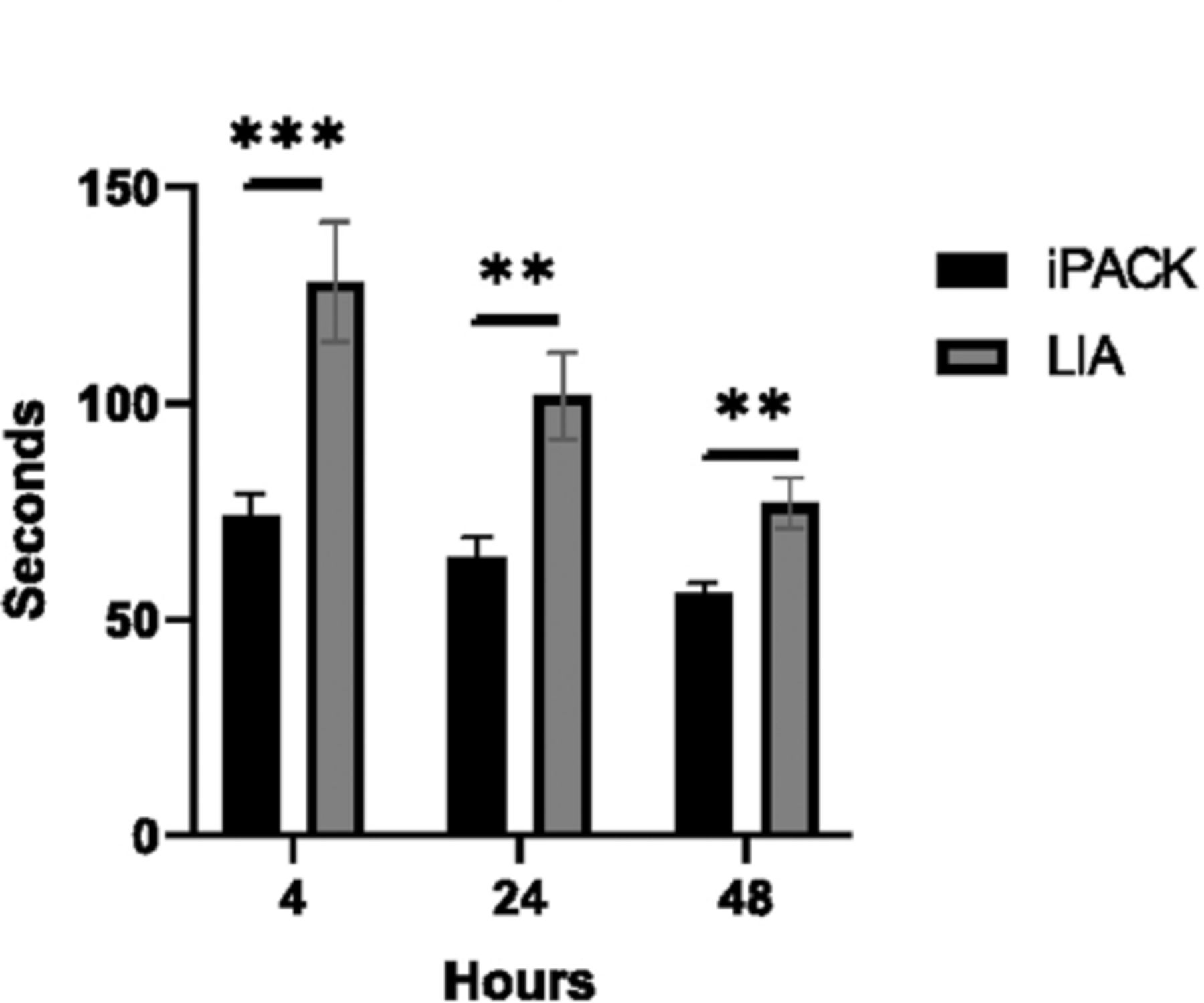
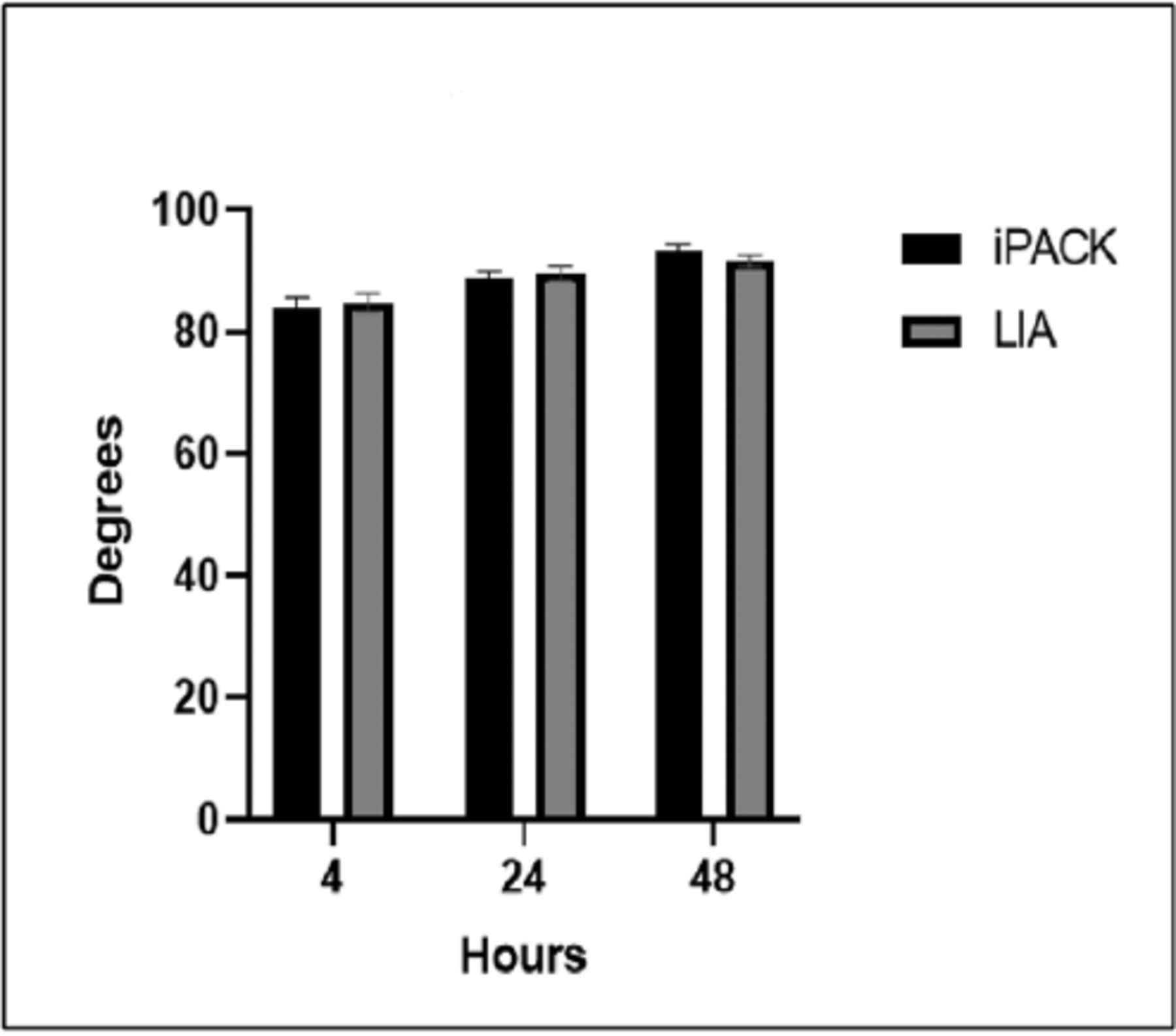
Results: The pain score during activity in iPACK group was significantly lower compared to LIA group at 4 hours postoperatively, but no significant difference was observed at 24 or 48 hours. The timed up and go test took significantly longer for patients in LIA group at 4, 24, and 48 hours compared to those in iPACK group. No significant differences in knee range of motion were observed between the 2 groups at any point.
Conclusion: Based on our findings, iPACK block is an effective technique in reducing pain in the immediate postoperative period without affecting motor function, resulting in enhanced recovery following primary TKA.
Optimal pain control and safe postoperative early mobilization are the main objectives of enhanced recovery after total knee arthroplasty (TKA).1,2 The trend of postoperative analgesia after TKA has been shifted from epidural and femoral nerve blocks (FNB) to motor-sparing sensory nerve blocks. Femoral nerve block is an effective technique to control anteromedial pain and reduce postoperative opioid consumption post TKA but results in quadriceps muscle weakness, making physical rehabilitation unsatisfactory.3-5 Alternatively, blocking the saphenous nerve in the adductor canal provides comparable anteromedial pain relief and preserves quadriceps strength comparing to FNB after TKA.6-8
Human knee innervation is complex.9 The posterior knee joint is innervated by popliteal plexus, formed by the tibial and posterior branches of the obturator nerves.10 The efficacy of blocking these terminal sensory branches at the posterior knee capsule is under investigation. Pain that arises from the posterior knee after TKA may be ameliorated by ultrasound-guided local anesthetic infiltration of the interspace between the popliteal artery and the capsule of the posterior knee (iPACK).11,12 Since the first description of iPACK block by Sinha (unpublished observation)extensive research has been carried out to assess its efficacy. 13,14 The advantages of iPACK compare to other modalities for posterior knee pain control are its motor-sparing analgesic effectiveness, reduced postoperative opioid consumption, and improved functional measures.15 Unwanted complications during iPACK block include the risk of common peroneal nerve block, intravascular injection, or vascular injury to the nearby popliteal vessels.
In contrast to the local anesthetic infiltration of iPACK, intraoperative periarticular local infiltration analgesia (LIA) is a standard analgesic option for acute pain management after TKA. However, LIA block is performed by orthopedic surgeons on landmark technique. Its efficacy depends on the technique and the analgesic drugs regime used, but there is no consensus.16 Therefore, provided the potential advantage of motor-sparing and may be comparable analgesia of iPACK, this study aimed to compare iPACK block with routine periarticular LIA block when combined with adductor canal block (ACB) under spinal anesthesia. We hypothesize that iPACK is an effective technique to provide adequate analgesia after TKA.
Methods
We performed a prospective randomized controlled trial among patients who underwent elective, primary unilateral TKA under spinal anesthesia. The trial was registered at clinicaltrials.gov #NCT04565093. After obtaining Institutional Review Board approval (No. E-20-4819, from King Khalid University Hospital, Riyadh, Saudi Arabia), this study was carried out from September 2020 to March 2021. The inclusion criteria were having an American Society of Anesthesiologists (ASA) classification of I–III, being ≥18 years old, and having a body mass index (BMI) of ≤50 kg/m2. Patients were excluded if they had a history of rheumatoid arthritis, renal impairment, liver disease, had undergone prior back surgery, were on any anticoagulant, or had any other contraindication for spinal anesthesia.
All patients were informed and consented to receive either iPACK block + ACB (iPACK group; n=40) or periarticular LIA block + ACB (LIA group; n=40) after spinal anesthesia. On arrival to the operation room, all eligible participants had an intravenous cannula in situ and monitors according to ASA guidelines. Under complete aseptic technique, spinal anesthesia was performed with a pencil-point 27-gauge (Whitacre) needle at lumbar space L3-L4 or L4-L5, with bupivacaine heavy (0.5%) and fentanyl (15 μg), for a total volume of 3 mL.
The randomization scheme was generated using an online software (www.randomizer.org). Random allocation to either the iPACK or LIA group was indicated in a sealed, opaque envelope organized and opened in the block area by the anesthesia nurse. All participants and postoperative outcome assessors (physiotherapists) were blinded to the group allocation. The anesthesiologist responsible for intraoperative care and the operating surgeon were aware of the randomization.
Description of peripheral nerve block techniques
Infiltration of the interspace between the popliteal artery and the capsule of the posterior knee and ACB were performed using a complete aseptic technique and under ultrasound guidance by consultants anesthesiologists or regional anesthesia fellows approximately within 10-15 minutes. Four senior orthopedic consultants performed the periarticular LIA block under complete aseptic measures using a technique based on landmarks approximately within 5-10 minutes.
Adductor canal block
A linear transducer (SonoSite 15-6 MHz) was placed anteriorly distal to mid-thigh then slide medially to locate the femoral artery under the sartorius muscle. The needle (Pajunk, Germany, 80-100 mm) was inserted in-plane in a lateral-to-medial orientation and advanced further to penetrate the vasto-adductor membrane into the adductor canal toward the saphenous nerve if visible. After careful aspiration, 1-2 mL of normal saline was injected anterior and lateral to the femoral artery to confirm the proper injection site. The needle was redirected if the spread of normal saline was not evident. A total of 20 mL of bupivacaine (0.25%) was injected into the adductor canal around the femoral artery.17
Interspace between the popliteal artery and the capsule of the posterior knee block
A curvilinear transducer (SonoSite 5-2 MHz) was placed on the popliteal crease to visualize the space between the popliteal artery and femoral condyles. The needle (Pajunk, Germany, 80-100 mm) was inserted in-plane from the transducer’s anterior end in a medial-to-lateral trajectory. With the needle tip resting 2 cm beyond the lateral border of the artery, 20 mL of bupivacaine (0.25%) was injected after a negative blood aspiration to infiltrate the tissue space in divided doses as the needle was withdrawn.11
Periarticular LIA block
A mixture of 20 ml of bupivacaine (0.5%), 100 μg epinephrine, ± 10 mg of Morphine, ± 8 mg of lornoxicam, was diluted in 40 mL of normal saline. The posterior capsule was infiltrated with the mixture solution prior to implantation. After implantation, the rest of the solution was injected into the retinacular flaps, surrounding muscles, and subcutaneous tissues.18
Postoperative pain control
All participants were prescribed intravenous morphine 2 mg bolus, up to a maximum of 10 mg, if indicated in the Post-Anesthesia Care Unit (PACU). The multimodal analgesic regimen for the ward included 8 mg of intravenous lornoxicam every 12 hours and 1 gm of paracetamol every 8 hours if indicated for postoperative days 0-1. After 24 hours, 200 mg of celecoxib was given orally every 12 hours, as well as 20 mg of oxycodone orally every 12 hours and 75 mg of pregabalin orally every 12 hours; in addition, 1 gm of paracetamol, taken orally every 6 hours, was prescribed for breakthrough pain.
The primary outcome was the severity of pain assessed postoperatively at 4, 24, and 48 hours by 3 physiotherapists blinded to group allocation. Physical rehabilitation was evaluated by measuring the active-assisted knee range of motion (ROM)19 using a goniometer (Sammons Preston-Rolyan #7514, Bolingbrook, IL, USA), and a timed up and go (TUG) test used to assess postoperative ambulation. Timed up and go test uses the time a person takes to rise from an armchair, walk 3 meters, turn around, walk back to the chair, and sit down.20 All patients were instructed preoperatively on how to report postoperative pain on a 10-point numerical rating scale (NRS), where 0 is no pain and 10 is the worst pain imaginable. The secondary outcomes were physical rehabilitation progress, duration of surgery, length of PACU stay, postoperative hemodynamics, length of hospital stay (LOS), and any adverse effects like vascular injury, common peroneal nerve block, intravascular injection/local anesthetic systemic toxicity or any other iPACK- or ACB-related complications.
Statistical analysis
A previous trial found that the mean ± standard deviation of pain score at 24 hours post TKA to be 4.9 ± 2.7 points, and post iPACK to be 2.5 points. Assuming 80% power at a 2-sided number of 0.05, we determined that a sample size of 40 patients per group total of 80 would be essential.12,14 Statistical analysis was performed using GraphPad Prism version 8.4.3 for Windows (GraphPad Software, La Jolla, CA, USA). Where appropriate, group means with a standard error of the mean (SEM) and sample size were reported. For all tests, differences between the groups were reported as exact p-values. Differences were considered statistically significant at an alpha level of <0.05. An unpaired student’s t-test was used to calculate group differences between parametric data. Chi-square test was used to calculate group differences between non-parametric and categorical data.
Results
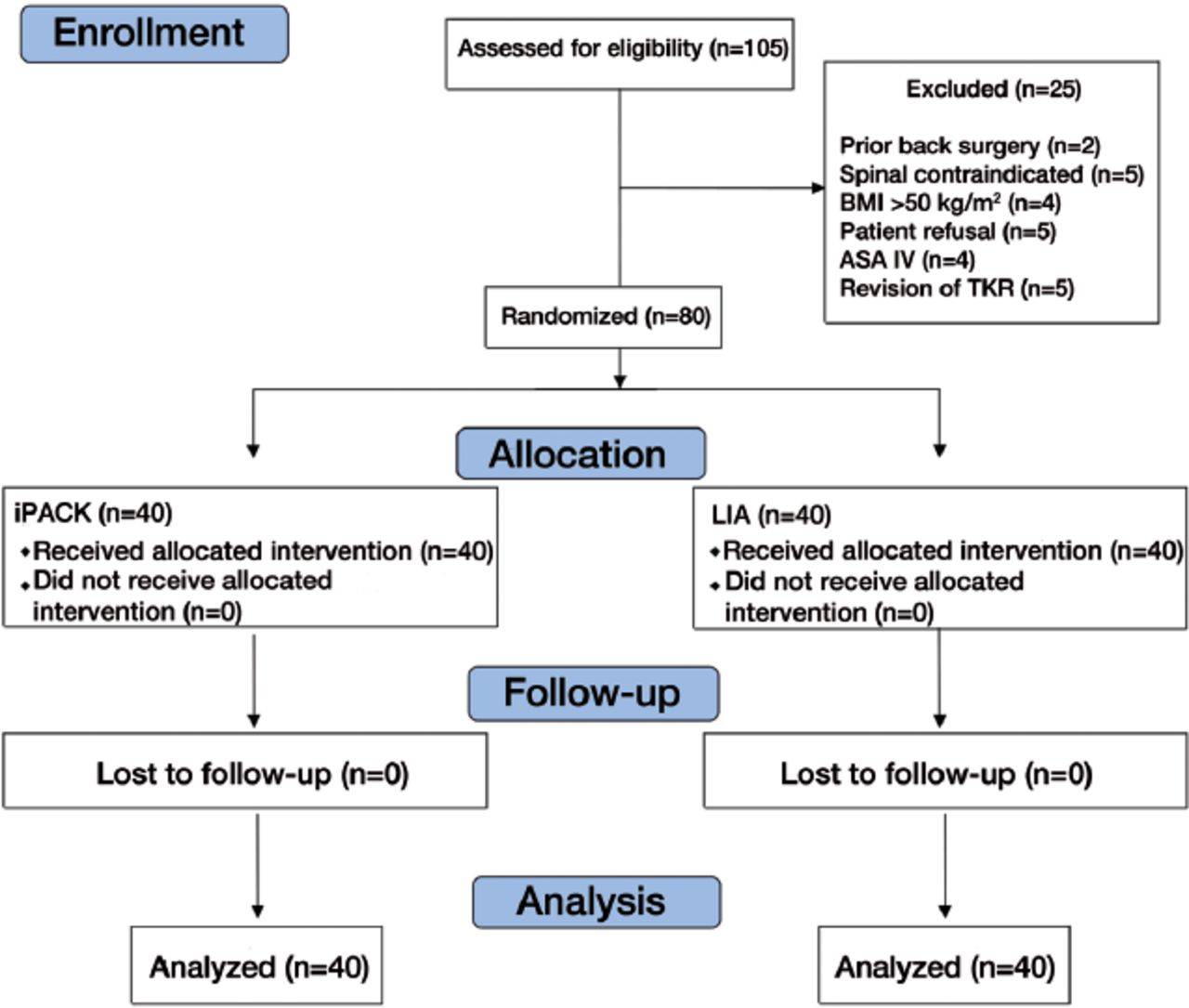
During recruitment, 105 patients were assessed for eligibility. Twenty-five patients were excluded from the study who met the exclusion criteria. We randomly allocated 80 patients to either the iPACK or LIA group to assess postoperative pain after TKA (Figure 1). The demographic data was comparable between the 2 groups (Table 1). There were no statistically significant differences between the 2 groups in relation to the duration of surgery, length of PACU stay, mean arterial pressure, heart rate, or LOS in days (Table 2).
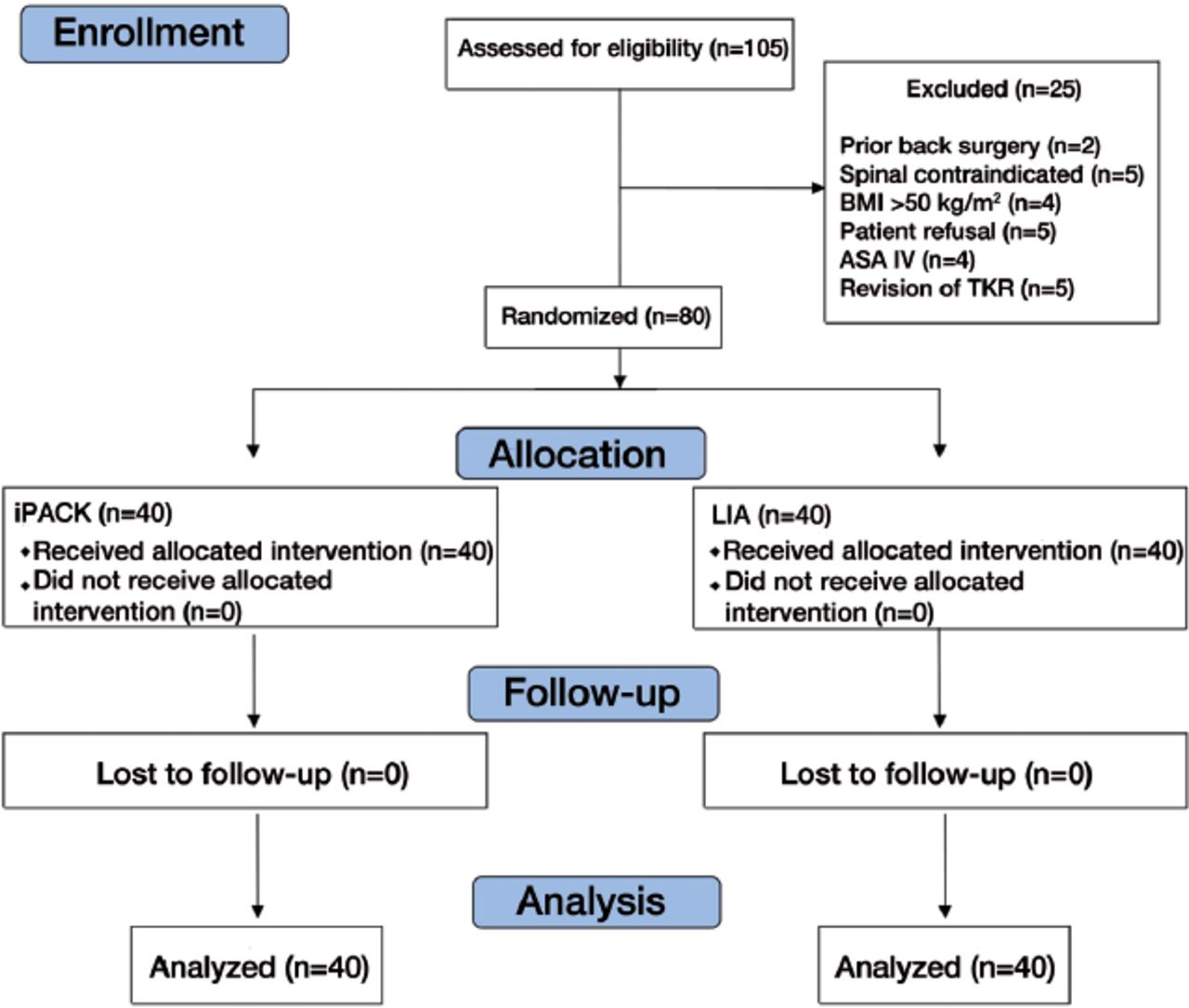
- Consolidated standards of reporting trial flow diagram. iPACK: interspace between the popliteal artery and the capsule of the posterior knee, LIA: local infiltration analgesia, GA: general anesthesia
- Demographic data comparing iPACK and LIA groups.
- Intraoperative and postoperative patients characteristics comparing iPACK and LIA groups
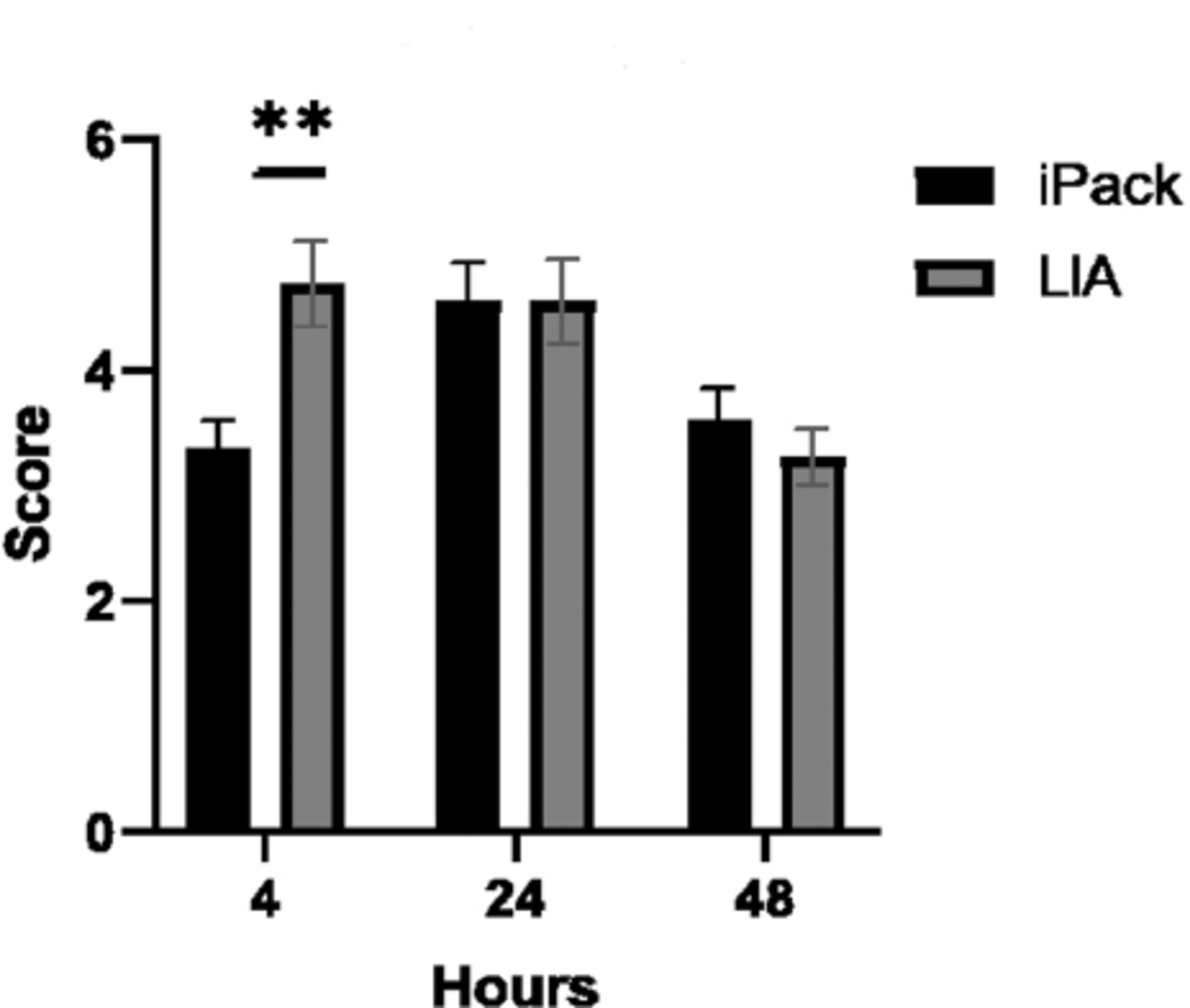
As shown in Figure 2, the pain score was significantly lower in the iPACK group compared to the LIA group at 4 hours postoperatively (3.32 versus 4.75) (p=0.0046). No significant difference was observed after that at 24 hours (p=0.8253) or 48 hours (p=0.4098) when comparing the 2 groups. The TUG test, in seconds, was significantly longer in the LIA group at 4, 24, and 48 hours compared to the iPACK group (p=0.0004, p=0.0013, and p=0.0017), respectively; (Figure 3). No significant differences were observed between the 2 groups when comparing knee ROM at 4 hours (p=0.7935), 24 hours (p=0.6979), or 48 hours (p=0.3069)(Figure 4).
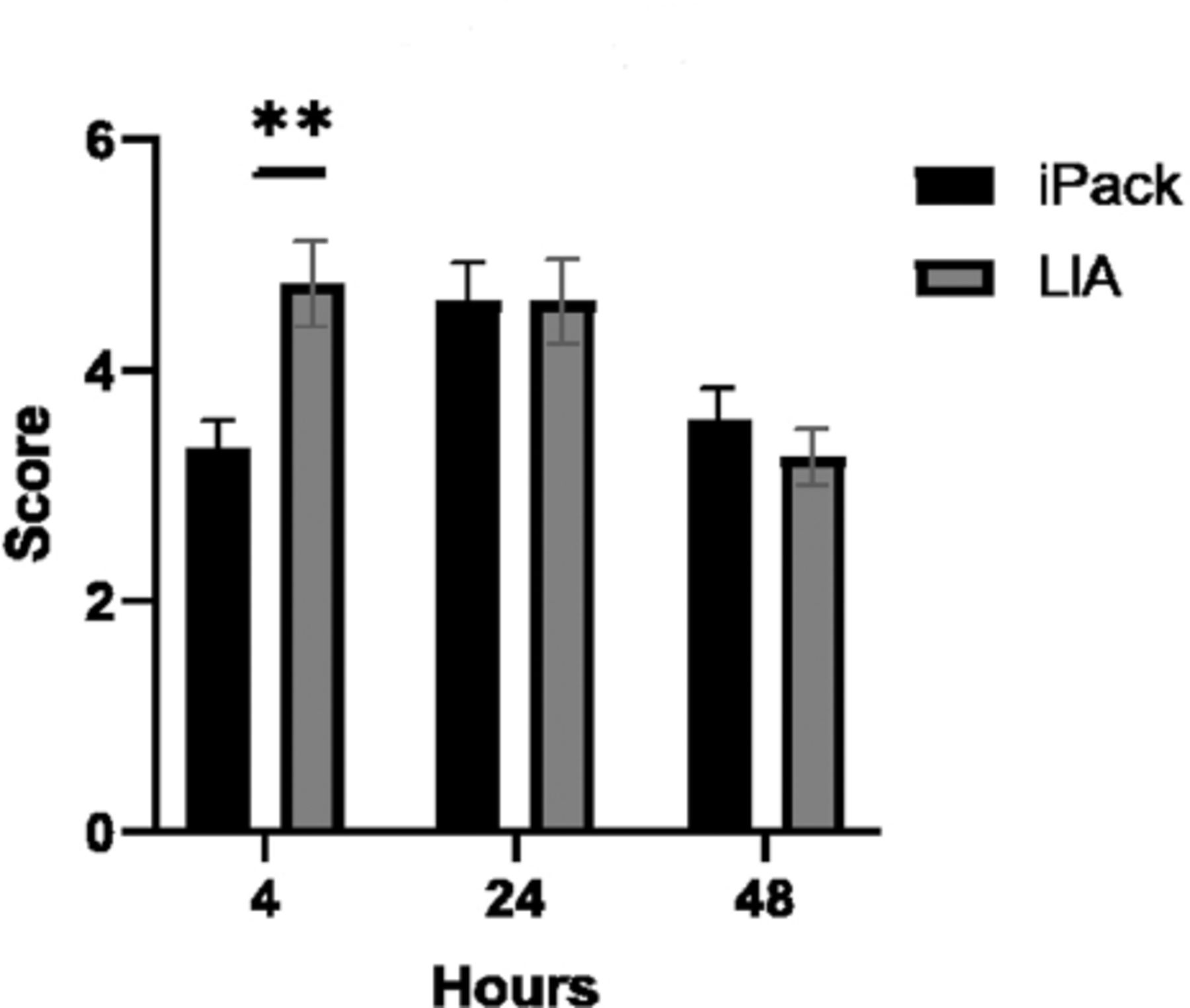
- Pain score during mobilization using Numerical Rating Scale (NRS 0-10) where 0 is no pain and 10 is the worst pain imaginable at 4, 24, and 48 hours postoperatively comparing iPACK and LIA groups. *p<0.05, **p<0.01, ***p<0.001, iPACK: interspace between the popliteal artery and the capsule of the posterior knee, LIA: local infiltration analgesia

- Timed-Up-and-Go test in seconds at 4, 24, and 48 hours postoperatively comparing iPACK and LIA groups. *p<0.05, **p<0.01, ***p<0.001, iPACK: interspace between the popliteal artery and the capsule of the posterior knee, LIA: local infiltration analgesia

- Assisted-active knee range of motion (ROM) 0=full extension 135=maximum flexion in degrees at 4, 24, and 48 hours postoperatively comparing iPACK and LIA groups. iPACK: interspace between the popliteal artery and the capsule of the posterior knee, LIA: local infiltration analgesia
Discussion
This study was carried out to assess the efficacy of iPACK block compared with LIA block under spinal anesthesia and ACB in relation to postoperative pain control and early mobilization. We found that patients who received iPACK block reported mild pain in the early postoperative period only, while those in the LIA group reported moderate pain. This assessment was conducted immediately after the spinal anesthesia effect had worn off 4 hours after surgery. After that, the pain score was moderate in both groups on days one and 2. Similarly, there was no significant difference in analgesic consumption between the 2 groups. As the patients in the iPACK group had less pain, they had better mobility compared to those in the LIA group as early as 4 hours on the ward. The active-assisted knee ROM measurements, taken while the patients were still on the ward, were comparable between the 2 groups. Therefore, postoperative early rehabilitation was possible in the iPACK group due to better pain control and the motor-sparing effect of the combination of iPACK block and ACB. These findings support those reported in a retrospective study conducted by Jung.21
Periarticular LIA block, first described by Kerr and Kohan.22 Although it is a blind landmark technique and there is no consensus on the optimal dose or medication regime for postoperative pain control, its analgesic effect is undoubted. A recent meta-analysis showed that local anesthetic infiltration is superior to epidural analgesia for postoperative pain control after TKA.23 Perhaps the doses and techniques used for periarticular LIA were likely inconsistent between the different operating surgeons in our study. Another systemic review and meta-analysis investigated and did not support adding iPACK block to ACB in the presence of periarticular LIA due to lack of any additional benefit.24
The intra-articular excision of the knee evokes pain from structures being innervated by the popliteal plexus. Ultrasound-guided iPACK block mainly targets the terminal branches of the popliteal nerve plexus, which directly supply the posterior capsule of the knee.25 In 2 different studies, Kampitak et al2,25 discussed the optimal location of the motor-sparing effect of iPACK block and its related complications. In this study, we performed the iPACK block between the popliteal artery and the femoral condyles, just above the popliteal crease. None of our patients had vascular injury, common peroneal nerve block, intravascular injection/local anesthetic systemic toxicity, or other iPACK- or ACB-related complications.
Study limitations
First, the medication regimen (including dosages) and knee infiltration analgesia techniques used by different surgeons at our institute were not standardized. Second, patients’ preoperative knee pain and medications were not recorded in this study. As such, further studies on a large number of patients are required to eliminate these limitations.
In conclusion, iPACK block is an effective technique in reducing pain in the immediate postoperative period without affecting motor function, resulting in enhanced recovery following primary TKA.
Acknowledgment
This work was supported by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia. The authors would like to thank Shatha Alsousy, Jameela Alshahrani, and Alhudrin Sahiol from the Department of Physiotherapy, King Saud University Medical City, Riyadh, Kingdom of Saudi Arabia for postoperative data collection. Moreover, we would like to thank Dr. Saara Mansoor, PhD. student, Dalhousie University, Halifax, Canada, for the statistical analysis of the data obtained. We would like to thank SCRIBENDI (https://www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 23, 2021.
- Accepted August 25, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.