


Abstract
Objectives: To investigate the clinical profiles and outcomes of young adults presenting with ST-segment elevation myocardial infarction (STEMI).
Methods: We retrospectively reviewed King Saud Medical City, Riyadh, Saudi Arabia, registry between January 2016 and November 2017 for all patients younger than 45 years old who were admitted with STEMI. We compared this study population to a control group of patients aged 45 years and older who were enrolled in the same period.
Results: In total, 402 patients were enrolled; 197 were younger than 45 years. The incidence of newly diagnosed dyslipidemia was higher in younger patients (44% vs. 32%, p=0.01). Smoking was significantly more prevalent in the younger group (52% vs. 35%, p=0.001). The prevalence of pulmonary edema and cardiogenic shock on presentation was significantly higher in the older group (3% vs. 10; odds ratio, 4.43; 95% confidence interval, 1.750-10.94; p=0.002). Hospital stay was also longer in the older group (4±2 vs. 5±2 days, p=0.03).
Conclusion: ST-segment elevation myocardial infarction in young patients has a favorable outcome. Smoking and dyslipidemia are the main risk factors for STEMI in young individuals. The majority of young patients with dyslipidemia were not aware of their pre-existing condition. Our findings recommend local adaptation and implementation of screening programs for dyslipidemia in the young and the reinforcement of smoking prevention programs.
ST-segment myocardial infarction (STEMI), a serious consequence of coronary artery disease (CAD), tends to affect people between the sixth and seventh decade of life.1 Patients younger than 45 years of age represent approximately 5-10% of all acute myocardial infarction (AMI) cases.2,3 In developing countries, however, AMI frequently occurs at a younger age, approximately one decade earlier than that reported in developed countries.4 The Middle East has one of the highest percentages (11%) of adults who develop STEMI for the first time before the age of 40 years.5 In comparison, the rate in North America is 4%, Western Europe is 2.7%, and Africa is 9.7%.6
In young patients, STEMI has lower mortality rates and a lower incidence of related major adverse cardiovascular events (MACE), such as cardiogenic shock or stroke. Moreover, a higher rate of successful primary percutaneous coronary intervention accompanied by higher thrombolysis in myocardial infarction grade flow and fewer bleeding complications have been reported in young patients.7
The mechanisms and disease courses of STEMI in young individuals may differ from those in the elderly. Cigarette smoking with or without cocaine abuse is considered one of the strongest risk factors associated with CAD in young adult.2,3 Moreover, a family history of premature coronary artery disease is frequently encountered as an important risk factor in youth.8 This could be attributed to genetic disorders related to lipid metabolism.9 Most previous reports have shown favorable outcomes in young adults with AMI.10 However, identifying the variations of such risk factors for STEMI in the younger age group might have an important value for preventive measures and treatment plans.
In Riyadh, Saudi Arabia, there are 8 million residents, of which 6.5 million are younger than 45 years.11 This is partly due to the presence of predominantly male young migrant workers, representing more than 3 million residents.12 To date, several studies have investigated AMI in patients younger than 45 years.1,2,13 However, only few have focused on STEMI.7 Locally, approximately 25% of patients presenting with STEMI are younger than 45 years.14 However, local studies investigating such cases are extremely scarce.5,15 On the same note, specific modifiable risk factors such as smoking (21%), obesity (37%), and diabetes (23%) are more prevalent regionally than globally.16-18 Therefore, the circumstances were ideal for investigating the clinical profile and outcome of acute STEMI in adults younger than 45 years in comparison to those of older patients.
Methods
We retrospectively reviewed our electronic database, Medysis® (Riyadh, Saudi Arabia), of all patients younger than 45 years of age who were admitted with a confirmed diagnosis of STEMI between January 2016 and November 2017 at a tertiary care hospital, King Saud Medical City (KSMC), Riyadh, Saudi Arabia. We compared the study population to a control group of older patients consecutively enrolled in a contemporary period. In each subject, we reported the presence of traditional cardiovascular risk factors, including current smoking habits and a family history of CAD, dyslipidemia, arterial hypertension, and diabetes mellitus. In addition, clinical and laboratory data including blood pressure, laboratory tests, electrocardiography (ECG), weight, height, body mass index, echocardiography, in-hospital outcomes (recurrent chest pain, heart failure, stroke, bleeding, cardiogenic shock, and death), length of hospital stay, and circadian dependence of symptom onset were recorded. This study was approved by the Institutional Review Boards of KSMC, which waived the requirement for patient consent.
Inclusion criteria were all patients aged <45 years, diagnosed with STEMI based on clinical presentation, with available ECG and blood tests (creatine kinase and troponin levels were included). The ECG criteria used to diagnose STEMI were any new ST-segment elevation measuring >0.2 mV in ≥2 contiguous leads (V1-V3) or >0.1 mV in all other leads, or the presence of a new left bundle branch block accompanied by an increase in troponin-I or T. We excluded all patients with incomplete data, those with a non-confirmed diagnosis of STEMI.
Data was retrospectively collected from clinical records and electronic charts, web-based clinical databases, and clinical imaging storage systems. The web-based clinical databases contain the following information: demographic data, cardiovascular risk factors, and clinical and laboratory data, as well as the time of symptom onset subdivided into 4 categories (midnight-06:00, 06:00-12:00, 12:00-18:00, and 18:00-24:00). Echocardiographic variables, including left ventricular (LV) ejection fraction, LV dimensions, and diastolic function, were recorded.
We looked at treatment strategy, thrombolytic therapy (alteplase) vs. invasive treatment. Major adverse cardiovascular events were defined as a composite of cardiac death, stroke, and acute kidney injury. Cardiac death was defined as death due to pump failure, cardiogenic shock, arrhythmia, or severe pulmonary edema.
Statistical analysis
The collected quantitative data was described in terms of mean ± standard deviation and range, and the qualitative data was described in terms of frequency and percentage. Comparisons between young and old patients were carried out using the Mann-Whitney test, the test of proportion (Z), the Chi-square test (x2), or the Fisher exact test as appropriate. Statistical significance was set at p<0.05. Statistical analyses and data plotting were performed using GraphPad Prism 8.
Results
We included 402 patients, of whom 197 (49%) were younger than 45 years. The baseline characteristics are shown in (Table 1). The mean age was 40±4 years among patients younger than 45 years and 55±7 years among those older than 45. Women represented 2.5% of the young group and 3% of the elderly group. Patients with a history of hypertension (25% vs. 36%), diabetes (40% vs. 52%), dyslipidemia (16% vs. 24%), and obesity (7% vs. 19%) were significantly less common among the younger group than among the older group. However, upon further workup, the incidence of newly diagnosed dyslipidemia was found to be more common in the younger age group (44% vs. 32%). There was no significant difference in the overall prevalence of dyslipidemia between the younger and older groups (60% vs. 56%). Furthermore, smoking history was significantly more prevalent in the younger group (52% vs. 35%), as was the case with substance abuse (3% vs. 0.5%). Importantly, a history of prior myocardial infarction was significantly more frequent in elderly patients than in younger patients (12% vs. 6%).
- Baseline demographic and clinical characteristics of patients younger and older than 45 years.
The atypical symptomatic presentation and diurnal variation did not show any significant difference between the groups, and oxygen saturation was higher in the younger group (97% vs. 96%; Table 2). Symptom to door time of <12 hours was more common in younger patients (81%) than in elderly patients (77%). The mean symptom to door time was 9±19 hours in young patients and 12±28 hours in old patients (p=0.22). The maximum time from symptoms onset to presentation was 3 days in young patients compared to 7 days in the old patients.
- Clinical presentation and outcomes of patients younger and older than 45 years.
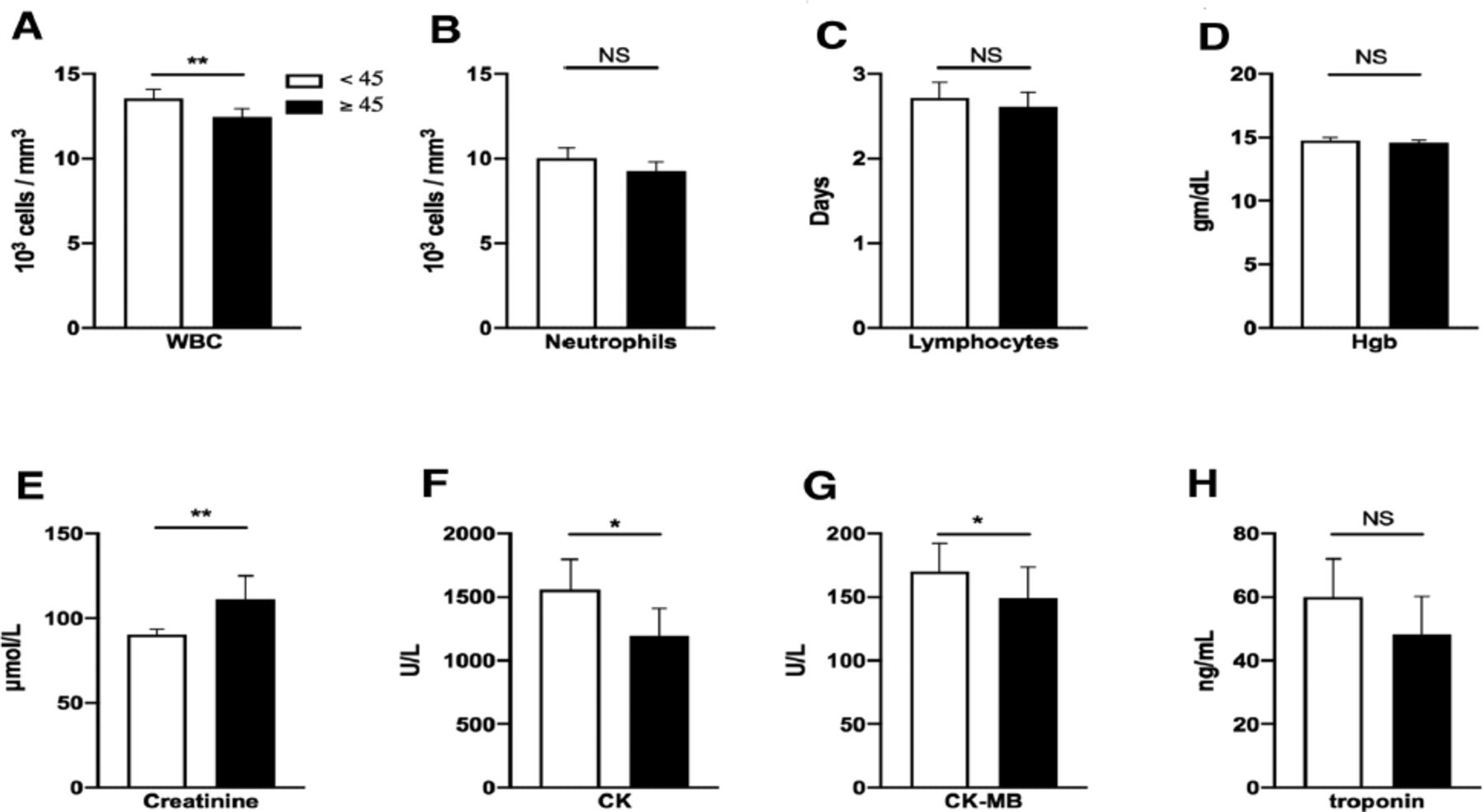
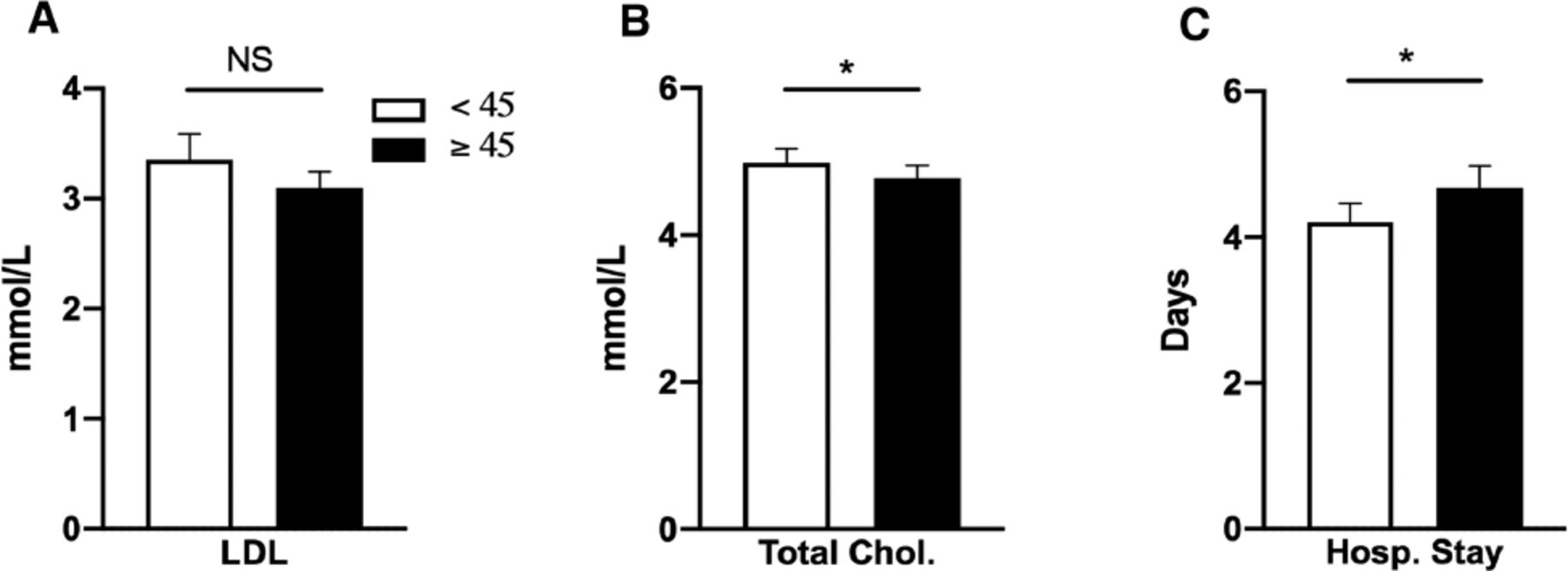
The mean initial and peak white blood counts values were higher in the younger than in the older patients (13.5x103 cells/mm3 vs. 12.4x103 cells/mm3, p=0.005; and 14.2x103 cells/mm3 vs. 13.1x103 cells/mm3, p=0.006) (Figure 1A). There was no significant difference between the mean neutrophil and lymphocytic counts when compared between the 2 age groups (10.02x103 cells/mm3 vs. 9.28x103 cells/mm3, p=0.06; and 2.71x103 cells/mm3 vs. 2.61x103 cells/mm3, p=0.4) (Figure 1 B&C). Hemoglobin levels were comparable between the 2 groups with no significant difference (14.75 g/dL vs. 14.57 g/dL, p=0.1) (Figure 1D). In contrast, the mean creatinine level at presentation was significantly higher among the older patients (90.3 μmol/L vs. 111.2 μmol/L, p=0.004) (Figure 1E). The peak creatine kinase (CK) (1557.2 U/L vs. 1194.4 U/L, p=0.02), CK-MB (169 U/L vs. 149 U/L, p=0.01), and troponin levels 60 ng/mL vs. 48 ng/mL, p=0.1) were higher in younger patients than in older patients (Figure 1F-H). Similarly, the mean low-density lipoprotein (3.35 mmol/L vs. 3.09 mmol/L, p=0.1) and total cholesterol levels (4.9 mmol/L vs. 4.7 mmol/L, p=0.04) were higher in the younger age group (Figure 2 A&B). Other laboratory findings and the left ventricle ejection fraction did not show any significant differences between the 2 groups (Table 2).

- Laboratory results for patients younger and older than 45 years. A) Mean white blood cell count (WBC) among patients younger than 45 years of age in comparison to that among patients aged 45 years or older at presentation. B-C) Mean neutrophil and lymphocytic count in patients younger and older than 45 years at presentation B) Mean hemoglobin (Hgb) level among patients younger than 45 years in comparison to that among patients aged 45 years or older. E) Mean creatinine level in patients younger than 45 years in comparison to that among patients aged 45 years or older. F-H) The cardiac markers creatine kinase (CK), creatine kinase-MB (CK-MB), and troponin among patients younger than 45 years in comparison to that among patients aged 45 years or older. *p<0.05, **p<0.01, and error bars represent the 95% confidence interval.

- Lipid profile and length of hospital stay for patients younger and older than 45 years. A-B) Mean low-density lipoprotein cholesterol (LDL) and total cholesterol in the two populations. C) Mean duration of hospital stay (in days) in patients younger and older than 45 years. *p<0.05, and error bars represent the 95% confidence interval. Hosp: hospital, Chol: cholesterol
An invasive strategy was more commonly employed in the younger group than in the older group (66% vs. 52%). Thrombolysis was performed on 32 (16.2%) young patients and 38 (18%) on the elderly group (Table 2). Referral to CABG capable centers was more common among the older patients compared to younger patents (1 vs. 5, p=0.1) (Table 2). Pulmonary edema (Killip III) and cardiogenic shock (Killip IV) were more common in the elderly (5 vs. 21; odds ratio, 4.43; 95% confidence interval, 1.750-10.94z) (Table 2). Other complications, such as cardiac arrest occurring pre-hospitalization or during hospital admission; arrhythmias, including atrial fibrillation; and in-hospital MACE, including death, stroke, and acute kidney injury, did not show statistically significant differences between the 2 groups (Table 2). Hospital stays were significantly longer in the older group than in the younger group (4 ± 2 vs. 5 ± 2 days, p=0.02) (Figure 2C).
Discussion
In the present study, we analyzed the clinical profiles of adults younger than 45 years of age who presented with STEMI and compared them to those of older patients. We found that young patients were more frequently smokers and had high dyslipidemia prevalence. The pathophysiology of STEMI in young patients can be different from that in the older population.2 Although atherosclerosis and plaque rupture are the most common causes of STEMI, younger patients are more prone to having coronary spasms, coronary spontaneous dissection, and vasculitis as underlying factors for acute coronary artery blockage. Moreover, histopathological studies have shown that atherosclerotic plaques in the younger age group develop more quickly and contain more lipids with a relative lack of cellular scar tissue compared to plaques seen in older patients.19 These plaques are considered highly vulnerable and prone to rupture; thus, they are more likely to cause STEMI than chronic stable angina at a younger age.20 Indeed, in our analysis, the prevalence of dyslipidemia was high in younger patients (60%). Forty-four percent of those patients did not report having a history of dyslipidemia or receiving any treatment, with only 16% being aware or receiving treatment. Although diabetes and hypertension were more prominent in the elderly, potentially due to aging and a higher prevalence of obesity,21 the dyslipidemia burden was similar between the 2 groups. Indeed, the immense burden of dyslipidemia among AMI patients has been reported locally and regionally.22,23
Furthermore, coronary artery vasospasm complicating coronary atherosclerosis can lead to thrombus formation, which can cause AMI and even sudden cardiac death; however, spontaneous coronary reperfusion may occur in the early stages of myocardial infarction.24 Cigarette smoking is a major risk factor for both atherosclerosis and spasm, and endothelium-mediated vasodilation has been found to be impaired in smokers.25 In the present study, we found that smoking was a prominent risk factor among young patients. Indeed, this is a well-documented risk factor for STEMI in youth, where several groups have reported smoking prevalence rates as high as 70%-90%,1,26,27 which is more than that reported in our study (52%). In local epidemiological surveys, smoking is more prevalent among men (22%) than women (1%).16 This may explain in part the predominance of male STEMI patients (97.5%) in our study. Furthermore, male gender is a major risk factor for STEMI, where female patients frequently present with non-STEMI or unstable angina.28,29 These findings shed light on the relationship between gender, smoking, and lipid profile in the early precipitation of STEMI. Several international guidelines have suggested early screening and treatment of dyslipidemia in patients as young as 25 years or younger, especially if they are smokers.30 The early introduction of statin therapy has resulted in a reduction in AMI rates.31
We observed a long symptom to door time in both age groups, which can be attributed to the inclusion of multiple late presenters (3-7 days). Although atypical presentation is frequently reported in older STEMI patients, we did not observe any difference between the 2 groups.32 However, the incidence of pulmonary edema and cardiogenic shock was approximately 3-times higher in elderly patients (10% vs. 3%). This can be attributed to the increased arterial stiffness, multiple comorbidities, and multi-vessel involvement that are usually found in the aforementioned group.33 Another related manifestation is the longer hospital stay observed in the same group, which can be attributed to the same reasons. In contrast, younger patients commonly present with single-vessel disease.34 The acute occlusion of a single vessel without established collaterals can explain the observed higher levels of CK, CK-MB, and troponin in young patients. With that, having a history of AMI and post-STEMI referral to CABG were less common among younger patients which further emphasize the difference in the extent of CAD between the 2 groups.
In our study, we discovered that 44% of young STEMI patients were unaware of their dyslipidemia status. The gap in their knowledge regarding the preexistence of such a condition is a potential driver of their premature presentation.35 Therefore, strict implementation of screening programs for dyslipidemia starting at a young age, especially for those at risk, such as smokers or those with a family history of AMI, is warranted. The age at which screening is initiated may differ from one region to another, along with local guidelines.36 Currently, the local guidance for dyslipidemia screening is focused on people aged 45 years or older.37 However, the youngest patient present with STEMI in our study was a 26-year-old man. Therefore, regional calls to establish and implement screening programs for dyslipidemia in young individuals are proliferating.35,38 On the same note, smoking remains an important modifiable risk factor for AMI in young individuals, and the high prevalence of this habit in the region has proven to be detrimental. Tackling both problems will require national coordinated efforts to establish screening guidelines as well as preventive task forces. Our work will serve as a regional and national reference for such diseases, along with its related comorbidities. Finally, we encourage further research on this topic and other related pathologies, such as stroke and renovascular diseases, in young patients to maximize our understanding and provide a basis for future regional guidance.
Study limitations
The present study was a single-center, retrospective case-control analysis. The data regarding newly-diagnosed diabetes and hypertension were missing for a number of patients, and thus were excluded from the analysis. Data regarding the number of vessels involved, number and type of stents deployed, cannot be retrieved for some patients also not included in the analysis. Furthermore, data on long-term all-cause mortality, re-hospitalization, recurrent AMI, stroke, and subsequent revascularization were not included since we lost follow up for large number of patients. Finally, our study design precludes the calculation of the prevalence and incidence of STEMI in young individuals, and our relatively small sample size may result in misjudgment of some analyses provided.
In conclusion, individuals younger than 45 years of age presenting with STEMI are predominantly smokers or having dyslipidemia. The majority of young patients with dyslipidemia are not aware of their pre-existing condition. In terms of outcome, younger patients are less likely to develop pulmonary edema and cardiogenic shock, and more likely to have a shorter length of hospital stay. Smoking prevention, adaptation, and implementation of a screening program for dyslipidemia with subsequent intervention for those at risk might decrease the burden of STEMI in young patients. Further regional studies on the burden and implications of AMI and dyslipidemia in young individuals are needed.
Acknowledgment
We thank Dr. Amal Aqqad, Dr. Ghayda Kullab, Dr. Ahmad Ramzy, and Mr. Saad Alsomali for their valuable contributions during the data collection process. We also would like to acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 13, 2021.
- Accepted September 28, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.