


Abstract
Objectives: To evaluate the demographic data and complications in children who had undergone percutaneous endoscopic gastrostomy (PEG) over 9 years period.
Methods: The demographic data, complications, length of hospital admission related to PEG insertion and follow-up findings of 39 patients who had undergone percutaneous endoscopic gastrostomy using the standard pull-through technique between 2011 and 2020 were examined. The study took place at the Gastroenterology Division, Department of Pediatrics, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Results: The most common indications of feeding with a gastrostomy tube include neurological diseases (n=30, 76.9%), followed by metabolic disorders (n=3, 7.69%), chronic diarrhea (n=2, 5.1%), chronic kidney diseases (n=2, 5.1%), cystic fibrosis (n=1, 2.56%), feeding aversion fibrosis (n=1, 2.56%). Out of the 39 patients, 20 (51%) did not have any complications. However, minor complication are expected. Most common complications included local infection (n=14, 35.89%) followed by granulation tissue (n=6, 15.38%), “buried bumper syndrome” developed in one.
Conclusion: Percutaneous endoscopic gastrostomy tube is the desirable method for patients who are unable to feed orally, feeding is not adequate for demands, has special feeding requirements, or swallowing dysfunction. The technique has become more widespread because of its simplicity, safety, and low cost. Major complications are rare. The procedure is safe and effective and could be carried out by pediatric gastroenterologists after training.
To maintain the normal growth and development of a child, a sufficient energy and nutritional requirements should be provided. Providing sufficient energy and nutrition play a significant role in management of the primary disease. Normally, nutrition is provided orally. However, when energy and nutritional requirements cannot be administered orally, enteral feeding is used.1 Nasogastric, nasoenteric tube, gastrostomy (GT), and enterostomy tubes have been used before. It is preferred that enteral feeding is administered through the stomach. Feeding through the stomach is more physiological.2 Moreover, pancreatic enzymes functioned and controlled as the passage of the nutrients from the stomach to the small bowel.3 A gastrostomy tube can be inserted using endoscopically, radiological, or surgical methods. The most common method in pediatric age group is percutaneous endoscopic gastrostomy (PEG), developed by Gauderer in 1980. Nowadays, PEG tube is becoming the preferred method to deliver medication, fluid, and food in children who do not have sufficient oral intake. Previously, the main approach was an open surgical gastrostomy.4 In 1980, the first PEG tube insertion was reported.5 Since then, it is rapidly becoming the technique of choice. The aim of this study is to evaluate the demographic data, complications, and length of hospital admission in children who had undergone PEG.
Methods
This is a retrospective study of all children who underwent PEG procedure between 2011 and 2020 were included in the study that took place at the Gastroenterology Division, Department of Pediatrics, Prince Sultan Military Medical City, Riyadh, Saudi Arabia. Only 2 patients were excluded after missing their follow up. The International Review Board approval was obtained from the Ethical Committee of Prince Sultan Military Medical City, Riyadh, Saudi Arabia with project number 1299. Demographic data, underlying diseases, indication for insertion, times of PEG change, procedure-related complications, and gastroesophageal reflux disease (GERD) rate were reviewed. The diagnosis of GERD was made mainly on a clinical findings. Medications after PEG insertion (proton pump inhibitor [losec and nexium] which packed by tabuk pharmaceutical manufacturing company, Saudi arabia under the license from Astrazeneca AB and prokinetics [domperidone] which also packed by tabuk pharmaceutical manufacturing company, Saudi arabia). Lengths of hospital stay after insertion and number of admissions related to PEG insertion were also gathered. Abdominal x-rays at 45 degrees were performed before the procedure to assess the presence of the colonic gas in front of the stomach and to assess the presence of scoliosis. The presence of colonic gas in front of the stomach after cleaning the bowel with laxative and presence of peritoneal dialysis were considered contraindication in our center. The procedure was performed using the pull method and requiring 2 physicians. One for endoscopic guidance and the other was for percutaneous interventions. The patient was placed in a supine position and the head was raised 45 degrees to keep the colon below the stomach. Skin sterilization was performed before the introduction of the scope to avoid excessive air, which could have dilated the colon to cross in front of the stomach. After sterilization, the percutaneous entrance was implemented in the epigastric region after considering the light of the endoscope on the skin and the fluctuation sensed by the fingers. A standard PEG set (Kimberly-Clark MIC® PEG size 14 French) or corpack size (12 and 16 French) was initially placed in all patients.
Results
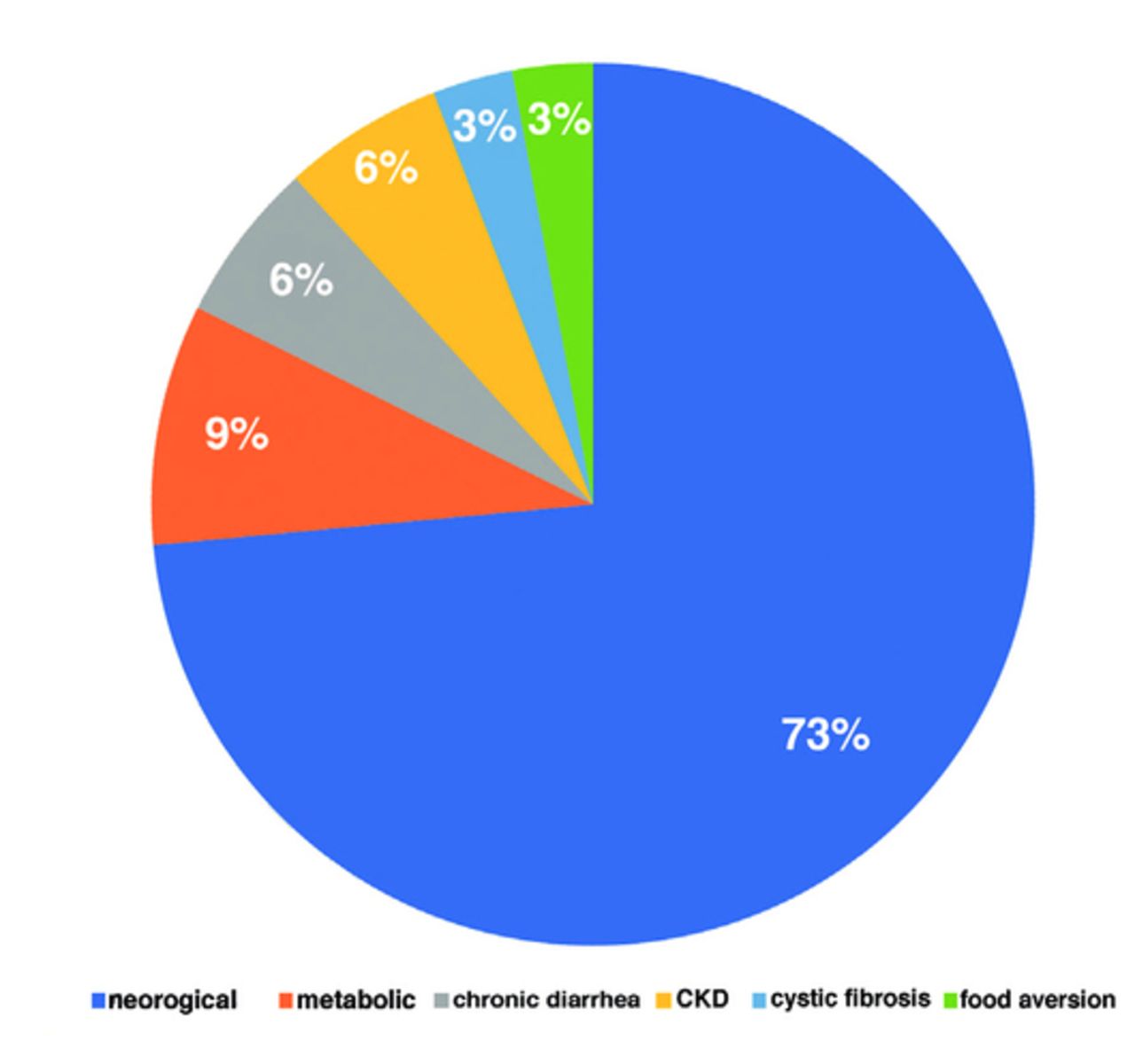
Over a 9-year-period, 39 PEG procedures were performed in 39 children. Twenty eight switched from standard PEG to button and 2 was removed. Twenty-three (59%) were male. The youngest patient was 5 months of age and the oldest was 12 years (144 months) with a mean age of 53 months. The mean weight was found to be 12 kg (3.5-34 kg). The number of patients below 2 years was 12 (30.8%). The mean length of admissions was 3.5 days. The PEG was changed to low profile GT in 17 (43.5%) of our patients. Percutaneous endoscopic gastrostomy was removed in 2 patients (5%), One of them recovered from encephalopathy and the other one was removed due to the mother’s dissatisfaction. The mean time for switching from the standard PEG to low profile GT was 8 ± 3.4 (5-12) months. Indications for change were breakages or family wishes. In this period, 2 patients (5%) died due to factors related with the underlying diseases. The families of these patients were asked by nutrition nurses who performed follow-up visits whether they would allow their children to have a PEG catheter placed again and a positive answer was obtained from all parents. The most common indications of feeding with a gastrostomy tube include neurological diseases, which impair functions, such as sucking, chewing, and swallowing (n=30, 77%) followed by metabolic disorders (n=3, 9%), chronic diarrhea (n=2, 6%%), chronic kidney diseases (n=2, 6%), cystic fibrosis (n=1, 3%), and feeding aversion (n=1, 3%) as shown in Figure 1.
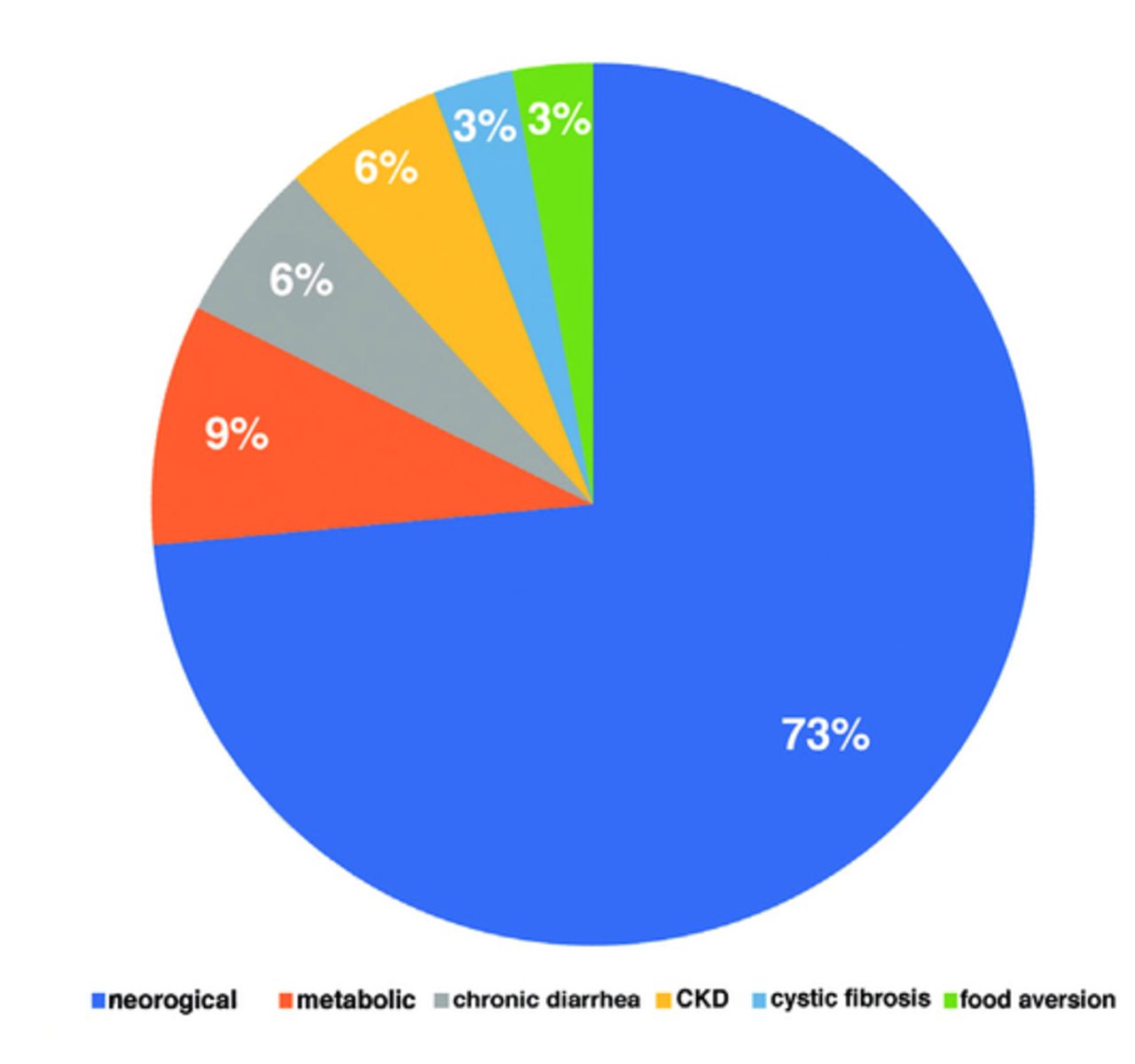
- Indications for percutaneous endoscopic gastrostomy insertion. CKD: chronic kidney disease
During the follow-up, one patient with severe onset epileptic encephalopathy with uncontrolled seizures was started on a ketogenic diet after PEG insertion. Currently, his seizures is well controlled. Twenty-seven patients were not able to take their medication for different reasons (recurrent vomiting, recurrent aspiration, or swallowing incoordination) and all of these patients show better compliance with their medications at present. Thirty patients (77%) have neurological diseases, with sucking, chewing, and swallowing incoordination, which put them at risk of recurrent chest infection. The pediatric intensive care unit admissions, due to respiratory problems, was 2.1% per year before PEG tube insertion has declined to 0.8% after PEG insertion. Our patients were examined in terms of gastroesophageal reflux (GER) before the procedure (all patients were questioned about reflux complaints, and the diagnosis of GER was made based on the clinical findings). Few of them had a gastroscopy or 24-hour pH-impedance exam. While the number of patients who used anti-reflux drugs before PEG was 19 (48.7%), this number was observed to increase to 21 (53.8%) after PEG tube insertion.
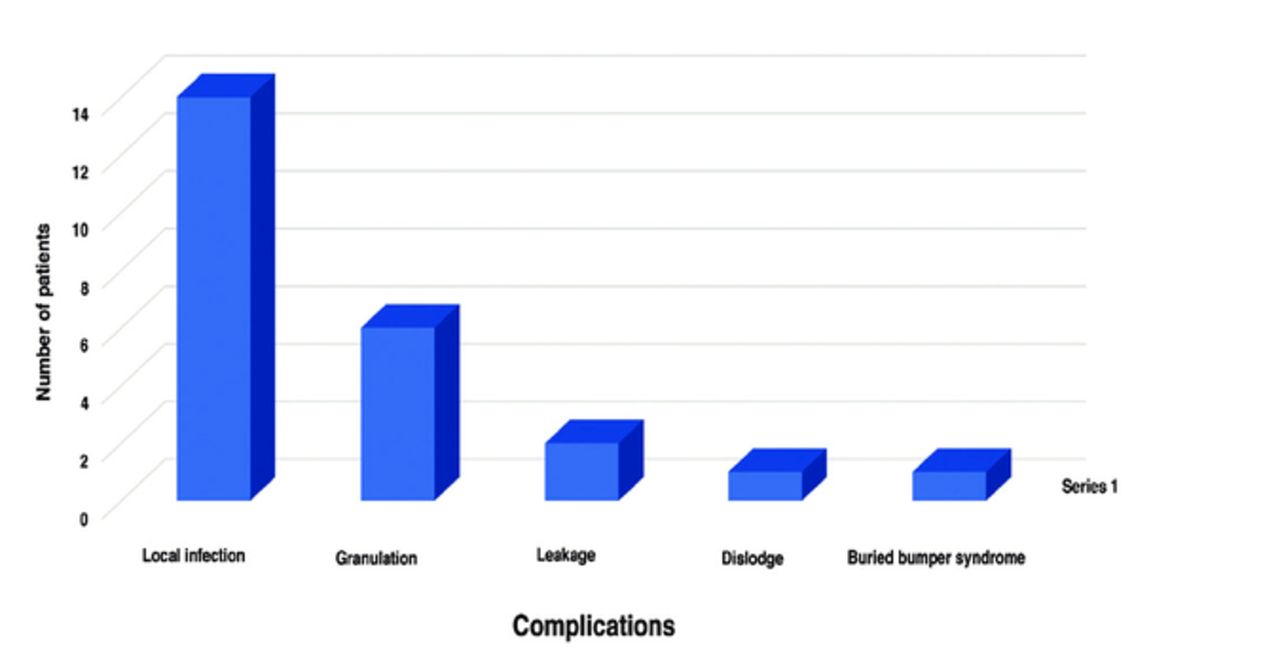
Out of the 39 patients, 20 patient (51%) did not have any complications. However, minor complication are expected after PEG insertion.6,7 Most common complications included local infection (n=14, 35.9%) followed by granulation tissue (6 patients, 15.4%), leakage (n=2, 5%), and GT dislodge (n=1, 2.6 %) as shown in Figure 2. Two patients with cerebral palsy had aspiration pneumonia after percutaneous endoscopic gastrostomy insertion. They had undergone Nissen fundoplication. “Buried bumper syndrome” developed in one patient and was removed by pulling it without complication and button PEG low profile gastrostomy tube were placed. One patient developed significant cellulitis and were treated with intravenous antibiotics. The granulation tissue was treated with local silver nitrate cauterization.

- Complication for percutaneous endoscopic gastrostomy tube insertion.
Discussion
Percutaneous endoscopic gastrostomy insertion is an endoscopic technique that allows the insertion a tube to create a tunnel between the abdominal wall and the stomach, facilitating passing of medication, fluid, and food into the patient’s stomach.8 There are a few reports in infants with PEG tubes insertion.9 The appropriate body weight for insertion of PEG in the previous guidelines was approximately 10 kg.10 Recent studies have reported the safely in young infants with and can be used in infants below one year of age and a body weight as low as 2.6 kg.11 The youngest patient in our study was 5 months old and weighed 3.5 kg. When 39 patients included in this study was examined, it was noticed that the patients with neurological problems presented the highest indication for PEG insertion. This was compatible with the large series published worldwide.12 Because of the high rate of consanguinity in our country, we have high metabolic diseases rate. Metabolic diseases are the second most common reason for PEG insertion (7.7%). This is compatible with study carried out by Srinivasan et al,13 it was reported that 160 (41.6%) of 384 subjects in whom PEG was placed had neurological problems and 7 (1.8%) had metabolic problems.
In a study by Tugba-Koca et al,8 the number of children who used anti-reflux medications increased from 16 (47.1%) to 18 (52.9%) after insertion of a PEG tube. We also observed an increase in the use of anti-reflux medications after placement of PEG tube from 19 (48.7%) to 21 (51.2%) children. In our study, 2 patients who had recurrent aspiration pneumonia after PEG tube insertion had undergone Nissen fundoplication. Although minimal evidence supported the view that the reflux symptoms increases after PEG insertion, others have reported the opposite.15,16 Puntis et al15 recommended that routine anti-reflux medication should not be used in these patients, and investigations for GERD should be avoided in patients without symptoms or signs. However, some of the outcomes could be affected by comorbidities of each patient and this consider a limitation of our study. There are major and minor complications of PEG insertion. Major complications include death, peritonitis, hemorrhage necrotizing fasciitis, and tumor implantation. Minor complications include leakage, local infection, fistula formation, buried bumper syndrome, ulcers, and accidental removal. In general, major complications are rare, while minor complications are proportionally expected.8 In a study carried out by Fortunato et al16 on 760 children with a PEG tube, local infection happened in 8% of the children and granulation tissue happened in 9% of children. In our study, the most common complication was local infection (n=12, 30.7%) followed by granulation tissue (n=6, 15.4%).
In conclusion, feeding through a PEG tube is the desirable method for patients with dysphagia, those who are unable to feed orally, feeding is not adequate for demands, has special feeding requirements (metabolic or ketogenic diet), or has significant respiratory complications due to swallowing dysfunction despite having a functioning digestive system. The technique has become more widespread because of its simplicity, safety, and low cost. Major complications are rarely observed. The procedure is safe and effective in our country and could be carried out by pediatric gastroenterologists after appropriate training.
Acknowledgment
The authors gratefully acknowledge American Manuscript Editors (https://americanmanuscripteditors.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 11, 2020.
- Accepted December 9, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.