


Abstract
Objectives: To evaluate resected congenital lung and mediastinal lesions among children and their characteristics in a single tertiary hospital.
Methods: A retrospective chart review analysis of all patients under 14 years of age who underwent congenital lung and mediastinal lesion resection in a single tertiary center from June 1997 to June 2018 was performed.
Results: In total, 108 cases of resected lung and mediastinal lesions were performed from June 1997 to June 2018. Congenital lung and mediastinal lesions were found in 52 (48%) cases. Overall, 23 cases were males (44%) and 29 (56%) were females. The most common histopathology was congenital lobar emphysema.
Conclusion: This study provides a 21-year review of the clinical and histopathological features of resected congenital lung and mediastinal lesions in a single center. Congenital lung and mediastinal lesions represented 48% of all resected lesions.
Resected lung and mediastinal lesions in pediatrics can be either congenital or acquired. Congenital lesions include congenital pulmonary airway malformation (CPAM), congenital lobar emphysema (CLE), pulmonary sequestration, and foregut duplication cysts. The pathogenesis of congenital lung and mediastinal lesions is still not fully understood; however, molecular studies suggest that different congenital lesions share a common origin.1-3 The clinical presentation of congenital lesions varies. Presentation can be in an acute setting, such as acute respiratory distress, chronic presentation with recurrent chest infections, or the patient may be asymptomatic.4-6 Furthermore, congenital lesions may be detected during fetal life by prenatal ultrasound. Additionally, chest x-ray (CXR), chest ultrasound (US), and chest computerized tomography (CT) play important roles in the diagnosis of congenital lung and mediastinal lesions postnatally. Although different imaging modalities aid in the diagnosis, histopathological diagnosis may not reflect the imaging findings.7,8
Few studies have been conducted to evaluate resected lung and mediastinal lesions among the pediatric population. Additionally, available epidemiological data show variation in the types of lesions between studies conducted in different parts of world. Locally, no known study has reviewed resected pediatric lung and mediastinal lesions. The aim of this study was to evaluate resected congenital lung and mediastinal lesions among children and their characteristics in a single tertiary hospital in Saudi Arabia.
Methods
This study was a retrospective chart review analysis of all patients under 14 years of age who underwent congenital lung and mediastinal lesion resection in a single tertiary hospital in Saudi Arabia. Any patient who was referred to our center after resection for further management were excluded. The period reviewed is from June 1997 until June 2018. Data collected included demographics, clinical presentations, investigations, type of surgical intervention, postoperative complications, and histopathological findings. All collected data was entered into Microsoft Excel 2010 spreadsheet.
For statistical analysis, IBM Statistical Package for Social Science (SPSS®) for windows, Version 22.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. Means ± standard deviation (SD) was used to represent quantitative variables. For qualitative data, frequencies and percentages were used.
This study was initiated after obtaining ethical approval from the King Abdullah International Medical Research Center (KAIMRC). The reference number of the study was RSS16-044. All the data collection forms were kept under strict confidentiality, accessible only to the data collectors.
Results
In the pediatric age group, there were 108 cases of resected lung and mediastinal lesions in a single tertiary hospital in Saudi Arabia, from June 1997 to June 2018. Of the 108 cases, 52 (48%) were congenital lung and mediastinal lesions, and 56 (52%) were acquired lung lesions. Twenty-three cases were males (44%) and 29 (56%) were females. Diagnosis of the congenital lesions included prenatal US; and with CXR, chest US and chest CT postnatally. For prenatal diagnosis, 28 (53%) cases underwent prenatal US. Nine patients were diagnosed prenatally with congenital lesions (17%), while a prenatal US did not detect any congenital lesions in 19 (36%) cases. Postnatally, all patients underwent CXR for the diagnosis of congenital lesions; however, in selected cases, chest US and CT were performed to confirm the diagnosis. Chest US was performed in 4 (7%) cases, whereas 46 (88%) cases underwent chest CT.
In 19 (38.8%) cases, emergency admission was required preoperatively, while 30 (61.2%) cases were admitted electively. Furthermore, the most common age period in which lesions were resected was between the age of 30 days and 1 year (Table 1). The type of surgical intervention performed was thoracotomy in 48 (92.3%) cases, thoracoscopy in 3 (5.8%) cases and one (1.9%) case requiring conversion from thoracoscopy to thoracotomy. Additionally, no recurrence or reoperation was required in any case. In the postoperative course, 3 (5.8%) cases had persistent air leakage, 10 (19.2%) cases had pneumothorax, 4 (7.7%) cases had pleural effusion, 2 cases (3.8%) had pneumonia and one (1.9%) case had emphysema. Postoperative mechanical ventilation was required in 14 (26.9%) cases, with a mean duration of 2.1 days ± SD 1 day.
- Timing of surgery by age period (N=52).
The most common resected congenital lung lesion was CLE, representing 18 (34.6%) cases. Other resected congenital and mediastinal lesions included CPAM, pulmonary sequestration, and foregut duplication cysts (Table 2). The distribution of lung lesions varied according to histopathology. For CLE, the left upper lobe (LUL) was most commonly observed, seen in 7 (38.9%) of the cases, followed by the right middle lobe (RML), which was seen in 5 (27.8%). In CPAM, the right lower lobe (RLL) was the most common location, seen in 6 (42.1%) cases. For pulmonary sequestration, 3 (60%) cases were in the RLL, whereas most of the cases of foregut duplication cysts were located in the mediastinum, as observed in 8 (53.3%) cases.
- Histopathology of the studied cases (N=52).
Discussion
Lung and mediastinal lesions in pediatrics can be broadly classified into congenital or acquired lesions. Studies from different regions of the globe show variation in the incidence of different histopathological resected lung and mediastinal lesions. A study in India reported that congenital lung lesions represented 60% of all resected lung lesions. In the same study, CPAM and CLE were the most common, each representing 25% of the total resected lesions.4 Additionally, in the United States of America (USA), a report of 258 resected lesions showed that more than 50% of the resected congenital lesions were CPAM.9 Furthermore, a single institution study in England showed that CPAM was the most common resected cystic lesion. In contrast, a study performed in China showed that lung abscess was the most common lesion requiring surgical intervention.10 Additionally, a study in Turkey showed that the most common lesion requiring surgery was a hydatid cyst.11
In our study, congenital lung and mediastinal lesions represented 48% of all resected lesions. Congenital lobar emphysema represented the most common, with 34.6% of resected congenital lesions, followed by foregut duplication cysts, which represented 28.8%. Although CLE is the most commonly resected congenital lesion, the trend in our institution is now leaning toward a more conservative non-operative approach. In addition, the vast majority of all congenital resected lesions are performed within the first year of life, with thoracotomy being the most common approach.
We observed in our study that only 53% of patients had a prenatal US. Despite the variable natural course of prenatally diagnosed congenital lesions, prenatal US should be offered in all pregnancies.12-15 Offering a prenatal US will aid in identifying high-risk pregnancies. Predictors of high-risk pregnancy with fetuses having congenital lung or mediastinal lesions include polyhydramnios, hydrops, and mediastinal shift.12,15,16 In patients with high-risk predictors, parental counseling and planned perinatal care should be provided to achieve the best outcomes.
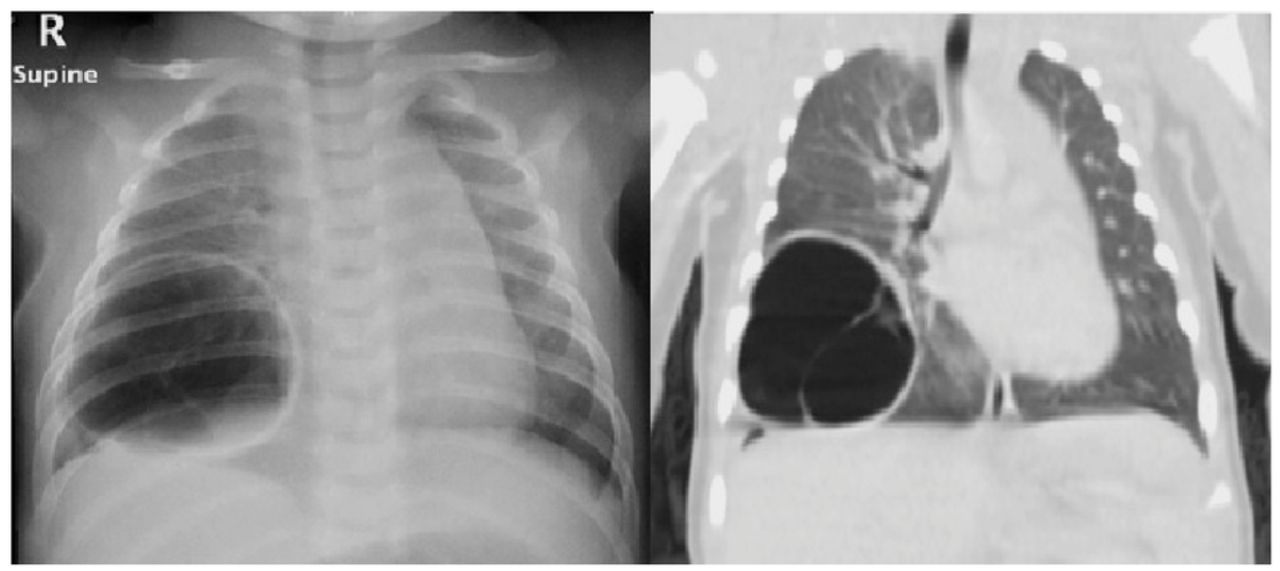
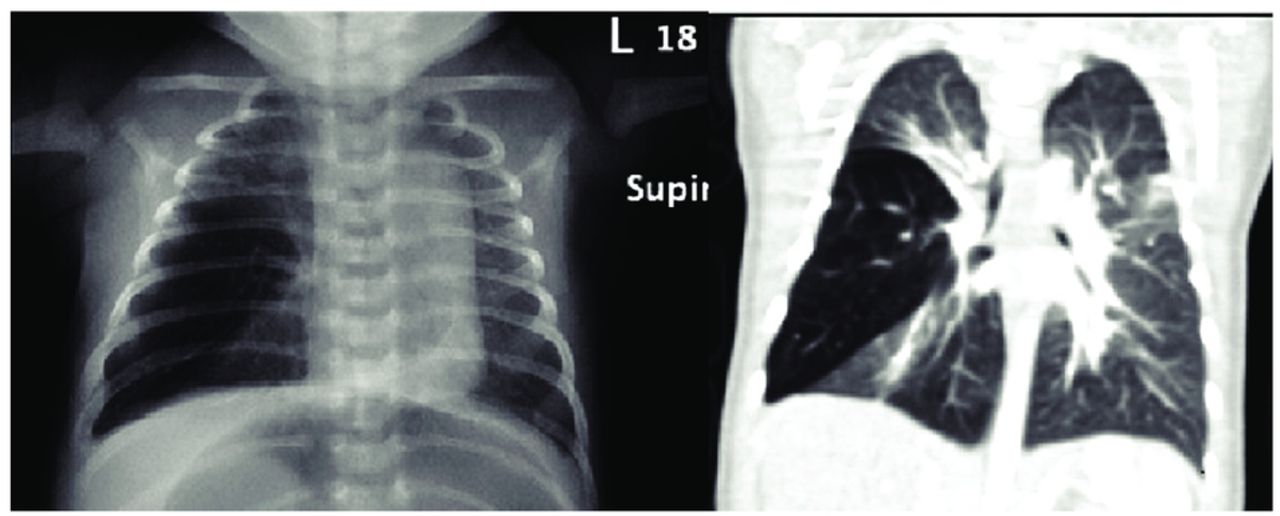
The presentation of congenital lung and mediastinal lesions varies. For symptomatic lesions, such as respiratory distress, surgical intervention is indicated (Figure 1).17,18 Due to the lack of knowledge of the natural course of congenital lung and mediastinal lesions, the role of surgical intervention in such lesions is controversial. Current indications for surgical resection of asymptomatic congenital lung and mediastinal lesions are due reported risk of malignant degeneration in some types of lesions, risk recurrent infections and pneumothorax (Figure 2).17,18
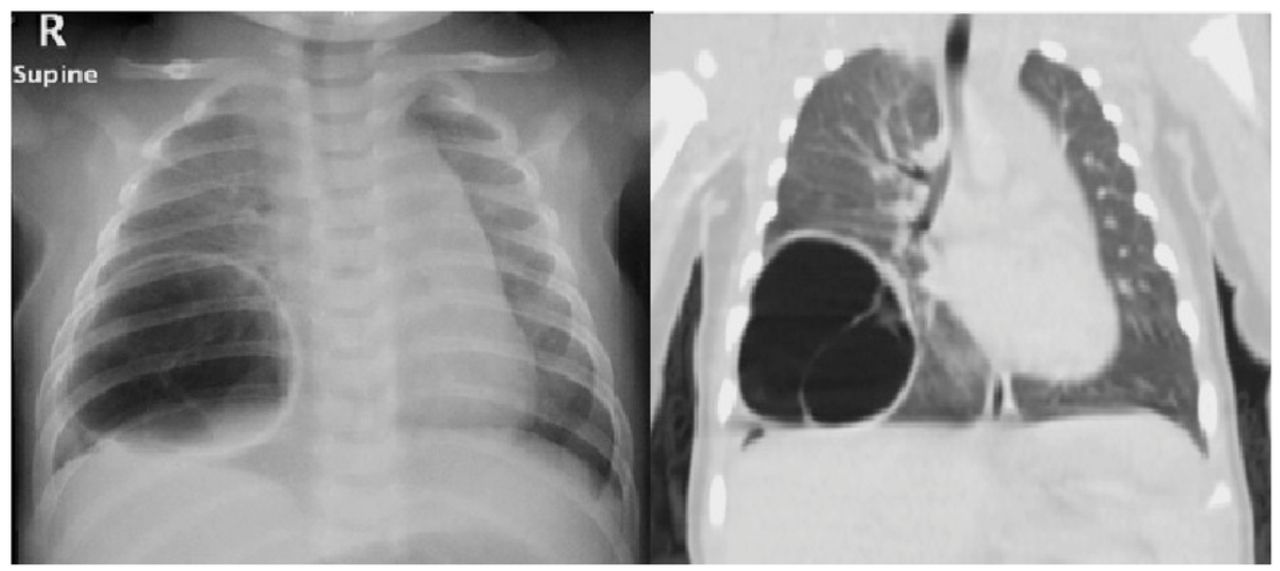
- Four-week-old child who presented to the emergency department with respiratory distress. A) chest x-ray showing hyperlucency and B) cross-section imaging showing hyperinflation of right middle lobe suggestive of congenital lobar emphysema (CLE). Patient underwent right middle lobectomy within the same admission with uneventful course. Histopathological examination confirmed the diagnosis of CLE.

- A 4 month asymptomatic female with incidental finding of A) right lower cystic lesion in the chest x-ray. B) Cross-sectional imaging showing a well-defined cystic-like lesion in the right lower lobe. Patient underwent right lower lobectomy on an elective basis. Pathology showed that the lesion was congenital pulmonary airway malformation.
Study limitation
It was a retrospective, single institution, and hospital-based review. Despite these limitations, this study provides a 21-year review of the clinical and histopathological features of resected congenital lung and mediastinal lesions in a middle eastern center, where data are limited.
In conclusion, this study demonstrate that congenital lung and mediastinal lesions represent almost half of all resected lesions, with CLE being the most common histopathological type. Further population-based studies are needed to determine the exact magnitude of congenital lung and mediastinal lesions in our region.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 21, 2021.
- Accepted January 14, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.