


Abstract
Objectives: To assess and age stratify the types and frequencies of endometrial pathologies in Saudi women with abnormal uterine bleeding (AUB) that underwent endometrial biopsies, at our hospital over a 13-year period.
Methods: In a retrospective study, from 2006 to 2018, all endometrial biopsies from Saudi women with AUB, reported at the laboratory of King Saud University-Medical City, Riyadh, Saudi Arabia, were revisited and analyzed. The women were categorized into <40, between 40-55 and >55 years of age.
Results: We analyzed 6458 biopsies. In <40 and 40-55 years’ groups cyclical endometrium was most common followed by endometrial polyps and disordered proliferative endometrium. In the >55 years’ group, atrophic endometrium was most common followed by endometrial polyps. The hyperplasias and malignancies together accounted for 7.2% of the study, majority in the >55 years’ group. Simple hyperplasia without atypia was the most common (3.9%), followed by malignancies (1.9%), complex atypical hyperplasia (0.7%), complex hyperplasia without atypia (0.4%), and simple atypical hyperplasia (0.3%).
Conclusion: Awareness of the probable spectrum of endometrial histopathologies in the various ages is useful in guiding management. Endometrial biopsies are valuable in early detection of precancerous and cancerous endometrial lesions especially in women over 40 years.
- abnormal uterine bleeding
- age stratified
- endometrial sampling and pathology
- menopause
- endometrial hyperplasia
- carcinoma
Abnormal uterine bleeding (AUB) refers to menstrual bleeding which is abnormal in terms of quantity, time duration or regularity. It can present as menorrhagia, metrorrahagia, polymenorrhoea, oligomenorrhoea, amenorrhoea, intermenstrual or postcoital bleeding. Abnormal uterine bleeding is one of the major gynecologic complaints, accounting for approximately 30% of outpatient visits to the gynecological clinic by women in the reproductive age and approximately 70% of gynecological consultations in perimenopausal and postmenopausal women.1
In 2011, the International Federation of Gynecology and Obstetrics introduced a new classification system termed by the acronym “PALM–COEIN” (polyp, adenomyosis, leiomyoma, malignancy and hyperplasia, coagulopathy, ovulatory dysfunction, endometrial, iatrogenic and not yet classified) for the common causes of AUB in non-pregnant women of reproductive age, in order to homogenize terminology.2 Common causes of AUB in female under 18 years of age includes hormonal dysregulation, pregnancy, use of hormonal contraceptive pills, pelvic infections, coagulopathies, and tumors (ovarian). In women between 19-39 years, the potential causes include pregnancy associated conditions (miscarriages, placenta previa, placental abruption, ectopic pregnancy and trophoblastic diseases), leiomyomas, endometrial polyps, polycystic ovarian disease (PCOD), hormonal contraception and endometrial hyperplasia (with or without atypia). Endometrial cancers are relatively uncommon in this age group. Endometritis, diseases of the uterine cervix, various systemic (namely, endocrine disorders) and iatrogenic (namely, drugs) conditions can also cause AUB. Regarding women aged above 40 years, the causes of AUB include anovulatory bleeding (reduced ovarian function perimenopausal women), endometrial atrophy, leiomyomas, endometrial polyps, endometrial hyperplasia (with or without atypia) and carcinoma. Abnormal uterine bleeding especially in women over 40 years of age requires detailed investigations in terms of medical history, physical examination, laboratory testing and radiological evaluation such as ultrasonography, hysteroscopy, sonohystography. Furthermore, age above 40 years, use of exogenous hormones (namely, tamoxifen), nulliparity, obesity and anovulatory cycles are risk factors for developing endometrial cancer.3,4 The decision to do sampling of the uterine endometrial lining for histopathological assessment is at the discretion of the clinician. Based on the current recommendation of the American College of Obstetricians and Gynecologists endometrial tissue sampling should be a first line procedure in the management of AUB in women over 45 years. In women younger than 45 years, any history of unopposed estrogen exposure (namely, obesity or PCOD), ineffective medical treatment and persistent AUB should be an indication for endometrial sampling.5,6 Endometrial sampling can be performed as an outpatient or as an inpatient procedure. The histopathological assessment of the tissue sample by light microscopy is the gold standard for the diagnosis of endometrial cancer and other endometrial pathologies and it has a high accuracy in identifying endometrial hyperplasia and carcinomas.7,8 For endometrial biopsy, the pipelle or dilatation and curettage methods are effective and minimally invasive methods, and in certain cases, curettage may itself be therapeutic. The possible pathological patterns observed in endometrial samples include menstrual, proliferative, secretory, atrophic and disordered proliferative endometrium, endometritis, endometrial polyps, endometrial hyperplasia with or without atypia and endometrial malignancies. For the optimal interpretation of an endometrial sample, information pertaining to patient’s age, clinical history, menstrual cycle and drug history regarding the use of exogenous hormones, ultrasound findings including the endometrial thickness should be provided to the reporting pathologist. The pathology report contributes significantly to the management in AUB. The prevalence of uterine malignancies increases with age and is most frequent in women aged 55-64 years. However, about 20% of such cancers are diagnosed in women younger than 55 years and AUB is the most common symptom in endometrial hyperplasia and carcinomas.9,10
The objective of this study is to document the spectrum of pathologies and their frequencies diagnosed in the endometrial biopsies of Saudi women that presented to our hospital complaining of AUB, over a period of 13 years. We also studied the variation in the endometrial pathologies in 3 different age groups, in order to explore the common causes of AUB in those age groups. Our hospital is a tertiary facility in the central region of Saudi Arabia and our findings reflect the range of possible causes of AUB in this region.
Methods
This is a retrospective study conducted at a tertiary level medical center, King Khalid University Hospital (KKUH), King Saud University, Riyadh, Saudi Arabia. Ethical approval was obtained from the Institutional Review Board at King Saud University-Medical City, Riyadh, Saudi Arabia (IRB number E-17-2538, reference: 20/0787/IRB). All non-pregnant Saudi women who underwent endometrial sampling at our hospital from January 1, 2006, to December 31, 2018, covering a 13-year period, were included in this study. As per routine protocol, the endometrial samples were fixed in 10% formalin solution and processed as per standard methods and stained with hematoxylin and eosin. The prepared slides were subsequently examined using a light microscope and reported by certified anatomical pathologists. Any case that was reported as malignant was examined and co-signed by 2 certified anatomical pathologists. Non-Saudi women and pregnancy related bleeding were excluded from this study. The patients were age stratified into 3 categories: i) younger than 40 years, ii) aged 40-55 years, and iii) older than 55 years. The medical records with the pathology reports of all the study cases were reviewed and cataloged according to the following variables: date and patient age at time of sampling, menstrual history, and endometrial sample histopathology report. The histopathology reports were tabulated under the following possibilities: unsatisfactory, normal menstrual patterns (proliferative, secretory and menstrual phases), atrophic endometrium and pathologies like chronic endometritis, endometrial polyp, luteal phase defect, effects of exogenous hormone therapy, disordered proliferative endometrium, simple hyperplasia (with and without atypia), complex hyperplasia (with and without atypia), and invasive malignancy. For patients who underwent follow up hysterectomy, their post-operative pathology report was also documented. Lastly, statistical analyses were performed using Microsoft excel.
Results
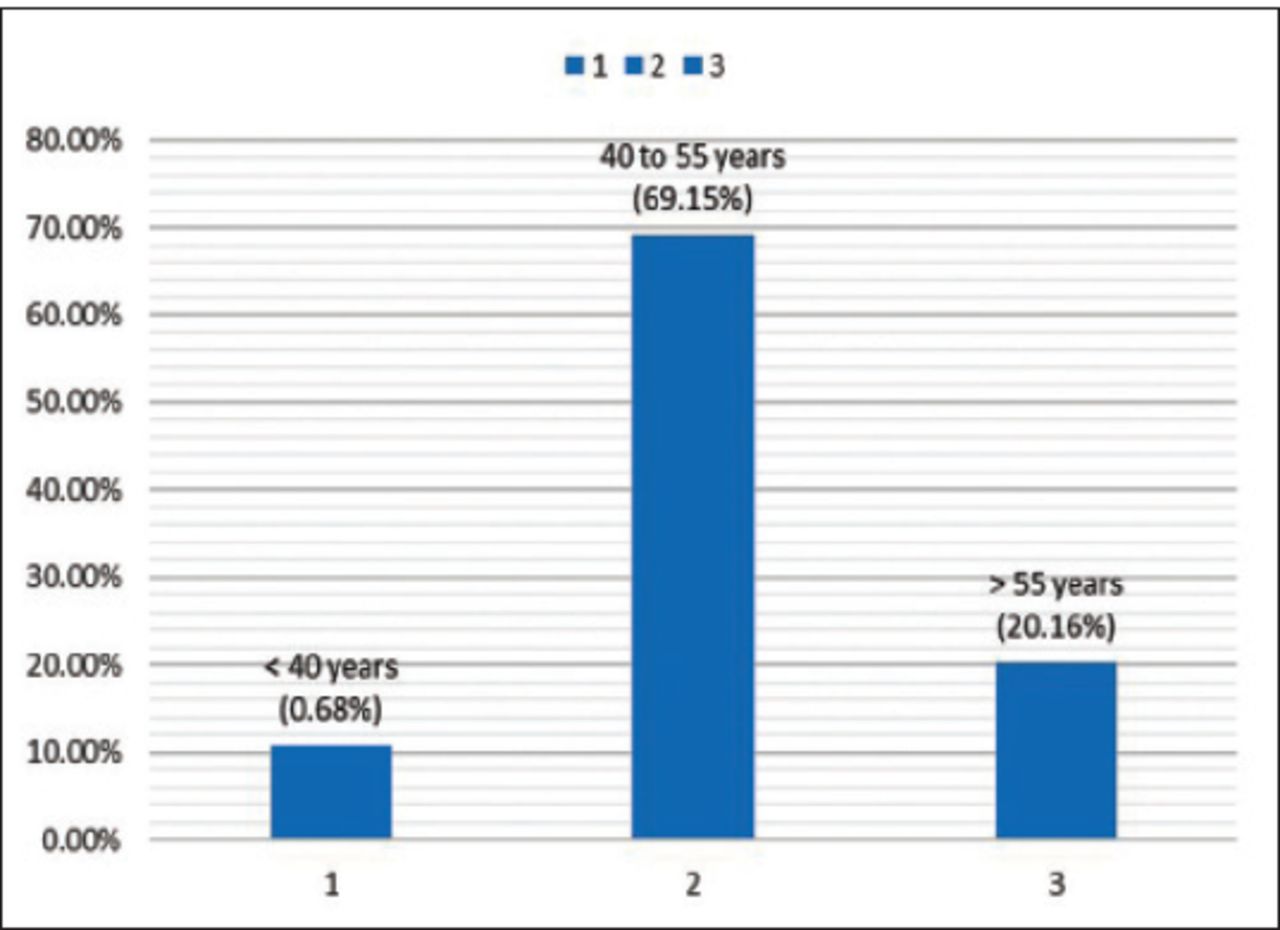
A total of 6458 endometrial biopsies were analyzed. The mean age of the women at the time of sampling was 49.5 ± 9 years. The majority (69.2%, n=4466) of our endometrial samples were from women aged 40-55 years, followed by women older than 55 years (20.2%, n=1302), and then by women under 40 years (10.7%, n=690) (Figure 1).

- Age group distribution of the study population.
Pathological findings were reported in 46.4% (n=2996) of the samples and the remaining 53.6% (n=3462) of endometrial samples of were reported as normal cyclical endometrium, atrophic endometrium or unsatisfactory for opinion (Figure 2). Normal cyclical patterns (proliferative, secretory and menstrual) amounted to 28.6% (n=1848) and atrophic endometrium accounted for 11% (n=712). A modest percentage of biopsies, 14% (n=902) were inadequate, containing blood clot and mucinous material only and were rendered as unsatisfactory for opinion. All our findings were tabulated in an age stratified manner (Table 1).
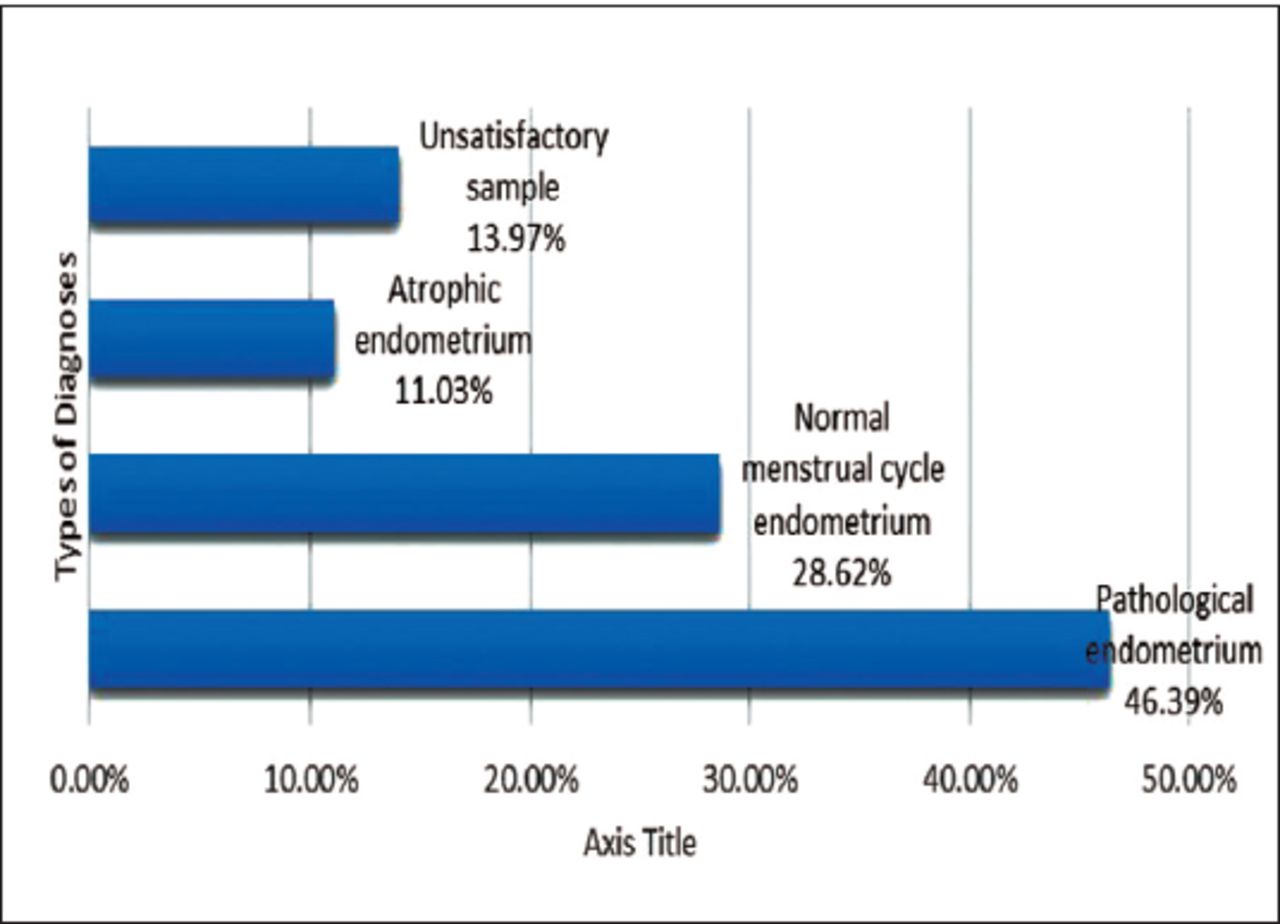
- Types of endometrial sample in the study population.
- Age stratified histopathological spectrum of endometrial samples.
Among all the endometrial pathologies (n=2996), endometrial polyps (39.3%) were the most common, followed by disordered proliferative endometrium (DPE) (27.1%), then collectively hyperplasias and malignancies (15.5%), chronic endometritis (10.3%), exogenous hormone associated changes (6.4%), and lastly luteal phase defect (1.5%) (Figure 3).
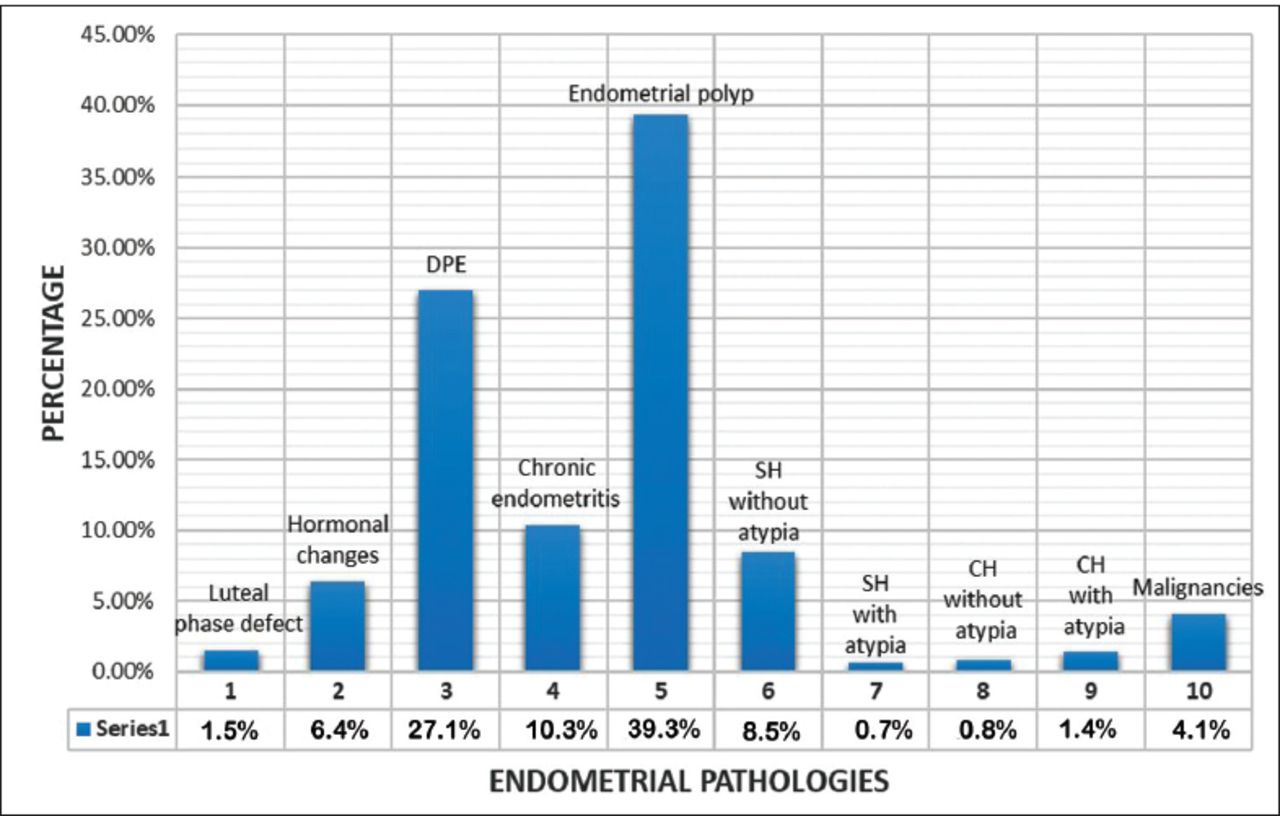
- Types and percentages of the pathological endometrial samples reported in the study population. DPE: disordered proliferative endometrium, SH - simple hyperplasia, CH - complex hyperplasia
In the below 40 years age group (n=690) the most common physiological condition was secretory endometrium (26.1%; n=180) and pathological condition was benign endometrial polyp (22.2%; n=153). Similarly, in the 40-55 years age group (n=4466) the most common physiological condition was secretory endometrium (17%; n=760) and pathological condition was benign endometrial polyp (16.6%; n=739). In the above 55 years age group (n=1302) the most common physiological condition was atrophic endometrium (29.7%; n =387) and the pathological condition was benign endometrial polyp (21.9%; n=85).
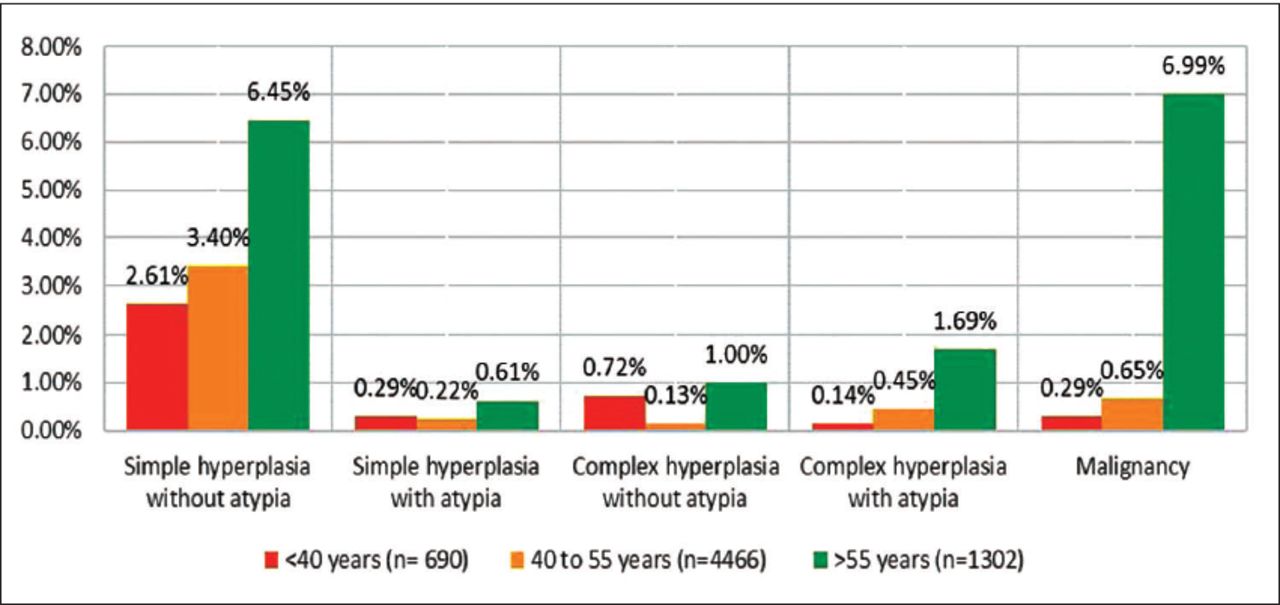
Hyperplasias (with and without atypia) and malignancies collectively comprised 7.2% (n=463) of the entire study population, in which simple hyperplasia without atypia was the most common (3.93%: n=254), followed by malignancies (1.9%: n=122), then complex hyperplasia with atypia (0.7%: n = 43), without atypia (0.4%: n=24) and finally simple hyperplasia with atypia (0.3%: n=20) (Table 1). Among the endometrial pathologies, the hyperplasias and malignancies together constituted 15.5% of all pathologies. The stratified age group study showed a rising trend with age, with the over 55 group dominating the malignancies and hyperplasias (Figure 4).

- Histogram of the age stratified distribution of the hyperplasias and malignancies in the study group.
Among the biopsies reported as malignant (n=122) (1.9% of the study population and 4.17% of the endometrial pathologies), majority were endometrial endometrioid adenocarcinomas amounting to 70.5% (n=86) of all cancers, majority belonging to the international federation of gynecology and obstetrics (FIGO) histologic grade 1 (Table 2). Other malignancies included serous carcinoma, clear cell carcinoma, mixed malignant mullarian tumors, adenosarcoma, malignant mixed Mullerian tumor, and squamous cell carcinoma of uterine cervix. The primary treatment for endometrial cancer is total hysterectomy with bilateral salpingo-oophorectomy (TAHBO). TAHBOs were performed in 73.8% (n=90) of the cases, out of which 83.3% (n=75) were reported the same as the initial endometrial sample. The remaining cases showed minor discrepancies in terms of the classification of the malignant tumor. In some cases, the FIGO grade was modified, while in others, the sub-classification of the malignancy was changed. On case turned out to be adenocarcinoma of the cervix extending into the uterine corpus, while 2 cases were reclassified as metastatic ovarian and colorectal carcinoma.
- Tabulation of the malignant endometrial reports and the follow up hysterectomies.
Discussion
Abnormal uterine bleeding is a common gynecological problem encountered by women of every age group. It has a noticeable impact on the health and quality of life, affecting 10% to 30% of women in the reproductive age.11,12 Even though the majority of women with AUB do not have a malignant or premalignant lesion, it should not be ignored, especially in postmenopausal women since the risk of endometrial malignancies in postmenopausal bleeding ranges from 3% to 25%.13 Globally, endometrial cancer is the sixth most common type of cancer in women and is the most common gynecological cancer.14,15 Hyperplasias can be precancerous, having noninvasive proliferation of the endometrium and based on architectural complexity and nuclear atypia are classified as simple or complex hyperplasia with or without atypia. Studies have shown that without treatment, the risk of non-atypical endometrial hyperplasia progressing to carcinoma is less than 5% over a 20-year period and most of such cases regress spontaneously during follow-up, with progression risk of simple (1%) and complex (3%) hyperplasia without atypia.16 Complex hyperplasia with atypia is most likely to progress to endometrioid endometrial carcinoma and it is associated with a probable coexistent endometrial carcinoma in approximately 30% to 40% of cases.17,18 The risk of a woman developing endometrial cancer in their lifetime ranges from 0.7% to 1.6% with the prevalence increasing with age.19 An estimated 3.1% of women are diagnosed with uterine cancer at some point in their life.10 Endometrial tissue sampling (pipelle or curettage) is the gold standard for a definitive diagnosis and it is the only investigation modality that may identify and differentiate endometrial hyperplasia from invasive cancer.20 The endometrium is a dynamic tissue and shows variable histological changes depending on age, phase of menstrual cycle and any other specific pathology. Assessment of endometrial samples can be a diagnostic challenge to pathologists because of the overlapping histological findings, lack of sample adequacy or inter-observer variability. The spectrum of causes of AUB is wide and variable ranging from normal physiological causes to endometrial hyperplasias and malignancies.
In this study we evaluated the type and frequency of endometrial histology encountered in a large population of Saudi women with AUB (n=6458) at our histopathology laboratory over a 13-year period. Majority of our biopsies belonged to women in 40-55 years’ age group. In women younger than 40 years of age, normal menstrual pattern was the most common histological finding. The same was true for the 40-55 years’ age group, while in women over 55 years, the most common histological finding was atrophic endometrium. Each pathological pattern encountered in our participants is detailed below.
Cyclical endometrium
A large proportion of our cases (28.6% of total study population) represented physiological cyclical endometrium (proliferative, secretory or menstrual). Bleeding during proliferative and secretory phases are usually due to anovulatory cycles or ovulatory dysfunctions and they tend to be more common around menarche and perimenopause/menopause and do not necessarily indicate an underlying pathological disease. Abnormalities of the hypothalamic-pituitary-ovarian axis leads to aberrations in ovarian follicle maturation, ovulation, or corpus luteum formation; hence, they affect the hormonal milieu and result in AUB. Around menarche, AUB is probably due to immaturity of the hypothalamic-pituitary-gonadal axis. A range of endocrine disorders that can cause ovulatory dysfunction.21
Atrophic endometrium
It was one of the most common cause of AUB in women over 55 years of age (11% of total study population). It is a response to the hypoestrogenism that occurs around menopause. The atrophic endometrial sample tends to be scanty, comprising of superficial strips of non-proliferative endometrial gland lining with little to no endometrial stroma. Notably, since there is atrophy, the scant tissue sample does not necessarily make the biopsy inadequate and such cases should be interpreted in light of patient’s menopausal status. Giannella et al,22 in their study found that approximately 90% of asymptomatic postmenopausal women with endometrial thickness of less than 7 mm showed atrophic endometrium upon being biopsied. The cause of bleeding in atrophy is not well known; it is probably a hormone deficiency related endometrial thinning, making the lining fragile and susceptible to injury and bleeding. Another theory suggests the rupture of thin-walled blood vessels around the cystically dilated atrophic glands as a possible cause.23 The world literature also documents atrophic endometrium to be the most common cause of AUB in postmenopausal women.24
Benign endometrial polyp
It was the most common endometrial pathology reported in our study (18.2% of the total study population and 39.3% of the endometrial pathologies). Majority of the cases were among women aged 40-55 years. The prevalence of benign endometrial polyps in women with AUB ranges from 20% to 40%, and their incidence increases with advancing age.25 The etiology of endometrial polyps is probably related to unopposed estrogen stimulation, leading to localized proliferation and hyperplasia of endometrial glands and stroma, which over time evolves into a polyp. In comparison to the adjacent normal endometrium, endometrial polyps exhibit increased expression of estrogen and bcl2 and decreased expression of progesterone. Cytogenetic studies indicate anomalies in chromosome 6, 7 and 12.26 Other associated conditions that may predispose to endometrial polyp formation include hypertension, obesity, late menopause, and tamoxifen therapy.
Disordered proliferative endometrium
After endometrial polyps, DPE was the second most commonly encountered pathology in our study (12.6% of the total study population and 27.1% of endometrial pathologies), and the most prevalent in the 40-55 years age group. Disordered proliferative endometrium is an exaggerated proliferative phase representing chronic anovulation in the perimenopausal years. As a result of the anovulation, the corpus luteum does not develop, culminating in relative increase in estrogen levels and a relative decrease in progesterone levels. This chronic prolonged unopposed estrogen stimulates disorderly proliferation of the endometrium with mild glandular architectural distortion, making the endometrium fragile, unstable and susceptible to subsequent shedding.27 The bleeding in DPE tends to be painless and irregular.
Endometritis
We reported a significant number of cases of non-specific chronic endometritis (4.8% of the total study population and 10.3% of endometrial pathologies) and they were mainly observed in the 40-55 years age group. The diagnosis of chronic endometritis depends upon finding plasma cells, and there may be associated spindling of stromal cells, lymphoid follicles, stromal edema, and altered glandular development. Chronic endometritis is often asymptomatic but it may present with AUB, pelvic pain or leukorrhea. In previous study,28 the overall prevalence of chronic endometritis ranges from 42% to 52% in endometrial samples of women with non-neoplastic causes of AUB. Chronic endometritis has also been documented in 10% to 11% of patients who underwent hysterectomies for benign gynecologic conditions.29,30 Many studies have demonstrated a relationship between chronic endometritis and infertility/recurrent miscarriage/implantation failure with the prevalence of chronic endometritis in such cases ranging from 3% to 60%.31 Another study suggested an association between endometrial polyps and chronic endometritis in premenopausal women with AUB.32 Due to the absence of typical clinical or ultrasound findings, the diagnosis of chronic endometritis relies on histology but histological assessment too is nonspecific and therefore a combination of histology, hysteroscopy and microbial culture is commonly used for chronic endometritis diagnosis. Endometrial culture is not routinely performed at our hospital and we do not have information regarding endometrial culture in our patients. Our study is limited by the absence of information regarding endometrial cultures of our patients.
Exogenous hormonal therapy associated changes
These were also reported in our study (3% of the total study population and 6.4% of endometrial pathologies). Progesterone compounds are commonly used to control AUB by inhibiting ovulation and endometrial growth. Histology of such cases typically show endometrial gland atrophy and decidualized the endometrial stroma. Occasional they may show hypersecretory glands.33
Luteal phase defect
It was reported in a small percentage of our samples (0.7% of the total study population and 1.5% of endometrial pathologies). It is a type of ovulatory AUB in which ovulation occurs, but the production of progesterone by the corpus luteum is insufficient, resulting in development of an abnormal poorly developed secretory endometrium.21
Hyperplasias and maligancies
Collectively the hyperplasias and malignancies (7.2% of the total study population and 15.5% of all endometrial pathologies) were most common in women over 55 years of age. Specifically, 341 of our patients were diagnosed with hyperplasias (5.3% of the total study population and 11.4% of all endometrial pathologies) out of which, simple hyperplasia without atypia was the most common. The second most common was complex atypical hyperplasia followed by complex hyperplasia without atypia. Typically, endometrial hyperplasia is due to failure of ovulation in perimenopausal women, with resultant prolonged action of excessive estrogen derived from persistent unripe ovarian follicles. In regards to malignancies, 122 of our samples were positive for cancer (1.9% of total study population and 4.1% of endometrial pathologies), the incidence being more common in women over 55 years. This was similar to reported literature that majority of malignancies were diagnosed among patients older than 55 years.34 As per world literature, approximately 90% of endometrial cancers are diagnosed in women older than 50 years, 20% are diagnosed in women before menopause, and 2% to 14% are reported in women younger than 40 years.20,35 In our study only 0.3% of participants under the age of 40 were diagnosed with cancer, and the incidence increased with age, being diagnosed in 0.7% of the 40-55 years group and 7% in women over 55 years. It is therefore incumbent that all women over 40 years of age with AUB should to undergo endometrial screening in the form of endometrial sampling for early detection and treatment of premalignant or malignant conditions. One study observed a relatively good diagnostic accuracy in detecting intrauterine malignancy when combining the parameters of being post-menopausal, symptomatic and having an endometrial thickness of more than 4 mm.36 AUB is the most common symptom of endometrial cancer and long-term chronic exposure to unopposed estrogen is the primary risk factor.20 Of the 122 cases of endometrial malignancies, endometrioid carcinoma accounted for 70.5% (n=86). Notably, 24.4% (21 out of 86 cases) and 1.64% (2 out of 86 cases) of our endometrioid carcinomas showed coexistent complex atypical hyperplasia and simple atypical hyperplasia, respectively, attesting to a clear association between atypical hyperplasia and carcinoma. Hence, it is recommended that all women with biopsy diagnosed atypical hyperplasia should receive definitive surgical management as the risk of coexistent cancer is high. The overall results of our study are in tandem with and comparable to data reported in existing literature.37,38 The relatively lower frequency of endometrial carcinoma in our study population can probably be attributed to early childbearing and multiparity.
Unsatisfactory for opinion
A proportion of endometrial specimens were render unsatisfactory for opinion in our study (13.9%) as they only presented blood clots or mucin. There is limited literature available on the criteria for adequate and inadequate endometrial specimen. Approximately 20% (n=186 186/902) of our unsatisfactory samples were from women in the over 55 years; the unsatisfactory nature of the sample may be attributed to the menopausal atrophy of the endometrium. One study suggested that an inadequate endometrial sample reflects a non-neoplastic condition and is enough to rule out endometrial hyperplasia and malignancy; they did so by demonstrating that an inadequate sample has a high negative predictive value in diagnosing endometrial neoplasia.39 Another limitation in endometrial biopsies is that the sample might not be collected from the entire endometrium; hence, a lesional area may be missed, yielding an inaccurate report. Especially in a blind biopsy, if the cancer is focal it can be missed. In order to prevent this, we recommend correlation with the thickness of endometrial wall rendered on ultrasound. Also, simultaneous hysteroscopy will provide additional information. It has been demonstrated and recommended, that in case of asymptomatic women, a cut off value of endometrial thickness of 8 mm or more can be used as an indication to perform hysteroscopy and subsequent biopsy, in order to detect endometrial pathologies.40
Study limitations
The current study did not correlate our biopsy pathologies with the corresponding endometrial thicknesses. In addition, the participants of this study were considered as symptomatic and having AUB based on the participants self-assessment of their menstruation. Also, for some of our malignant endometrial biopsies we did not have information on the follow up hysterectomies. The major strength of our study lies in the large sample size and data pertaining to Saudi women, thereby enabling good representation of this community for analysis of such disorders.
In conclusion, endometrial sampling is a crucial diagnostic modality used in the management of women with AUB. It demonstrates the hormonal response of endometrium and is a reliable indicator that provides information regarding probable specific and nonspecific causes of AUB, and yielding a range of patterns from normal endometrium to malignancy. The majority of our patients with AUB presented with normal cyclic endometrium, followed by endometrial polyps and disordered proliferative endometrium. Malignant lesions were the least common patterns observed in our endometrial samples. This study also demonstrated that different age groups are associated with different patterns of AUB, normal physiological changes were the most common finding in women under 40 years of age. The 40-55 years’ age group too showed normal physiological changes along with a substantial number of DPE and endometrial polyps. Endometrial hyperplasia and endometrial malignancies were more common in the perimenopausal and postmenopausal women. However, regardless of age, irregular menstrual bleeding warrants a thorough investigation and it is essential to perform endometrial sampling with histopathological evaluation in all women over 40 years, in order to rule out the possibility of pre-neoplastic conditions or malignancy. The accurate analysis of endometrial samplings and timely diagnosis of pre-neoplastic and neoplastic conditions are the keys to optimal and effective management, as prognosis is excellent in early detection of tumors. The importance of endometrial sampling and histopathological evaluation in women with AUB, to guide further management, cannot be overemphasized, especially in perimenopausal females.
Acknowledgment
We, the authors would like to acknowledge and extend our appreciation to the Deanship of Scientific Research at King Saud University, Riyadh, Saudi Arabia, for their valuable support.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 19, 2020.
- Accepted February 8, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.