


Abstract
Objectives: To examined the impacts of chronic pain on depression and poor sleep quality dimensions as well as the mediating function of poor sleep quality in the pathway between chronic pain and depression.
Methods: Between March 2019 and February 2020, we conducted a cross-sectional study on 233 chronic pain patients in 2 tertiary hospitals in Riyadh, Saudi Arabia.
Results: Of the 233 patients, 36% had depression, while 66.1% had poor sleep quality. Chronic pain intensity and pain disability significantly explained 10.9% of depressed affect variance, 4.9% of anhedonia variance, 17.3% of somatic complaint variance, 4.5% of interpersonal difficulty variance, 7.4% of sleep efficiency variance, and 15% of perceived sleep quality variance. The result also showed a positive, direct effect of chronic pain on poor sleep quality, which in turn positively and directly affect depression. However, chronic pain had only indirect effect on depression.
Conclusions: Among chronic pain patients, the high rates of poor sleep quality and depression requires a special attention. Chronic pain intensity and disability predict depression and sleep quality dimensions differently. The result underlines the need of managing poor sleep quality to address depression in the context of chronic pain.
Chronic pain is persistent pain that lasts more than 3 months1 and more than the expected healing period.2 It has deleterious effects on patients’ health, daily activities, and workplace productivity.3 Its tenacious nature contributes to the co-occurrence of depression and poor sleep quality.4 Of all patients with chronic pain, 22.9%-60.8% meet the criteria for depression.3,5,6 Chronic pain explains the variance in depression,7 which might occur as a result of the shared neuroplasticity alterations and underlying processes between chronic pain and depression.8 There is still uncertainty related to the question of whether depression occurs before the onset of chronic pain or due to the persistent and enduring pain.9 The diathesis-stress framework posits that chronic pain might lead to unpleasant sensory and troubling emotional feelings, which, in turn, create a sense of helplessness and hopelessness and result in the development of depression symptoms.10 The criteria for depression include sleep difficulties.11 An overlap between depression and sleep disturbance has been found,12 which occurs as a result of changes in the dopamine system13 and the serotonin and proinflammatory cytokine levels.14 Chronic pain also disturbs the patient’s sleep quality because he/she struggles to fall or stay asleep.9 Sleep quality refers to the extent of night-wakefulness, which is due to sleep latency, efficiency, arousal, and/or the number of awakenings Chronic pain patients suffer from more sleep.15 disturbances;16 40.7%-86% of patients with chronic pain have sleep disturbances.17,18 Chronic pain and sleep share the same neurophysiological mechanisms.19 In addition, chronic pain has a stronger effect on sleep disturbance than sleep on chronic pain.20
There are still inconsistencies related to the relationship of chronic pain with both depression and sleep quality, which might be due to measurement issues. Some studies only measured the total pain intensity using various scales, such as the McGill pain questionnaire,21 brief pain inventory,3 visual analog scale,22 or only a single question on whether the patient has chronic pain.23 These measurements assess current pain or pain during the last week and have an inadequate comprehensive and multidimensional viewpoint related to chronic pain that lasts for more than three months.10 With regard to depression, using the categorical or overall total score is inappropriate, because it does not capture the heterogeneousness of the underlying dimensions of depression symptomology.24 There is a need to better understand how chronic pain affects the symptoms of depression.25 A diagnosis of depression is based on the manifestation of depressive symptoms.11 Thus, identifying the effect of chronic pain on these depressive symptom dimensions is crucial for a comprehensive assessment, diagnosis, and management, as well as for developing interventions for the management of chronic pain. Similarly, sleep quality is a multidimensional, complex construct;26 therefore, to understand its nature, a special consideration of the underlying dimensions is needed.
A limited body of literature has examined the mechanisms by which chronic pain, poor sleep quality, and depression are related. Three different mechanisms have been investigated. Some studies have reported that sleep affects chronic pain intensity through depression,17 while others have shown that chronic pain leads to sleep disturbance27 and is mediated by mood issues, including depression, and still, others have reported that chronic pain affects depression through sleep disturbance.28,29
The majority of existing evidence originates in Western countries, which limits its generalizability to other contexts. Pain is a subjective experience that is shaped by the patient’s physiological and psychological aspects, in addition to sociocultural and environmental circumstances.2 Ethnicity and cultural background differences also affect chronic pain and related outcomes.30 The sequels of chronic pain must be studied in different sociocultural contexts to fill the gap in the existing body of evidence related to the influences of chronic pain.31 In Saudi Arabia, chronic pain and its high impact are evident among the adult population (46.4% and 4%, respectively).32 However, the pathway through which chronic pain is related to depression and sleep quality has not been examined in Saudi patients. Thus, among chronic pain patients in Saudi Arabia, this study assessed the extent of depression and poor sleep quality, examined the effect of chronic pain on depression and sleep quality dimensions, and investigated the pathway by which chronic pain affects depression. Based on the diathesis-stress framework and existing evidence,10 we hypothesized that chronic pain positively affects depression directly and indirectly through the mediating function of poor sleep quality.
Methods
We conducted a cross-sectional study involving 233 patients with chronic pain from the specialty pain clinics of 2 main tertiary hospitals in Riyadh, Saudi Arabia between March 2019 and February 2020. The patients were screened for eligibility to participate in the study while they were waiting for regular appointments. The inclusion criteria were chronic pain diagnosis, Saudi citizenship, adults, and willingness to provide consent. Ethical permission was granted by the institutional review boards of King Saud University (E-19-3719) and the Saudi Ministry of Health (19-146E). Before collecting the data, informed consent was provided and explained to each participant. Structured interviews were conducted with 233 patients to collect data. Since the minimum required sample size for structural equation modeling (SEM) is 200 participants,33 the current study sample was considered appropriate.
The survey questions were assessed the patients’ background, including age, gender, education, income, hours of exercise, and smoking status.
Chronic pain
The Chronic Pain Grade (CPG) scale,34 which has 7 items, was used. It evaluates chronic pain during the last 6 months with 2 subscales: pain intensity and pain related disability. First, the pain intensity has 3 items that assessed present, worst, and mean pain intensity based on 10 points Likert scale. Second, the pain disability assesses the hindrance of pain in performing everyday activities and the change in the capacity to take part in activities and work based on 10 points Likert scale. One item asks about the number of days during the last 6 months when routine activities (for example, work or housework) could not be performed owing to the pain. The CPG scale can also be categorized into 4 grades based on pain intensity and disability points. The CPG scale has been validated in different languages.35 In the present study, we utilized the Arabic version of the CPG scale,36 which is also reliable, with a Cronbach’s alpha value of 0.916 for pain intensity and 0.815 for pain disability.
Depression
We used the Center for Epidemiologic Studies-Depression (CESD) scale,37,38 which quantifies the symptoms of depression. Using 20 items, the participants rated how frequent they suffer from depressive symptoms based on 4 points Likert scale throughout the last week. The total score ranges from 0 to 60, with a higher score reflecting higher depression and a score of 16 or more indicating depression, which is in alignment with depression criteria from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition. The CESD has 4 subscales: depressed affect, anhedonia (lack of positive affect), somatic complaints, and interpersonal difficulties. It is reliable and valid in different populations,39 including patients with chronic pain.40 The structure of the CESD scale’s factors is also applicable to patients with chronic pain.41In the present study, the CESD Arabic scale42 was used, and it has also an evidence of reliability, with a Cronbach’s alpha value of 0.867.
Poor sleep quality
The Pittsburgh Sleep Quality Index (PSQI)43 was used to evaluate poor sleep quality. The PSQI has 18 items that assess a patient’s overall sleep quality by measuring 7 components: usage of sleep medications, sleep duration, sleep quality, sleep latency, sleep efficiency, sleep disturbance, and daytime dysfunction. The total score ranges from 0 to 21, with a higher score indicating poor sleep quality, and a score of more than 5 reflecting sleep problems. The PSQI is reliable and valid in different populations,44 including patients with chronic pain.45 Among patients with chronic pain, sleep efficiency and perceived sleep quality are supported as scale subscales.46 In this study, we used the Arabic version of the PSQI,47 which has a reliability score of 0.752.
Data analysis
Data were analyzed using SPSS Statistics version 26 (IBM Corporation, Armonk, NY, USA). The extent of missing data for the study’s variables ranged from 0% to 3.9%. Little’s test was not significant, indicating that data were missing completely at random (MCAR). Thus, missing values were imputed by using expectation maximization. We performed descriptive statistics to analyze the patients’ background characteristics and study variables. Normality of the distributions was assessed based on skewness and kurtosis indices. Data were considered non-normal for a skewness index >3 and kurtosis index >10.33 At the item level, the skewness index ranged from 0.13 to 4.0, while the kurtosis index ranged from 0.08 to 16.32, indicating that univariate normality was not met; therefore, the multivariate normality was deviated. Correlational analyses were performed to assess the relationship between the study variables and patient characteristics.
Mplus version 8 was used to conduct confirmatory factor analysis to test the uni-dimensionality of depression and sleep quality, and then the supported underlying dimensions.41,46 Subsequently, multiple linear regression analyses were conducted with chronic pain intensity and pain disability as independent variables to predict depression and sleep quality dimensions. Kruskal-Wallis analysis of variance was conducted to assess how depression and sleep quality symptoms differed based on the four chronic pain categories. Using Mplus, we performed SEM to test our hypothesis using the robust maximum likelihood method to correct for non-normality. The fit indices, chi-square (χ2), comparative fit index (CFI), Tucker-Lewis Index (TLI), root-mean-square error of approximation (RMSEA), and standardized root-mean-square residual (SRMR), were used for examining the model fit with the data. For adequate fit, the index values were as follows: CFI and TLI ≥0.90, RMSEA <0.08, and SRMR <0.08.
Results
Table 1 lists the patients’ background characteristics. Their mean age was 51.32 years (standard deviation [SD] = 14.344; range = 18-87 years). Of the 233 patients, 67% were women, and only 32.2% were employed. Their education level varied: 15.5% were unable to read or write and 28.7% had a university or college degree. In addition, their personal income varied from 34.3% earning up to SR2000, whereas 11.6% earning SR10001-15000. The pain was located at different sites, but most of the patients (44.2%) suffered from back pain. On the CPG scale, 7.7% of the patients had Grade I (namely, low pain disability with low pain intensity), 31.3% had Grade II (namely, low pain disability with high pain intensity), 58.8% had Grade III (namely, high pain disability with moderately limiting pain), and 0.9% had Grade IV (namely, high pain disability with severely limiting pain). The mean number of exercise minutes/day was 26.52 (SD=45.07; range: 0-240). On an average, patients smoked 3.25 cigarettes/day (SD=8.73; range: 0-80).
- Background characteristics of study participants (N=233).
Descriptive results for study variables
The descriptive results are presented on Table 2. The mean pain intensity score was 73.45 (SD=21.21; range: 10-100), and the mean pain disability score was 68.56 (SD=23.91; range: 10-100). The mean depression score was 15.78 (SD=9.11; range: 0-53), and the mean score of poor sleep quality was 7.68 (SD=3.68; range: 1-18.81). Of the 233 patients, 36% had depression, while 66.1% had poor sleep quality.
- Descriptive statistics for study variables (N=233).
Kruskal-Wallis non-parametric analysis of variance showed significant between-group differences in the symptoms of depression (χ2 [3] = 5.878; p=0.001) and sleep quality (χ2 [3] = 7.183; p=0.000); here, the Grade IV group exhibited the worst symptoms of depression and the poorest sleep quality. The relationship of chronic pain intensity and pain disability with background characteristics showed a non-significant relationship; however, we found significant relationships between the number of smokes and chronic pain intensity (r=0.196; p=0.003) and pain disability (r=0.153; p=0.020). An independent t-test showed significant differences between smokers and non-smokers in chronic pain intensity (t [230] = 3.48; p=0.001) and pain disability (t [230] = 2.46; p=0.014).
Confirmatory factor analysis
For the CESD scale, the unidimensional model (1-factor) had poor fit with the data; the goodness-of-fit indices were as follows: χ2 (170, N=233) = 936.29, CFI=0.708, TLI=0.673, RMSEA=0.139 (90% confidence interval [CI]: 0.130-0.148), and SRMR=0.113. For the 4-factor model, the goodness-of-fit indices showed that the underlying depression dimensions (depressed affect, anhedonia, somatic complaints, and interpersonal difficulties) adequately fit the data, allowing item 3 from depressed affect to co-vary with item 19 from interpersonal difficulties. The goodness-of-fit indices were as follows: χ2 (163, N=233) = 356.392, CFI=0.926, TLI=0.914, RMSEA=0.070 (90% CI: 0.060-0.080), and SRMR=0.046. The standardized factor loading for the subscales were significant, ranged from 0.50-0.89.
For the PSQI, the unidimensional model had poor fit with the data; the goodness-of-fit indices were as follows: χ2 (14, N=233) = 59.48, CFI=0.782, TLI=0.673, RMSEA=0.118 (90% CI: 0.088-0.150), and SRMR=0.066. An excellent fit of the data, with the following goodness-of-fit indices: χ2 (13, N=233) = 18.97, CFI=0.971, TLI=0.954, RMSEA=0.044 (90% CI: 0.00-0.085), and SRMR=0.038, was found to support the 2-factor model (sleep efficiency and perceived sleep quality). The standardized factor loading for the subscales were significant, ranged from 0.41-0.85.
Effect of chronic pain on both depression and sleep quality dimensions
Table 3 lists the unstandardized and standardized regression coefficients, as well as the explained variance (R2) and F-statistics values for each regression analysis. For each depression dimension as a dependent variable, the analysis showed that a linear combination of chronic pain intensity and pain disability significantly predicted depressed affect (F [2, 230] = 14.00; p=0.000), anhedonia (F [2, 230] = 5.96; p=0.003), somatic complaints (F [2, 230] = 24.06; p=0.000), and interpersonal difficulty (F [2, 230] = 5.42; p=0.005). Looking specifically for chronic pain dimensions, chronic pain intensity did not significantly predict depressed affect (β = 0.097; t [232] = 1.03; p=0.302); however, pain disability significantly predicted depressed affect (β = 0.250; t [232] = 2.66; p=0.008). Only chronic pain intensity significantly predicted anhedonia (β = 0.228; t [232] = 2.34; p=0.02), while pain disability did not significantly predict anhedonia (β = 0.008, t [232] = 0.08; p=0.937). Both chronic pain intensity (β = 0.193, t [232] = 2.13; p=0.035) and pain disability (β = 0.251; t [232] = 0.2.773; p=0.006) predicted somatic complaints. Chronic pain intensity did not significantly predict interpersonal difficulties (β=0.043; t [232] = 0.437; p=0.663), while pain disability significantly predicted interpersonal difficulties (β = 0.242; t [232] = 2.487; p=0.014).
- Effects of chronic pain on depression and sleep quality dimensions (regression analyses).
A linear combination of chronic pain intensity and pain disability significantly predicted sleep efficiency (F [2, 230] = 9.21; p=0.000) and perceived sleep quality (F [2, 230] = 20.27; p=0.000). Only chronic pain intensity significantly predicted sleep efficiency (β = 0.370; t [232] = 3.86; p=0.00), while pain disability did not significantly predict sleep efficiency (β = 0.159; t [232] = 1.655; P = 0.099). Chronic pain intensity did not significantly predict sleep quality (β = 0.181; t [232] = 1.97; p=0.050), while pain disability significantly predicted sleep quality (β = 0.232, t [232] = 2.525; p=0.012).
Structural equation modeling
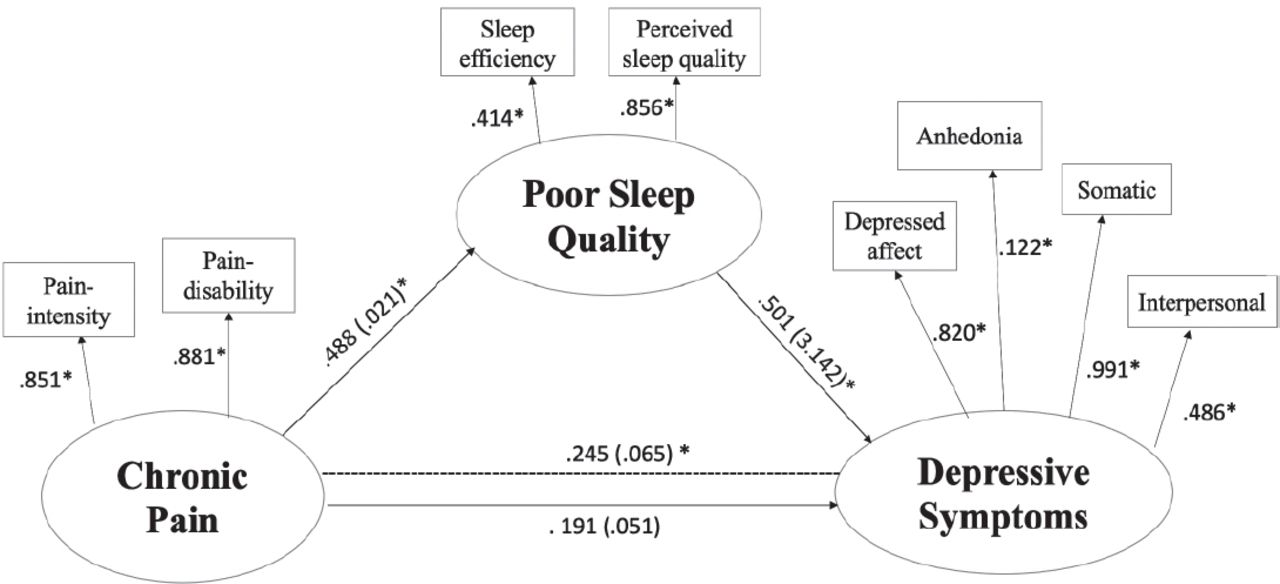
To test our hypothesis, SEM was conducted with chronic pain, poor sleep quality, and depression as latent variables. Our model adequately fit the data: χ2 (16, N=233) = 36.261, CFI=0.967, TLI=0.942, RMSEA= 0.070 (90% CI: 0.040-0.106), and SRMR=0.055; depressed affect co-varied with interpersonal difficulties. Figure 1 shows the standardized (B) and unstandardized (β) regression coefficients for each path. For all latent measures, the loadings for factor were significant (0.122-0.991). Chronic pain positively and directly affect poor sleep quality (β = 0.488; B = 0.021; p=0.00). Moreover, poor sleep quality positively and directly affect depression (β = 0.501; B = 3.142; p=0.00). In contrast, chronic pain did not have a significant direct effect on depression (β = 0.191; B = 0.051; p=0.106), but it indirectly affected depression (β = 0.245; B = 0.065; p=0.005). This analysis revealed that poor sleep quality has a full mediating function in explaining the association between chronic pain and depression.

- Structure equation modeling with the standardized (unstandardized regression coefficients.
Discussion
This study aimed to examine the extent of depression and poor sleep quality, effect of chronic pain on depression and sleep quality dimensions, and pathway by which chronic pain affects depression. Grade IV patients (high pain disability, severely limiting pain) exhibit the worst symptoms of depression and poor sleep quality. Chronic pain (namely, a linear combination of pain intensity and pain disability) predicts depression and sleep quality dimensions; yet, pain intensity and pain disability each independently predict depression and sleep quality dimension in different ways. With regard to the mechanism, chronic pain affects depression indirectly through poor sleep quality.
Our finding that 36% of chronic pain patients have depression aligns with the existing body of literature, which has shown that 22.9%-60.8% of chronic pain patients meet the criteria for depression.3,5,6 Although not every chronic pain patient has depression; patient with a higher level of chronic pain have more severe symptoms of depression. Therefore, chronic pain can be stressful, leading to catastrophizing, rumination, and helplessness48 because of pain and limited activity levels. Similarly, the existing body of literature has revealed that 40%-86% of chronic pain patients experience poor sleep quality17,18 which is in agreement with our finding that 66.1% of patients have poor sleep quality.
Although epidemiological studies highlight the association between chronic pain and advanced age, gender, and employment condition,30 some studies have revealed that age, gender, education, and occupation do not explain any differences in chronic pain.7,49 Our findings revealed no association between the patient’s background characteristics and both chronic pain intensity and pain disability. In terms of lifestyle and behavior, our findings highlighted the relationship between smoking and both chronic pain intensity and pain disability. The present finding is in agreement with the literature that reveals a positive feedback loop between smoking and chronic pain, as smoking is a risk factor for chronic pain, which could have an impact on patients’ decision to smoke.50
Our results do not support the 1-factor model for depression and sleep quality; yet, we found 4 depression and 2 sleep quality dimensions. Depression has 4 dimensions.37,51 Our findings support the heterogeneousness of depression and how chronic pain affects depression symptoms differently. Some studies have looked to the association between chronic pain and some depressive symptoms, but their findings are almost in alignment with our current findings. For instance, depressed affect is related to distress and feelings of sadness, fearfulness, anger, and chronic pain severity.52 Anhedonia is the lack of a positive effect (excitement, eagerness, and individual strength).53 A positive effect was not significantly correlated with chronic pain interference or intensity.54 Previous research did not specifically analyze the association between chronic pain and somatic complaints as dimensions of depression. Somatic complaints as a dimension of depression are not the same as chronic pain. Identifying how chronic pain affects depression dimensions is crucial for developing interventions related to depression in chronic pain patients. In terms of sleep quality, our present study revealed that sleep efficiency and perceived sleep quality are 2 dimensions of poor sleep quality, which is consistent with previous studies.46 Chronic pain intensity independently influences sleep efficiency, which is related to total sleep time. Pain disability affects perceived sleep quality, which is related to daytime dysfunction, usage of medications for sleep, subjective sleep quality, sleep latency, and sleep disturbance. Previous studies have shown that patients with chronic pain have lower sleep efficiency, and that high pain intensity predicts lower sleep quality.55
Poor sleep quality has a full mediating function in the association between chronic pain and depression because a higher level of chronic pain leads to poorer sleep quality, which, in turn, leads to worse depression symptoms. There are inconsistencies in the literature regarding this pathway. Our findings are similar to those of studies that have shown a partial29 or complete28 mediating role of sleep quality on the effect of chronic pain on depression. Although the diathesis-stress framework10 is used to test the chronic pain effects on depression, this framework does not include sleep quality. Evidence shows that chronic pain affects sleep quality9 and sleep quality affects depression.56 Our study underscores the crucial role of poor sleep quality in explaining the link between chronic pain and depression. This means that among patients with chronic pain a higher level of depression can be explained by the poor sleep quality. Clinicians can address depression by managing chronic pain, as well as assessing and treating poor sleep quality using pharmacological and non-pharmacological treatments, such as cognitive behavioral therapy.
Study limitations
First, the use of a cross-sectional design did not allow us to infer the cause-effect relationship and reverse causation. Second, using self-reported measures was not possible because it could have increased the shared method variance. Third, the study sample included a convenience sample of patients with chronic pain who were seeking treatment; therefore, the findings may not be generalized to patients who experience chronic pain but do not seek treatment or seek alternative forms of treatment. Although the sample was recruited from a government hospital to ensure that the sample represents the Saudi population, the majority of the study sample was female with a mean age of 51.32 years, and this could negatively affect the generalizability of the findings. To avoid increasing the structured interview duration, we could not consider some important factors (for example, anxiety, self-efficacy, and pain tolerance). Finally, the mediation analysis did not account for potential confounding factors that could affect the sequential ignorability assumption.
In conclusions, among chronic pain patients in Saudi Arabia, poor sleep quality and depression are prevalent issues, and this requires the assessment and treatment of both conditions. The current findings might underscore the cluster of symptoms related to chronic pain and address the need to consider the dimensions of these symptoms, not just the total score of both depression and sleep quality. Considering poor sleep quality in the context of chronic pain is highly necessary for managing depression, including its occurrence and progress. This finding can be utilized to tailor evidence-based interventions for patients in chronic pain clinics. Future longitudinal studies with larger sample sizes are needed to confirm the mediating effect of poor sleep quality.
Acknowledgment
The authors are thankful to the Research Center of the Female Scientific and Medical Colleges, Deanship of Scientific Research for funding this research and to the Deanship of Scientific Research and RSSU at King Saud University, Riyadh, Saudi Arabia for their technical support (such as English language editing).
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This research project was supported by a grant from the Research Center of the Female Scientific and Medical Colleges, Deanship of Scientific Research, King Saud University.
- Received November 29, 2020.
- Accepted February 9, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}