


Abstract
Objectives: To assess the efficacy of vancomycin powder (VP) in total knee arthroplasty (TKA).
Methods: The study design was retrospective cohort. All patients who underwent primary TKA for osteoarthritis between January 1, 2018, and March 1, 2020, in King Abdulaziz Medical City, Riyadh, Saudi Arabia were included (n=98). Of the total participants, 48 participants in the experimental group matched with 48 participants in the control group were included in the final study sample. Numerical variables are reported as means, standard deviations, and standard errors. The hypothesis was tested using the Chi-square test and independent t-test.
Results: In comparison to the control group, intraoperative vancomycin powder (VP) did not decrease surgical site infection risk in the experimental group (p=0.31).
Conclusion: We found no significant differences in the infection rates following primary TKA when using VP.
Total knee arthroplasty (TKA) has been increasingly used for advanced-stage osteoarthritis and offers surgeon satisfaction rates of 94.5% and patient of 90.3%.1 Many factors are known to cause revision TKA, including prosthetic joint infection, which is the most commonly indicated complication for revision TKA and is known to reduce successful outcomes.2 A recently adopted method for decreasing post-TKA infection and revision rate is the use of intraoperative vancomycin powder (VP).3 Although the use of systematic prophylactic antibiotics significantly decreases the risk of infection, some areas can be obstructed by hematoma or ischemic tissue after surgery. Thus, using a local antibiotic may provide a highly bactericidal environment that does not depend heavily on the systemic circulation of antibiotics.4 Vancomycin powder has been widely used in spinal surgeries as well as in joint arthroplasty and prosthesis after limb salvage. The aim of the study was to assess the efficacy of VP in TKA in our center.
Methods
This retrospective chart review study included all patients who underwent primary TKA for osteoarthritis between January 1, 2018, and March 1, 2020, in King Abdulaziz Medical City, Riyadh, Saudi Arabia. The exclusion criteria were patients who underwent primary TKA due to rheumatoid arthritis or post-traumatic arthritis, revision TKA patients, patients who had a previous infection, and immuno compromised patients. The final study sample included 48 participants in the experimental group matched with 48 participants in the control group.
All cases were performed by a single surgeon using a subvastus approach rather than a medial parapatellar approach. Patients from the experimental and control groups had betadine soap, betadine solution, and IobanTM dressing (3M, St. Paul, MN, United States) applied prior to incision. For the experimental group, 2 g of VP was applied to the joint prior to closure of the fascia, and serum vancomycin levels were measured 6 hours postoperatively. Clips were used for skin closure. All patients received 3 daily doses of postoperative antibiotics for a period ranging from 1 to 3 days, depending on the surgeon’s protocol of choice.
After obtaining approval from the Institutional Review Board (RC19/389/R), King Abdullah International Medical Research Center, Riyadh, Kingdom of Saudi Arabia, data were collected by co-authors from patients’ electronic medical records. The following variables were recorded: age, gender, body mass index (BMI), comorbidities, intraoperative VP if applied, preoperative antibiotic use, site of surgery, duration of surgery, length of primary surgical dressing, surgical site infection (SSI), the organism causing any SSI, and complications within the first 3 months post-surgery. The price of VP was SAR21 (USD5.60) per gram. Similar articles were searched for using the PubMed, MEDLINE, and Embase data bases.
Data were analyzed in 2 stages: the first stage included a descriptive analysis, wherein numerical variables are reported as means, standard deviations, and standard errors, and the second stage included hypothesis testing using Pearson’s Chi-square test and independent t-test. All data were managed in Microsoft Excel 2019 (Microsoft Ltd., WA, USA) and analyzed using SPSS v. 23.0 (IBM Corp., NY, USA).
Results
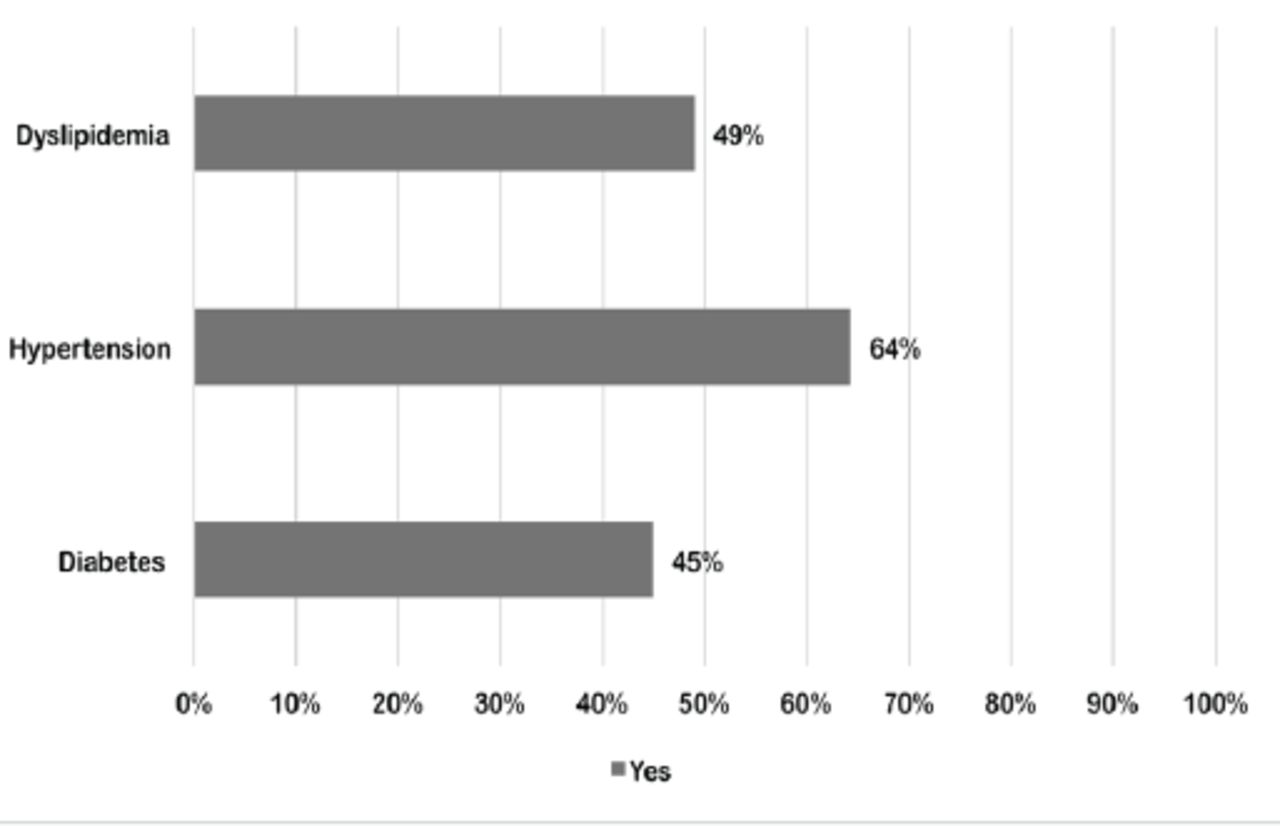
In the control group, 5 patients were aged 40-54, 32 were aged 55-69, 11 were aged 70-84 years, and 85 were aged ≥85 years. In the VP group, 2 patients were aged 25-39 years, 4 were aged 40-4 years, 27 were aged 55-69 years, and 16 were aged 70-84 years. In the control group, 3 patients were male and 46 were female. In the VP group, 13 patients were male and 36 were female (p=0.04). In the control group, 2 patients had a normal weight, 3 were overweight, and 44 were obese. In the VP group, 7 patients had a normal weight, 8 were overweight, and 34 were obese (p=0.006), as shown in Table 1. Among all study participants, the most common comorbidity detected was hypertension (64%), as shown in Figure 1.
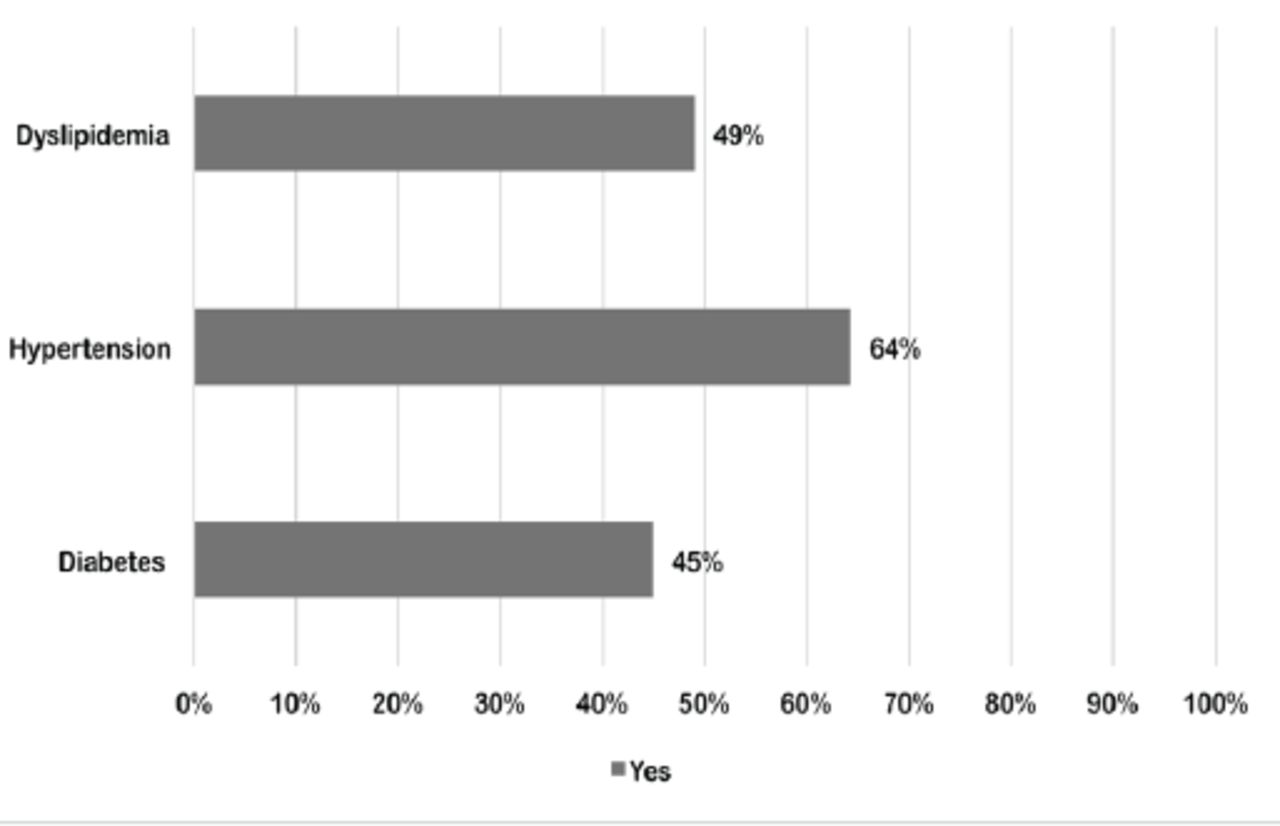
- The common comorbidities among study participants (N=98).
- Demographic characteristics of studied participants (N=98).
Surgical details.
Among patients in the control group, 26 underwent right-sided knee surgery, 17 underwent left-sided surgery, and 6 underwent bilateral surgery. Among patients in the VP group, 16 underwent right-sided surgery, 22 underwent left-sided surgery, and 11 underwent bilateral surgery. The mean duration of surgery was 128 ± 50 min for the control group and 158 ± 63 min for the VP group (p=0.061). In the VP group, the mean vancomycin level was 5.36 ± 3.56 μg/mL at 6 hours post-surgery. The mean duration of primary surgical dressing was 6.33 ± 1.31 d for the control group and 4.55 ± 2.42 d for the VP group (p<0.001). The mean duration of hospital stay was 9.18 ± 2.84 days for the control group and 8.39 ± 2.24 days for the VP group, as shown in Table 2.
- Procedure details of studied participants (N=98).
Only 2% of the patients in the control group had a deep SSI caused by multiple organisms and was treated with excisional debridement and intravenous antibiotics. Furthermore, in the control group, 2% had joint dislocation, 2% had a periprosthetic fracture, 2% had an acute kidney injury, and 2% had wound dehiscence. 6% patients from the control group underwent revision, as shown in Figure 2.
Risk of SSI
Compared to the control group, the use of VP in the experimental group showed no significant difference with respect to decreasing SSI risk (p=0.31), as shown in Table 3.
- Comparing the risk of surgical site infection between the vancomycin powder group and the control group (N=98).
Discussion
Our study found no significant difference in infection rates between the experimental and control groups in patients in whom obesity and diabetes were common. No allergic reactions or nephrotoxicity were observed in our retrospective study, which is consistent with previously published literature.4 Prosthetic joint infection (PJI) is a devastating problem in joint reconstruction surgeries; thus, many prevention measures have been used to reduce the rate of PJI, one of which is VP. Upon reviewing the literature, many recent studies on spinal surgeries have demonstrated a lower rate of SSI when using VP.5-11 Another experimental study found that the application of intrawound VP in contaminated fractures may reduce the risk of infection.12
In arthroplasties, Patel et al4 showed that the application of one gram of VP significantly reduced the infection rates in primary total hip and knee arthroplasty. However, patients received a single dose of cephalosporin within one hour before the incision. After prosthesis implantation, the surgeon applied a betadine soak in the surgical wound and then irrigated it by normal saline; therefore, Patel’s study could not determine which antibiotic or antiseptic agent was more effective at preventing infection.
Otte et al13 found that patients receiving VP in revision surgeries showed significant reduction in PJI. Dial et al3 reported a significantly lower rate of PJI in patients who underwent total hip arthroplasty and received one gram of VP before wound closure. However, their study found a significantly higher rate of chronic obstructive pulmonary disease in the control group, which may be considered a confounding variable. In addition, one patient in the control group accidentally received clindamycin instead of cefazolin, and clindamycin as a prophylactic may be associated with a higher rate of PJI.
Despite initially promising studies, others have found no effect of VP on SSI. For instance, Lum et al14 found no difference in the infection rates between the VP and control groups. Although they enrolled both total hip and TKA patients, their sample size was small. In addition, they found no difference in the revision rate and complications. Another study by Hanada et al.15 showed no difference in the infection rates between TKA and unicompartmental knee arthroplasty. In their study, they used cefazolin as a prophylactic antibiotic, and before closure, they used a bovidone-iodine solution for irrigation in both groups. Therefore, different methods for the prevention of infection were used, and we could not determine which method was most effective at reducing infection rates. However, a recent study by Butchalter et al16 assessed the effectiveness of povidone-iodine lavage with VP at reducing infection rates following primary TKA. The authors concluded that this combination may be a cost-effective method for reducing infection rates early following TKA.
Similarly, Iorio et al17 assessed the use of povidone-iodine lavage and VP in high-risk patients who underwent total joint arthroplasty. These authors defined high-risk patients as those whose BMI exceeded 40 or who were diabetic, immunosuppressed, or had undergone revision surgery. They found that povidone-iodine lavage with VP is a safe method and may reduce the incidence of infection in high-risk patients. The results of another large retrospective study by Yavuz et al18 corroborated our results of reduced infection rate. The study included 976 patients who underwent primary TKA (474 in the VP group and 502 in the control group). They followed up the patients for a minimum of 2 years after the procedure, whereas our study’s follow-up period was only 3 months.
A recent significant study by Xu et al19 found a significantly lower rate of PJI in VP-treated patients. In this study, a standard prophylactic antibiotic (cefazolin) was administered. After skin incision and prosthesis implantation, 1% povidone-iodine soak was applied, followed by irrigation with normal saline. Due to the use of different prophylactics, whether VP is useful for reducing PJI could not be determined. Moreover, in Xu’s study,19 only 9.6% of patients were diabetic, and most were non-obese.
Recently, a major retrospective study by Matziolis et al20 evaluated the use of intra-articular VP in 8,945 cases of total joint arthroplasty. Vancomycin powder was used in 1082 joints. All patients were washed with an antiseptic agent one day before the operation. A single shot of cefazolin (2 g) was administered 30 min before incision, and if the operation time exceeded 2 hours, a second dose of antibiotic was administered. These authors found that the rate of SSI was significantly lower after VP, which they attributed to the application of VP both before and after capsule closure, and any adherent powder was trapped in the subcutaneous tissue. Therefore, no aseptic wound complications were observed.
Study limitations.
First, due to its retrospective nature, selection bias may have been introduced. Second, the population size is relatively small compared with other studies. With respect to our study’s strengths, it is considered the first of its kind in Saudi Arabia; furthermore, obesity and diabetes, which are considered risk factors for SSI, were common in our study.
In conclusion, no significant differences in the infection rates following primary TKA were found when using VP, which is consistent with the recent literature. Although previous studies have reported a reduced rate of infection, our study failed to do so. Further prospective randomized trials with larger sample sizes are recommended to better assess the efficacy of VP in reducing the infection rate following primary TKA.
Acknowledgment
We would like to thank Editage (http://www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 28, 2020.
- Accepted March 15, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.